Article Text

Abstract
Objectives: To draw on empirical findings of the psychological factors that cause elementary-school children to engage in risky play behaviors that can lead to injury, with the aim of developing an integrative model that can support intervention-program planning.
Methods: An extensive review of literature on this topic was conducted, determinants of risk taking for which there was empirical support were identified, and results were synthesized to create an integrative model of children’s risk taking.
Results: Research on risk taking in children is limited, but the findings support the importance of examining child, family and socio-environmental factors to understand children’s risk-taking behaviors.
Conclusions: Development of a model outlining the determinants of risk behaviors can provide a foundation for initiatives that aim to reduce such behaviors and prevent childhood injuries.
Statistics from Altmetric.com
Unintentional injuries are a leading cause of death and hospitalization during childhood.1,2 Research examining the determinants of risk taking shows the multi-determined nature of injury-risk behaviors. The present report introduces an integrative model based on these research findings, and discusses implications for interventions that seek to reduce physical risk-taking behaviors in children 6–12 years of age. To develop the model, we reviewed published research and selected for discussion empirically supported determinants of risk taking in children, giving particular attention to factors amenable to intervention.
LITERATURE REVIEW
Journal articles written in English reporting studies of children 6–12 years of age and published from 1990 to 2005 were identified in MEDLINE, ERIC and PSYCLIT databases; reference lists of retrieved publications also were subsequently reviewed. Search terms included child* and youth crossed with each of the following terms: risk tak*, injury risk behav*, risk* beh*, risk compensation, sensation seeking and injur* risk; note: the asterisk allows retrieval of articles containing any variation of the word stem (eg, risk tak* = risk take, risk taking and risk taker). Abstracts and titles were reviewed by the authors and, after discussion (which sometimes involved reviewing the entire article), reports of empirical studies agreed upon were retrieved and reviewed. Findings were synthesized to identify unique determinants of risk taking and to develop the model reported. Illustrative studies were selected for citation (ie, the most extensive study and/or recent publication) to support the model; however, no formal criteria were used to assess the quality of the research reported.
