Article Text

Abstract
Aims: Death certification, a legal duty of doctors, continues to be poorly performed despite Royal College recommendations and increased education at an undergraduate level. Therefore, the current performance of certifying doctors was audited within a large teaching hospital entering the new century.
Methods: A total of 1000 completed certificate counterfoils were examined retrospectively for appropriateness of completion and the ability to construct a logical cause of death cascade.
Results: Only 55% of certificates were completed to a minimally accepted standard, and many of these failed to provide relevant information to allow adequate ICD-10 coding. Nearly 10% were completed to a poor standard, being illogical or inappropriately completed.
Conclusions: The results show no improvement in the state of certification. Possible interventions to improve outcomes are discussed; however, in light of a recent high profile legal case a current Home Office review of death certification may suggest the passing of statutory law to ensure accurate completion.
- death
- certificate
- certification
- audit
- hospital
- HIV, human immunodeficiency virus
- WHO, World Health Organisation
Statistics from Altmetric.com
Death certification, a practice with a history dating back to the 12th century, continues to be a legal obligation for a doctor attending a decedent during their terminal illness. The certificates (Medical Certificate of Cause of Death (Form 66)) are devised around the World Health Organisation's (WHO) proforma and comply with the standards and classifications of diseases set out within the International Statistical Classification of Diseases and Related Health Problems (ICD-10).1,2 The benefits of such a document are varied and include the proof of legal death, the generation of data for epidemiological studies or future health care provision, and the deterrence of crime. The previous review of death certification stated of the latter that “secret homicide has not been a significant danger at any time in the last 50 years”3; however, a recent high profile court case appears to conflict with these findings. A Home Office review is currently under way in light of these events and as such the importance of the document has been re-iterated.4
“The benefits of death certification are varied and include the proof of legal death, the generation of data for epidemiological studies or future health care provision, and the deterrence of crime”
Part of the legal obligation of a treating doctor is to complete a death certificate for the deceased in accordance with the WHO recommendations. These advisory notes are reproduced in an abbreviated form within every blank book of certificates,1 wherein a doctor is informed how to complete a certificate in a logical and appropriate manner. Should a certificate received by the registrar of births and deaths be deemed inadequate, it is the statutory obligation of the registrar general to refer the case to Her Majesty's coroner. Although a published document from the Office of National Statistics (formerly the Office of Populations, Censuses, and Surveys) suggests that most “doctors are punctilious and precise in completing” certificates,5 this fact has not been confirmed by previous studies.6–10 In fact, it appears that certifying doctors have shown no improvement over the years to such a degree that authors would appear increasingly apathetic of this fact.6,8 The Home Office has stated in its preliminary publication regarding its review of death certification that “looking again at the medical information sought on a death certificate might help address” the issue of poor performance.4 Therefore, we instigated an audit to examine the current state of certification within a large teaching hospital. We studied a large number of certificates and possible solutions to the problems were discussed.
METHOD
At certification, the completing doctor must re-iterate the information accurately upon the attached counterfoil.1 It was from this source that the information was gathered for our study. In total, 1000 counterfoils were examined from a single teaching hospital, which forms part of a large National Health Service trust. The hospital accommodates over 1100 beds, a large accident and emergency department, a children's hospital, an oncology centre, and both acute medical and surgical admission units. The certificates were examined in sequence, covering a consecutive eight month time period from October 1999 to June 2000. No cases were omitted from our study. The standard practice within the hospital is to refrain from issuing a certificate if the case is to be referred to the coroner. Thus, we are confident that none of the cases was investigated under the coronial system. We did not have access to additional information available through histology or microbiology, or any results of a postmortem examination not included on the certificate. The details of the certifying doctor were not recorded.
