Self poisoning with pesticides
BMJ 2004; 328 doi: https://doi.org/10.1136/bmj.328.7430.42 (Published 01 January 2004) Cite this as: BMJ 2004;328:42
- Michael Eddleston (eddlestonm{at}eureka.lk), Wellcome Trust career development fellow1,
- Michael R Phillips, executive director2
- 1Centre for Tropical Medicine, Nuffield Department of Clinical Medicine, University of Oxford, Oxford
- 2Beijing Suicide Research and Prevention Centre, Beijing Hui Long Guan Hospital, Beijing, People's Republic of China
- Correspondence to: M Eddleston, Ox-Col Collaboration, Department of Clinical Medicine, Faculty of Medicine, PO Box 271, 25 Kynsey Road, Colombo-08, Sri Lanka
- Accepted 17 November 2003
WHO's recent recommendations on reducing deaths from self harm will not help cut the high death rate from self poisoning in the Asia Pacific region
Self inflicted violence accounts for around half of the 1.6 million violent deaths that occur every year worldwide.1 About 63% of global deaths from self harm occur in the Asia Pacific region. Most of these deaths occur in rural areas, where easy access to highly toxic pesticides turns many impulsive acts of self poisoning into suicide. The World Health Organization's recent World Report on Violence and Health recommends that suicide prevention strategies focus on the identification and treatment of people with mental disorders.2 However, as impulsive self poisoning is often not associated with mental illness, this may not be the most effective approach for rural Asia.
Self inflicted violence
Self harm is a major problem in many nations in the Asia Pacific region, from the Pacific islands of Fiji and Samoa, to Asian nations as different as China and Sri Lanka.3 Suicide accounted for 71% (512 000/722 000) of all violent deaths in South East Asia and the Western Pacific region in 2000.2 Most deaths occur in rural communities: the incidence of fatal self harm in rural China is three to five times that in urban China,4 and self poisoning is the commonest cause of inpatient death in some rural Sri Lankan districts but a rare cause in the capital city.5
Suicide or fatal self harm?
Some experts believe that a distinction exists, particularly in terms of intent, between people who harm themselves (attempt suicide) and those who die (commit suicide).6 WHO's report on violence and health, however, acknowledges that, although an intent to die is a key element of suicide, determining the level of intent for an individual is difficult.2

Toxic pesticides are readily accessible in farming households of the developing world
Self harm, in particular self poisoning, is used for many reasons—to gain attention, express distress, or get revenge—not just for ending life.7 8 We think that many deaths from self poisoning in Asia Pacific occur in people who do not intend to die; they die because the poisons ingested are very toxic and patients are difficult to treat.3 9
Role of mental illness
WHO's report supports the common view that fatal self harm is always associated with a mental disorder.2 It does not consider the issue of impulsive suicides in people without mental illness. A meta-analysis by Bertolote and Fleishmann reported that 98% of fatal deaths from self harm occur in people with definite mental illness.10 But studies from China, India, and Malaysia suggest that a substantial proportion of people who die from self harm do not have a diagnosable mental illness.9 11–13
Self poisoning often occurs immediately after an acute relationship crisis not after long hours of premeditation.7 9 In one study of 326 people who had carried out serious but non-fatal acts of self harm in China,14 83% had ingested pesticides, only 40% had a diagnosable mental illness, and 35% reported that they first considered harming themselves 10 minutes or less before making the attempt.