MODEL OF THE DETERMINANTS OF CHILDREN’S RISK TAKING
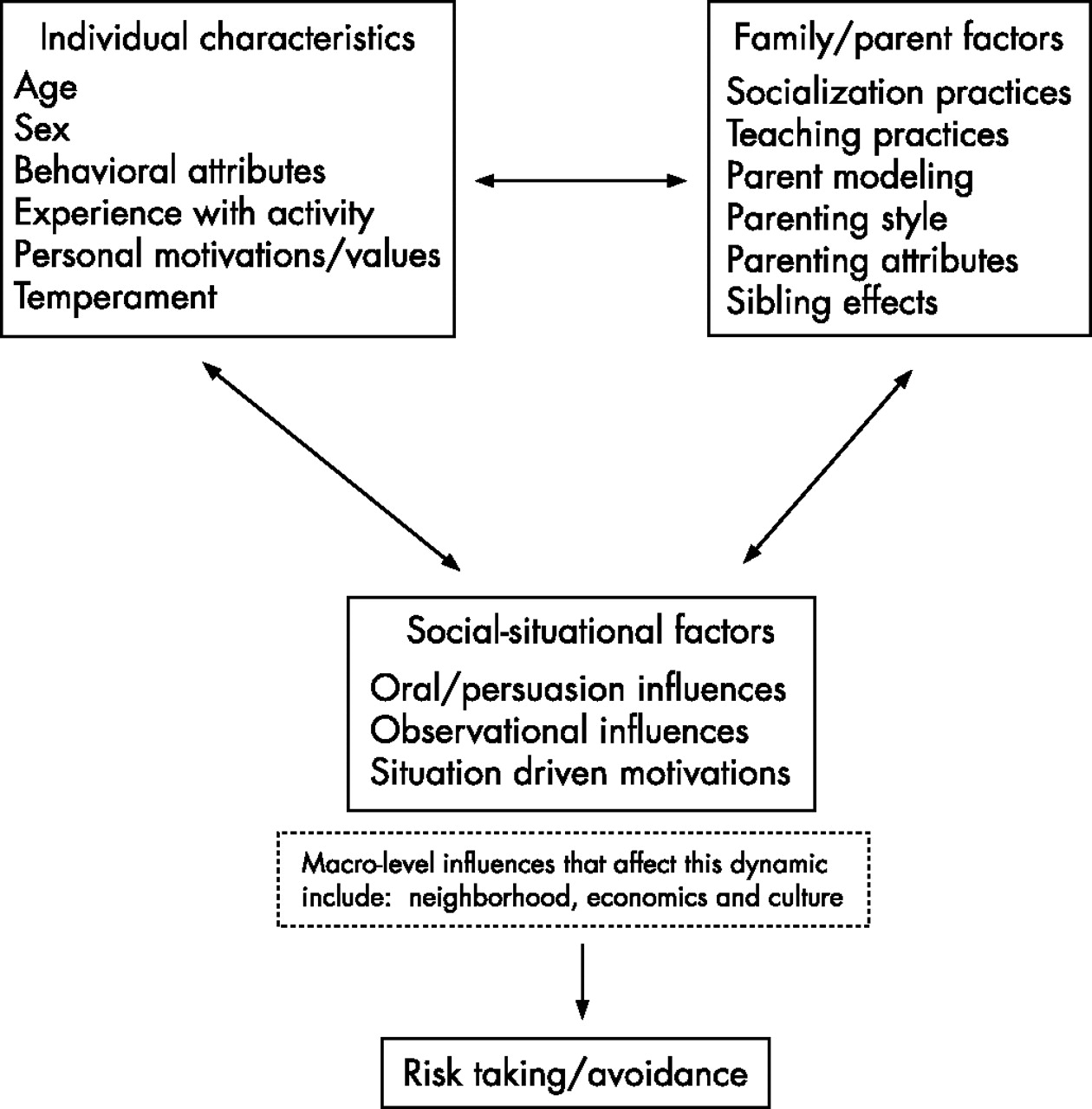
Numerous models explain risk taking during adolescence3–6; however, most are based on research investigating delinquency or risk behaviors that would not routinely apply to children of elementary age (eg, illicit drug use, alcohol consumption and unprotected sex). No such models have been developed to explain physical risk taking among elementary-school children (6–12 years of age). The accumulation of evidence during the past several years, however, now provides a foundation for the development of such a model. As shown in fig 1, children’s risk taking is a multi-determined outcome, with child, parent and social-situational factors all influencing this behavior.
{kind=link}
Empirically supported determinants of children’s risk decisions.
In the following sections, research from each of these domains of influence is reviewed, and implications of these findings for intervention programming are discussed. We acknowledge that some degree of risk taking is necessary for development, adaptive functioning and/or survival. The literature reviewed is concerned with understanding poor decision making about risk taking that increases the risk of injury. Moreover, although epidemiological data show that macro-level factors extending beyond the individual and family (eg, socioeconomics, culture and neighborhoods) also affect injury rates,8,9,10,11,12 these factors are not discussed in detail because the focus of this paper is limited to factors that are amenable to intervention programming. However, we certainly acknowledge that macro-level factors can influence children’s injuries and may affect the overall effectiveness of intervention programs. Therefore, it may be important to consider these factors when designing and evaluating such programs.
CHILD FACTORS
Children make many risk-taking decisions when they are unsupervised. It is important to understand how individual characteristics influence these decisions.
Age
There are surprisingly few studies on the developmental aspects of risk taking in children between 6 and 12 years of age. It has been shown that hazard identification improves with age,11 that older children are more optimistic than younger ones that injury will not occur,12 and that older children are more likely than younger ones to accept responsibility for resulting injuries.12 However, older children have not been shown necessarily to engage in greater risk taking than younger ones.12 Thus, what seems to matter more in predicting risk taking or avoidance are individual child attributes (eg, cognitions, temperament—see below), rather than age itself.