Information gathered from the counterfoils included age at death, the cause of death cascade, and the appropriateness of completion. The resultant information was reviewed by two histopathologists (a specialist registrar and a consultant). Initially, the certificates were assessed for contents including the presence or absence of information available through diagnostic imaging, microbiology, or histology. The usage of modes of death was also audited, a practice that has been specifically recommended against, especially if unqualified by a cause of death.1,9
Finally, all cases were allotted to one of four categories designated by the overall logicality or appropriateness of completion, including the correct use of Part II.
RESULTS
Included within the opening pages of every book of Medical Certificates of Cause of Death is a comprehensive and accurate set of instructions regarding completion of the certificate.1 However, very few completing doctors refer to this text or are even aware of its presence.11 The chapter details the duties of the completing doctor, wherein it advises that the form should be completed “to the best of your knowledge and belief” (bold in original). By using the WHO international proforma of death certification, and highlighting the terminology used within the ICD-10, it tells the doctor to identify the underlying cause of death, defined as “all those diseases, morbid conditions, or injuries which either resulted in or contributed to death and the circumstances of the accident or violence which produced any such injuries.”. The purpose of the definition is to ensure that all the relevant information is recorded and that the chain of events is completed, ultimately leading to the terminal condition. Examples are given and specificity is requested when completing, including the histopathology of a tumour, whether benign or malignant, the anatomical site, whether primary or secondary, and, for the former, the date of removal if previously excised.1,2 Malignant neoplasms were identified in 287 cases, 242 of which were entered within the Part I cascade. None of these certificates provided details of prior resection. Overall, 52 malignancies were haematological in origin, and in all cases histological information was given that allowed accurate ICD-10 coding. However, where applicable, none of these cases gave a site of origin. Of the remaining 190 cases, only 42 relayed information arising from histological examination as to the type of tumour. A total of 149 failed to site the primary tumour accurately; a further 11 gave no indication as to the primary tumour, whereas 15 stated the primary site as simply “carcinomatosis, primary unknown”. Some regard such terms as “carcinomatosis” as a mode of death.9 Thus, without the accompanying histological type and site of origin these should be deemed inadequately completed. This was not the case in this audit. It also should be noted that of the 26 that gave an accurate site of origin, nine of these stated only “prostate”, an organ that possesses only a single ICD-10 code and as such cannot be coded any more specifically.
“Old age and senility, terms used on 12 certificates, are only applicable if no other cause of death can be identified in Part I, and the patient is over the age of 70 years”
Specificity is also requested for non-neoplastic diseases, especially those of an infective origin. Bronchopneumonia is an accepted term provided that no other condition can be identified as a cause of death. This was identified in 113 cases (terms used included “bronchopneumonia”, “pneumonia”, and “chest infection”). However, 34 cases (3.4%) used the term unnecessarily, where other clearly identifiable causes were listed. Of the 289 certificates listing acute pulmonary inflammation, (notably “bronchopneumonia”, “pneumonia”, “chest infections”, and “acute exacerbation of chronic obstructive airways/pulmonary disease”), only 29 allowed accurate coding, despite the recommendation for insertion of the causative factor.2 Twenty seven of these indicated the pneumonia was aspiration induced, but only two of 289 (0.8%) identified the organism responsible (Pneumococcus pneumonia and Pneumocystis carinii). It is unlikely that only two cases were of bacterial origin or had microbiology performed. This lack of specificity is not unique to pneumonias. Septicaemia was reported in a total of 64 cases and yet in only seven (10.9%) was the causative organism named (three were meningococcal, two were pneumococcal, and two were methicillin resistant Staphylococcal aureus). Obviously, this is a continuing problem that needs to be dealt with. Little valuable information can be gained from such certificates as they stand at present.