Comparison with Britain
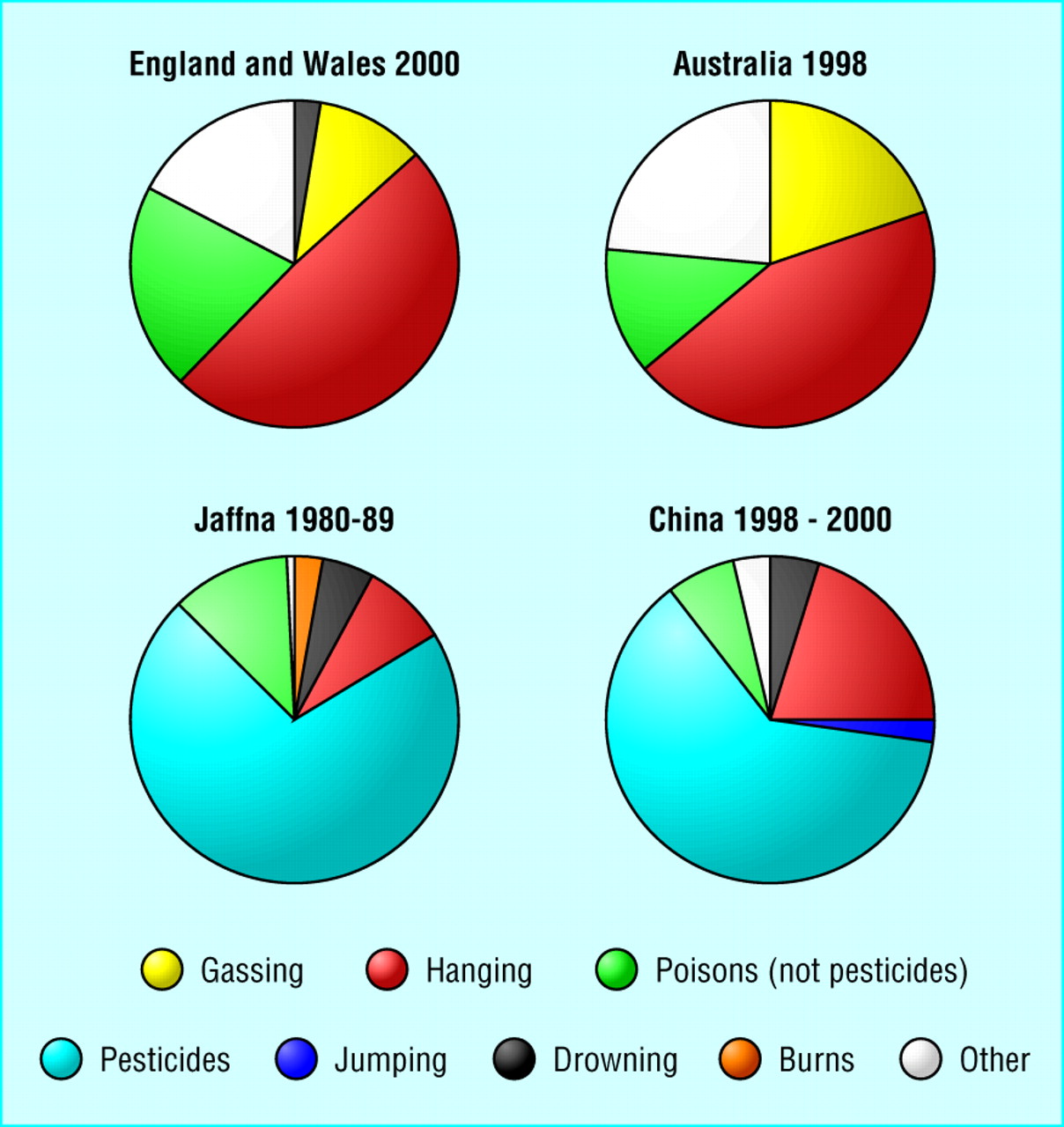
Self harm, in particular self poisoning, is common in the United Kingdom. However, most of the 3000-4000 deaths that occur each year from self harm are the result of gassing or physical acts such as hanging, not poisoning (figure).15 16 A high proportion of people who carry out such acts die, usually outside hospital. The premeditation required for these methods of self harm suggests that intent to die is high.