Sex
Sex has been shown to have a strong influence on children’s tendency to take risks, and on their injury rates. Consistent with epidemiological evidence that boys experience more frequent injuries than girls, laboratory research and studies in real-life situations show that boys engage in greater risk taking than girls.1,2,12–14 Moreover, sex is an attribute that influences how many other factors operate to affect risk taking by children. Thus, sex is one of the few factors for which interactive effects have been systematically studied. As will become evident in the remainder of this report, although boys and girls both sometimes take significant physical risks, they often have different motivations and thoughts about risk taking. Because of this, intervention programs that aim to change these underlying factors to reduce risk taking may need to be designed differently for boys and girls in order to be effective.
Cognitions
Consistent with numerous psychological models of health behaviors (eg, Health Beliefs Model15; Theory of Planned Behavior16), children who appraise danger as low, judge their personal vulnerability for injury to be low, and believe that the potential severity of injury is not great, are more likely to take risks.12,17–19 Interestingly, because of the attributions children make for injury outcomes, experiencing injuries does not necessarily alter these cognitions or lead to risk avoidance. In fact, children who attribute an injury outcome to bad luck, rather than their own behaviors, are very likely to repeatedly engage in the same behavior that led to an initial injury.17 This finding, coupled with the fact that parents assume that children do learn risk avoidance from injury experiences,20,21 may help to explain why experiencing a medically attended injury does not reduce the likelihood of children experiencing another such injury, but actually predicts future injury.22–29
Differences in injury-relevant cognitions also help to explain why boys engage in greater risk taking than girls. Girls think in terms of “Can I get hurt”, whereas boys think in terms of “How hurt might I get”.11 Boys are also more likely than girls to erroneously attribute injuries to bad luck when their own behavior is often responsible.17 Therefore, interventions that can effect changes in these cognitions could be successful in evoking reductions in risk behaviors. Such interventions have been developed for adults and adolescents.30–32 There are also recent reports of successfully changing cognitions among elementary-school children.33–35
Emotions
Children’s emotional responses in risk situations influence how they behave, and differ for boys and girls. Specifically, anticipation of positive feelings of fun and excitement leads to increased risk taking, whereas anticipation of fear leads to risk avoidance.34 Boys are more likely than girls to report experiencing fun and excitement in risk situations, which explains their greater readiness to engage in risk behaviors.18,33
These few studies are the first to document that risk decisions in children are driven not only by what they think (ie, rational processes) but also by what they feel or expect to feel when taking risks (ie, irrational processes). In fact, recent evidence shows that emotional predictors of risk decisions are statistically significant even after controlling for cognitive influences on risk taking.33 Thus, interventionists now have two domains by which they may effect changes in children’s risk taking: cognitions and emotions.
Experience
The more experience a child has with an activity, the greater tolerance for risk taking the child shows for that activity. The basis for this increased risk taking is a personal belief that they can successfully manage the increased risk.36 Grouping by age and mixing children who have low experience with those who have high experience (eg, in schoolyards, on playgrounds, on sports teams and at camps), therefore, may increase the risk for children with low experience because of the exposure to modeling of high-risk behaviors by children with greater experience (see the section Social-situational factors).
Motivations
Motivations for why children decide to engage in risk taking or risk avoidance vary with sex. Boys’ reasons for their risk decisions show that they consider fun and convenience, and often have overinflated beliefs about how effectively they can manage the risk. By contrast, girls focus more on safety concerns in deciding how to behave, which leads to greater risk avoidance.36 Interventions that target boys, therefore, may need to deal with more issues than just safety awareness.