The term cerebrovascular accident has entered medical terminology to such an extent that it is regularly used as a cause of death, although its use is not recommended because of the possible misunderstanding by uninformed relatives that a violent event led to the death.1 When used, the term should be qualified by the use of the more familiar description “stroke”. However, a total of 78 certificates used the term cerebrovascular accident unqualified and only 21 used stroke. Only four used both terms together. Notably, both terms are used for both infarction and haemorrhage within the central nervous system and therefore the type of stroke should be indicated on the form. Only 31 gave an indication as to the type of stroke (22.1%), whereas 17 accurately sited the anatomical position of the lesion within the cerebral hemispheres or hindbrain (12%). It is also unlikely that so few patients underwent imaging before death because, given the therapeutic benefits of anticoagulation in those who have suffered infarction, imaging is regarded as essential in contemporary clinical medical practice.12 Using the WHO ICD-10 method of classification, there are over 55 different codes applicable to strokes. The exact site of occlusion or haemorrhage within the cerebral vasculature can be coded, should such information be provided. Yet this information is not being relayed effectively to the registrar or the Office of National Statistics as a result of inadequate information being inserted. Therefore, national statistics of the prevalence of each type of stroke are almost certainly inaccurate.
The guidance notes also stated that modes of death—for instance heart failure, liver failure, or cardiac arrest—are unacceptable. Modes may only be used if qualified by an appropriate cause of death, although Slater believes that this is unacceptable.9 The audit identified 85 cases where a mode of death was inserted, seven of which were unqualified, and as such may be legitimately referred by the registrar general.
Old age and senility, terms used on 12 certificates, are only applicable if no other cause of death can be identified in Part I, and the patient is over the age of 70 years.1 Current reviews of certification procedures are questioning the acceptability of such a term so that it may not be suitable for inclusion in the future.4 Such cases cause problems when coding because of the lack of an appropriate code, and their inclusion provides no useful statistical information.
Five hundred and fifty cases were adequate for minimal coding purposes and provided a logical cause of death, although many did not produce the level of detail requested by the WHO. Two hundred and forty eight were logical, but lacking in simple detail—for example, neglecting to state the type of stroke or malignancy—and 93 gave a cascade that was illogical or an inappropriately completed certificate.
One hundred and nine cases used Part II inappropriately. As stated within the “notes for doctors”, “Part II should only be used when one or more conditions have contributed to death but are not part of the main causal sequence leading to death. Part II should not be used to list all conditions present at death.”.1 Despite this, such terms as “rheumatoid arthritis”, “old age”, and “osteogenesis imperfecta” were entered. Therefore, the correct use of Part II needs to be strongly re-iterated.
The remaining 93 cases were categorised as inappropriately completed or illogical in sequence design. Seven of these showed errors in cascade order, with the underlying cause of death placed in Part Ia, thus rendering the subsequent sequence incorrect. A further three cases included information suggesting that the cases should have been referred to the coroner. These included septicaemia originating from a wound infection arising from colonic surgery, a ruptured aortoenteric fistula following abdominal aortic aneurysm repair and, finally, a cardiac arrest resulting from hyperkalaemia induced by spironolactone treatment. We were unaware of all patients' clinical details or history other than those provided on the certificates. Therefore, we are unable to say whether coroner's officers, following discussions with the clinicians, rejected these patients or whether they were not reported at all. However, it remains an interesting point regarding any action we should, or should not, take under common law with respect to these cases, one that we shall continue to examine.
A single case failed to have any information written on the counterfoil, even though the certificate had been issued.
Of the cases overall, three identified hepatitis C related disease, one indicated leishmaniasis, and three indicated a human immunodeficiency virus (HIV) positive status. Two further cases suggested the presence of HIV, but failed to provide an accurate statement of this fact. Two certificates highlighted the use of smoking tobacco as a contributory factor in the cause of death, a statement accepted under Paragraph 2. Once previously the remit of the coroner, legislation was passed in 1992 following discussions between the Home Office and the coroner's working party to allow cigarette smoking to be entered on a death certificate without the need for referral to the coroner.13 Although permitted, few doctors highlight the use of tobacco, mainly because of the lack of evidence in individual cases for causation and the inherent multifactoral nature of the aetiology of atherosclerosis or carcinomas.14,15 A further concern, not highlighted previously, would be that its inclusion might initiate future legal proceedings against tobacco companies, actions that may prove insubstantial without proof of causality.