Comparison of methods used for fatal self harm in England and Wales, Australia, and Asia. Data for England and Wales (n=3480)w1 and Australia (n=2683)w2 are national, presenting only confirmed suicides; Data for Jaffna, Sri Lanka, (n=612) are from a review of coroner's records;w3 and for China; (n=519) from a national study9
{kind=link}
British hospitals deal with over 100 000 cases of self poisoning with medicines each year.16 Intent to die among people who self poison, unlike those who gas or hang themselves, is generally low and the case fatality very low: fewer than one in 300 people (0.3%) who reach hospital die. The poisons are not particularly toxic, effective antidotes are widely available, and medical management is simple. In 2000, only 712 people died from intentional self poisoning in Britain.w1
By contrast the case fatality for self poisoning in rural Asia is 10-20%.3 As a result, most deaths from self harm are due to poisoning and not physical acts (figure). A study from China that examined a nationally representative sample of 519 suicides found that 62% of deaths were due to pesticide ingestion and only 27% to physical methods.9 Moreover, 89% of the pesticide deaths occurred in rural farming households.9 Thus, in China alone, an estimated 175 000 (62% of 287 0004) deaths occur each year from pesticides, most in farming communities. Tens of thousands more rural deaths from self poisoning with pesticides occur in other Asia Pacific countries.
Since 1960, the Sri Lankan suicide rate has increased by over 700%.w4 This has been almost entirely due to an increase in the incidence of fatal self poisoning with pesticides because the incidence of all other methods (except plant poisoning) has remained stable.w4 w5 This rise in suicide rate has been much studied; suggested reasons include the civil war and frustration felt by educated young people because of lack of opportunity.w4 A simpler reason may be the introduction of pesticides into everyday use during the green revolution.
Medical management of pesticide poisoning
In our ongoing study of self poisoning with pesticides in Sri Lanka, 12% of patients required intubation (unpublished data). Half of the patients died and entered the suicide statistics. Many of the survivors would also have died if there had been no endotracheal tubes, laryngoscope, or doctor capable of intubating them. Such situations are common across the developing world. Patients die from aspiration or respiratory failure because doctors in small rural hospitals do not have the equipment or skills to intubate or the ventilators to support heavily sedated patients.
Essential antidotes are often lacking: atropine has been unavailable in parts of Nepal for many months (L Karalliedde, personal communication). It is impossible to manage serious organophosphate pesticide poisoning without atropine. A similar situation currently exists with yellow oleander poisoning in Sri Lanka: the lack of an affordable antitoxin means that patients must be transferred across the island to access pacing facilities.17 Many die during transfer.
Thus, the factor determining whether self poisoning is fatal or not is often medical, and nothing to do with the attempt itself (box). A parallel situation could occur in Britain if, for example, no antidote was available for paracetamol poisoning. The resulting higher case fatality for this common method of self harm would produce a substantial rise in overall suicide rate without a change in the degree of intent to die.
Recommendations for reducing deaths from self harm
WHO's report makes several recommendations to reduce the incidence of suicide—for example, improving recognition and management of mental disorders and strengthening community based support systems.2 Although these are important strategies for reducing fatal self harm globally, their ability to reduce deaths in rural Asia is questionable.
The report also suggests restricting the availability of methods for self harm (such as fencing in high bridges and restricting access to dangerous medicines or pesticides). This approach could have a rapid effect, but the report qualifies that access to pesticides should be controlled for only people “other than farmers.”2 Since over 80% of households in the developing world farm some land, most people in rural Asia would not be affected by the recommended restrictions. Indeed, most fatal pesticide ingestions occur in farming households.9
Case histories
Case 1—A 15 year old girl drank 20% paraquat after an argument and fight with her 11 year old brother. She was admitted to hospital and given Fuller's earth and supportive care. She told doctors that she had not known that it was paraquat and in her distress had simply grabbed the nearest bottle in the house and drunk from it. She died from cardiorespiratory arrest two days after admission.