Temperament/personality
Children who are high in impulsiveness and activity levels engage in greater risk taking and experience more injuries,37–39 although these children show no deficits in knowledge of safety or injury prevention.40 Children high in sensation seeking (ie, daring, novelty and thrill-seeking behaviors),37,41 who are oppositional (ie, non-compliant and difficult for parents to manage)42 or who overestimate their physical abilities43,44 also show greater risk taking. Sensation seeking also has been shown to lead to increased risk compensation when wearing safety gear, which means that wearing safety gear is particularly likely to lead to greater risk taking than when not wearing the gear among high sensation seekers.44 By contrast, children high in inhibitory control (ie, capacity to inhibit inappropriate behaviors) engage in less risk taking and experience fewer injuries than children low on this trait.45
Although interventions may be unlikely to effect changes in these disposition-based behaviors, identifying these children with high injury risk may prove useful for targeting increased supervision to ensure the safety of children with these behavioral attributes. In addition, recent intervention research suggests that tailoring interventions with some of these child attributes in mind can greatly increase effectiveness.46–49 Thus, screening to identify high sensation seekers41 would allow one to direct interventions to children most likely to show risk taking.33,35
FAMILY AND PARENT FACTORS
Through socialization, explicit teaching, and modeling practices, families exert a strong influence on the behaviors of their members. Surprisingly, although there is a plethora of research showing family influences on adolescent health risk behaviors (smoking,50 drinking,51 fat intake52 and seat belt usage53), studies assessing these effects on children’s risk taking are much less systematic and limited in number.
Socialization
Research on socialization practices shows that both mothers and fathers respond similarly to each other, but differently to the risk behaviors of sons and daughters. Sons receive explicit encouragement for risk taking, whereas daughters receive cautions about risk taking and about their vulnerability for injury. These socialization differences are evident as early as 2 years of age and persist through at least 8 years of age.54,55 Moreover, even when children show exactly the same risk behaviors with the same degree of competence, mothers intervene more frequently and quickly to stop risk behaviors by daughters than sons.55 Mothers are also more likely to interpret behaviors that could lead to injury in terms of safety for daughters, but in terms of discipline for sons.21
Reports by children indicate awareness of parent expectations about what would constitute acceptable risk taking, although sons and daughters respond differently to this knowledge. Daughters are more likely to comply with how they believe their parents would like them to behave, whereas sons are more likely to engage in greater risk taking than their parents would prefer.36 Girls are also more likely than boys to tell their parents about minor injuries and near-injury events, which would provide even further opportunity for parental intervention in risk avoidance for girls.17 Interventions that target increasing children’s awareness of parental or adult norms for how they should behave, therefore, may influence girls’ risk decisions, but are unlikely to have much effect on boys’ risk decisions.
Parents’ behaviors
Although parents’ teaching has been found to be the best predictor of children’s current safety practices, parents’ practices have been found to be the best predictor of how children intend to behave once they reach adulthood.56 Essentially, when parents model risk behavior while demanding safety practices from their children, they are effectively teaching children to believe that “safety is for kids”. The fact that parents’ modeling of risk behaviors can potentially have a long-term effect on their child’s risk practices suggests that interventions to reduce risk of injury in multi-generational work contexts (eg, agricultural worksites) may have to target the behaviors of senior and junior family members (eg, father and sons) to evoke reductions in risk practices.
Siblings
Older same-sex siblings also have been shown to influence the risk decisions of younger ones. Whether their intention is to promote greater risk taking or risk avoidance, older siblings are quite effective in knowing what to say to alter the decisions of their younger siblings.57 Moreover, younger siblings are particularly susceptible to the influence of their older sibling when they rate the quality of the relationship very positively. Older siblings who were boys most often focused on the value of having fun when trying to influence their younger brother. By contrast, older female siblings most often focused on safety-related issues.57 In addition, the greater the number of persuasive arguments made, the greater the success in convincing the younger sibling to change their risk decision.57 Thus, persistence by the persuader pays off, evoking change in the behavior of the persuadee.