Chronic alcohol abuse, also once the concern of coroners, was indicated in a total of 13 certificates.
DISCUSSION
The results revealed that of 1000 certificates, 55% were completed logically and appropriately. However, 24.8% contained incomplete data, 10.9% used Part II inappropriately, and 9.3% were illogical or inappropriate (fig 1). Therefore, only 55% were completed in accordance with the “notes for doctors”, which states plainly that forms should be completed to the best of the doctor's knowledge. Further analysis of these certificates reveal that 62.4% (n = 270) had less than or equal to four words written in the cause of death cascade, with most only completing line Ia (n = 238). Of these, 113 were written as “bronchopneumonia” or “pneumonia”, and 34 were entered as “myocardial infarction” only.

Of 1000 certificates, 55% were completed logically and appropriately. Of the remaining certificates, 24.8% contained incomplete data, 10.9% used Part II inappropriately, and 9.3% were illogical or inappropriate.
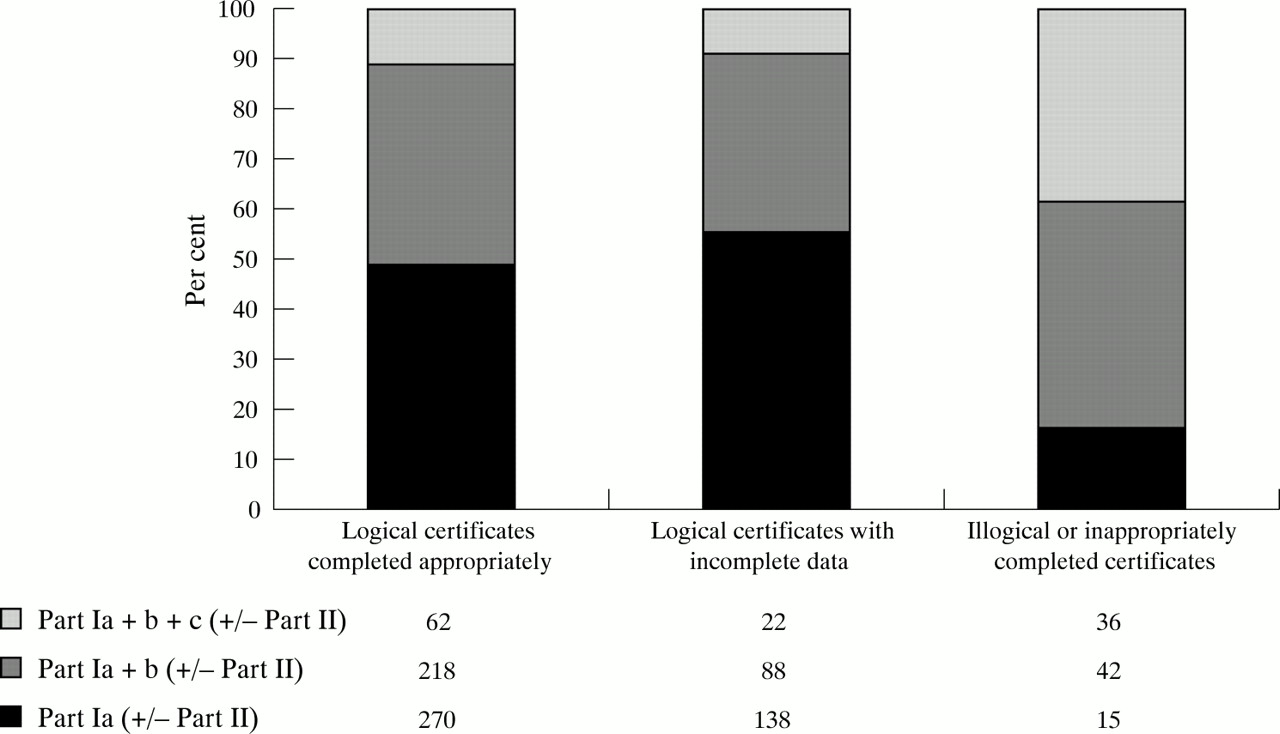
Acceptable and logical cascades were more likely to have only line Ia completed as a cause of death (270 of 550; 49.1%; fig 2). Conversely, an illogical or inappropriately completed certificate was more likely to have lines Ia to Ic completed (36 of 93; 38.7%; fig 2). This suggests that the more a doctor enters on to the certificate, the greater the likelihood of introducing an error. In 1990, the 43rd World Health Assembly adopted a recommendation for the introduction of a fourth line in Part I to allow the inclusion of more disease processes and the effects of associated therapeutic interventions.2 Countries can choose to adopt this at will, although this may result in further confusion and, given the trend for increasing errors with the greater use of lines indicated within our study, it is with great caution that any country should proceed with this recommendation.