Case 2—A 12 year old boy presented in a coma after drinking 200 ml of chlorpyrifos (an organophosphorus pesticide). He was intubated and transferred to intensive care, where he was ventilated for 10 days. At discharge, he told the psychiatrist that he had drunk the pesticide in front of his alcohol dependent father in an attempt to shock him and stop him hitting his mother.Seven years later, he is studying for an A level in maths.
Case 3—A 52 year old man drank 400 ml of 40% dimethoate while under the influence of alcohol. Neither his family nor friends knew the reason for his act of self harm. His Glasgow coma score on arrival in hospital two hours later was 3/15. He was intubated and given oxygen, atropine, pralidoxime, and dopamine. Although stable for four hours, he then developed bradycardia and severe hypotension. He did not respond to multiple doses of adrenalin and 200 mg of atropine and died within 15 minutes.
Primary and secondary prevention strategies relevant to the rural developing world are possible. However, pesticide regulation has to be nationwide and must apply to everyone, particularly farming households. It could include deregistering highly toxic pesticides or only allowing the use of the safer pesticide when two pesticides do the same job.18 Other methods might be to give legal authority to use pesticides to just a few people in each community (thus taking pesticides out of most households) or to provide lockers for storing pesticides away from houses so that they are not close at hand during moments of stress.
Improved medical management of self poisoning could also reduce suicide rates rapidly3 w6 since most patients with pesticide poisoning reach hospital alive.9 w7 Improvement will come from clinical research, implementation of findings into clinical practice, and improved supply of essential antidotes.
Halving the case fatality of pesticide poisoning in Sri Lanka from 20% to 10% would reduce the annual number of inpatient pesticide deaths by about a 1000. The national number of suicides would consequently fall from 4500 to 3500, a 22% reduction. Our ongoing study of the management of pesticide poisoning indicates that such a reduction is possible by using standardised protocols and good supportive care (unpublished data).
A similar reduction could be expected in China, where 59% of people who die after self poisoning receive medical treatment before dying.9 This represents 36.6% of all Chinese suicides, or 105 000 suicides annually. Thus halving the case fatality among people who receive treatment after ingesting pesticides would save over 50 000 lives a year and result in an 18% drop in the overall suicide rate.
Conclusion
Strategies to reduce the prevalence of mental illness and to increase the level of psychological and social support in rural communities should reduce the incidence of fatal self harm. However, such approaches will take time. We believe that national pesticide regulation and improved medical management will have a rapid effect possibly producing 100 000 fewer deaths a year in the Asia Pacific region alone. We hope that WHO will incorporate these approaches into its strategy to deal with this major global public health problem.
Summary points
Intentional self harm accounts for over 500 000 deaths each year in the Asia Pacific region
Around 60% of these deaths occur after self poisoning with pesticides, which is difficult to treat
Many of these acts are impulsive and will not be reduced by WHO's strategy to improve mental health services and increase community support
Regulating availability of pesticides and improving medical management could have a rapid effect on deaths from self harm in rural Asia
 References w1-w7 are on bmj.com
References w1-w7 are on bmj.com
Acknowledgments
We thank Nick Buckley, Palitha Abeykoon, David Gunnell, Mark van Ommeren, and the BMJ reviewers for their critical review, and Fahim Mohammed and Lalith Senarathna for intubation rate data and requesting consent for publication of the case histories.
Footnotes
-
Contributors and sources ME works as a clinical toxicologist in Sri Lanka and is currently performing randomized controlled trials of antidotes for pesticide self poisoning and studies of regulatory interventions. MRP is a psychiatrist and clinical epidemiologist who has worked in China since 1985. His research work involves national studies of self harm and public mental health. The impetus and evidence for this paper comes from their frequent exposure to patients with pesticide self poisoning in rural Asia.
-
Funding ME is funded by a Wellcome Trust career development grant (GR063560MA).
-
Competing interests ME is developing a randomised controlled trial with staff of Syngenta, a pesticide manufacturer, that will be funded by Syngenta. He has received no recompense for this work.