Interventions that wish to reduce risk behaviors in children of school age, therefore, may improve their chances of success by having an older sibling communicate about risk avoidance, rather than an adult or age-mate peer with whom the target child has no or a limited personal relationship. The importance of the target child respecting and valuing the opinion of the messenger is clearly evident in these findings. Thus, if one can identify famous figures (eg, sports stars and popular musicians) who children respect and whose opinion they value, recruiting these individuals to encourage children to engage in safety practices may prove successful to promote these practices.
SOCIAL-SITUATIONAL FACTORS
Social-situational factors that influence children’s risk taking can be quite extensive and diverse. However, we have limited our focus to those for which there is empirical support.
Peers
Many have said that elementary-school children are at greatest risk for injury when they are with peers.58,59 Indeed, even by 6 years of age children are aware that boys and girls differ in risk taking, and they show different expectations for peer risk taking depending on sex of the peer.60 Oral persuasion skills are well developed by 8 years of age61; hence, elementary-school children can be considerably influenced by their friends’ endorsements to participate in high-risk activities.36,57,62–64 Children also select best friends who are highly similar to themselves in their level of tolerance for risk taking, and they know this about one another.36 These friendship choices may reinforce and further contribute to children’s already existing tendencies (due to individual characteristics and/or family and parent factors as outlined previously) to take physical risks.
These findings highlight the potential benefits of targeting dyads or groups of friends, instead of individuals, in interventions that seek to reduce children’s risk behaviors. Intervention programs that aim to instill feelings of shared responsibility for each other’s safety may prove particularly successful. Programs for adolescents (eg, drunk driving) have shown some success when they target peer groups and emphasize shared responsibility. Similar approaches could prove to be useful for reducing younger children’s risk taking. Programs that draw on peers to communicate persuasive messages about risk avoidance, particularly messages delivered by close friends, also may prove particularly successful in evoking reductions in risk behaviors. However, tailoring programs based on sex of the target audience may be necessary to achieve success.60
Children’s risk decisions are also influenced by non-oral (observational) information, which allows for peer influences among children who do not even know one another. It has been shown that if the risk taker displays a facial expression that communicates confidence (eg, smiling), then children rate the behavior as low in injury risk, whereas displaying a fearful facial expression leads to greater perception of injury risk.12 Moreover, girls assign more significance to this wary facial expression than boys, leading to greater risk avoidance by girls than boys.
These findings indicate that increased perceptions of risk may suffice to deter imitative risk taking by girls but not by boys. Exposing boys to information that more strongly communicates fear and/or potential consequences of risk taking (eg, injury experiences of age mates) may be necessary to have increased perceptions of risk translate into reduced risk taking; in fact, results of a recent intervention study provide support for this premise.66
Recent evidence also indicates that the mere presence of an observing unknown peer can lead both boys and girls to make riskier choices.35 Thus, although the quality of the relationship seems to be important for oral persuasion towards more risky choices,36 it does not seem to be as important for non-oral (observational) influences. The literature on psychological interventions contains programs aimed at developing resistance skills in order to “inoculate” against future, somewhat unpredictable, social situations that might lead one to consider increased risk taking. Drawing on theories of psychological immunization,67 the aim is to build self-awareness about feelings or thoughts that are likely to occur in social situations pressuring for increased risk taking, and to teach children to use these emotions or thoughts to evoke strategies they have learned (eg, self talk messages) to resist such pressure favoring risk taking. This inoculation approach has been shown to reduce health risk behaviors (eg, drug use, smoking and alcohol consumption) among adolescents.68–70 It may also prove useful to enhance resistance to situational pressures for risk taking among elementary-school children.
Media
Media exposure also has been shown to influence children’s behavior, particularly via television viewing. Content analyses of children’s television programs show that the frequency of injury-risk behaviors by characters far exceeds modeling of safety behaviors, and most of the risk behaviors portrayed do not result in any injuries that have substantive negative or sustained consequences for the victim.71–73 Research examining the effect of television on children’s behavior shows that exposure to programs that portray high risk taking results in greater physical risk taking in hypothetical situations.74 Similarly, exposing school-age children to an educational safety video reduces their willingness to take risks, and increases their awareness of hazards in common situations.75
The implications of these findings for interventions are clear: safety education television programming may be effective in reducing childhood risk taking and raising awareness of hazards. Policy-based interventions to mandate reductions in the modeling of risk taking in children’s programming seem likely to have an effect by reducing real-life risk behaviors.
Key points
-
Despite the importance of understanding children’s risk taking in order to develop effective interventions, no prior attempt has been made to provide an integrative synthesis of what is known.
-
Reviewing existing literature shows that children’s risk taking is multi-determined and influenced by child attributes, parent–family characteristics and social–situational factors.
-
Empirical evidence has been synthesized to create a model that provides a foundation of knowledge to support development of injury-prevention interventions.
-
Drawing on the research findings and factors highlighted in this model, numerous suggestions for interventions to reduce children’s risk taking are provided.
Immediate contextual demands
Finally, children have also been shown to shift to increased risk taking when the immediate demands of the social situation favor these behaviors. Adults tend to perform behaviors that are convenient, even though these behaviors may increase the likelihood of injury to themselves or to their children.20 Recent evidence with children showed the same effect.33 When presented different possible paths of travel that pitted distance against safety (eg, the most convenient and fastest route was the riskiest one, the least convenient and slowest route was the safest), most children endorsed taking a more risky (convenient) route than was originally planned, and cited “convenience” as the reason for increasing their level of risk taking. This shift to greater risk taking was significantly greater for boys than for girls. Children justified their endorsement of a riskier path by changing their cognitive and emotional appraisals of risk to support their new riskier choice.33 Intervention programs need to make children aware of these situational determinants of risk taking, and attempt to promote children’s resistance to such immediate situational pressures. Using the types of inoculation intervention approaches outlined earlier may help achieve this aim.
GENERAL IMPLICATIONS FOR INTERVENTION
One of the greatest challenges to injury prevention is the variety of ways in which injuries result and, consequently, the potential range of intervention strategies. On the basis of the research findings reviewed, targeting micro-level factors is essential for interventions that aim to curtail injuries by reducing risk taking during the elementary years. Specifically, the research points to a number of potential targets for intervention (ie, what the intervention aims to alter), including children’s attitudes, beliefs, cognitions and emotions. Although these targets may be more familiar to psychologists than to public health professionals, extensive research with adults and adolescents provides insights into how to evoke changes in these factors at the individual level.30–32,76–78 These findings can provide foundational knowledge on how to develop intervention programs to target these key determinants of children’s risk taking. Of course, how one intervenes and the tactics used to disseminate the intervention are likely to achieve most success by also considering more macro-level factors, such as neighborhood attributes79 (eg, neighborhood friends communicating norms about risk taking, resources available to support safe play, etc), cultural considerations80–82 (eg, culture-based differences in the value placed on risk v safe behaviors, or in attitudes about interpreting injuries as “accidents”) and economic factors83 (eg, resources available to support risk v safety practices). Thus, in developing interventions for children of elementary-school age, there is a need not only to target individual attributes but also to consider the child within the broader socioeconomic context of family, friends, neighborhood and culture in order to maximize opportunities for success.
CONCLUSION
As shown in fig 1, children’s risk taking is a multi-determined outcome that is influenced by a variety of child, parent and family, and social-situational factors, and is set within a broader context of socioeconomic and cultural characteristics. The findings from numerous studies confirm that each of the determinants shown in fig 1 individually predicts risk-taking decisions in children 6–12 years of age, and many factors interact with sex and contribute to explain why boys engage in greater risk taking than girls. Although further research is needed to determine how these factors interact to influence risk taking, our current knowledge base is sufficiently developed to support the planning of evidence-based interventions to reduce inappropriate risk taking that increases injury risk among elementary-school children.
Acknowledgments
Preparation of the manuscript was supported by grants to the first author from the Canadian Institutes of Health Research, and by a grant to the second author from the Ontario Neurotrauma Foundation.
REFERENCES
Footnotes
-
Competing interests: None.