{kind=link}
{kind=link}
The use of Parts 1a–c indicates a greater likelihood of error introduction into the cause of death cascade.
Errors may have been introduced in one or more ways. Abbreviations continue to be used, a practice that remains unacceptable during completion of the certificate.1 Ill consideration of the legality of the form may affect the accuracy of completion, although this is stated throughout the accompanying text. Less time and accuracy may have been placed on completing the counterfoil. Six cases were identified in which information that should have been placed in Part II was entered incorrectly within the Part I cascade, although the true number may have been greater given the number of certificates inappropriately completed. However, the counterfoil remains part of the legal document and as such requires an equal degree of accuracy.1
Many doctors qualify with little or no formal training in death certification or disease coding procedures, whereas others may be inexperienced or have had insufficient practice. Within the notes it is stated that certification should be carried out by a consultant, or other senior member, and that this duty should not be delegated to a junior unless he/she is closely supervised. However, the duty of death certification continues to be delegated to the more junior members of teams.6,7,16 Within Report into death certification and coroners, Brodrick stated that the process of death certification should be a duty for a senior member of the team caring for the deceased patient.3 This recommendation, although never passed as law, was re-iterated in 1982 by the joint report of the Royal College of Physicians and Pathologists,17 and is stated plainly within the accompanying text of Form 66.1 It was not within the design of our study to audit the individual doctors, thus aiming to prevent accusations of a “witch hunt”, although anecdotally seniority did not appear to affect accuracy. Most forms are still completed by junior doctors, many of whom qualified at the University of Leicester, where death certification is part of the modular course, yet inaccurate completion of the death certificates continues. The university went so far as producing a video on death certification, although the results were unimpressive.18 Some doctors may also have qualified abroad and may be unaware of these methods of certification.
“Within the notes it is stated that certification should be carried out by a consultant, or other senior member, and that this duty should not be delegated to a junior unless he/she is closely supervised”
Finally, the completing doctors may feel that they do not have enough time to complete the certificates in full detail, indicating sites and causative factors. This is also not acceptable given the legal nature of the document. The notes of the deceased are often to hand while the certificates are being written; thus, the information is readily available and yet this is not transferred to the form. It could be argued that the certificate is not being completed to “the best of (their) knowledge and belief” and as such may become a legal offence. It should be noted that the incidence of lawsuits against the medical profession arising from death certification is increasing within the USA, a trend that may well follow within the UK.19
How can we improve the standard of certification?
-
We could encourage compliance with the joint report and the “notes for doctors” at a trust level.
-
We can continue to encourage the use of the hospital necropsy; a valuable and under used examination.
-
We should encourage consultation with senior members or pathologists.
-
We can provide better education, both at the undergraduate and postgraduate level, including the teaching of foreign doctors upon initial entrance into the employment of the hospital trust.
-
The presence of the “notes for doctors” should be emphasised to clinicians.
Although further education has often been recommended as an appropriate means of remedying this state of affairs, some now believe that this is unlikely to result in the expected level of achievement.6,8 Studies in which educational interventions have been introduced have shown little or no real improvement in medical student's abilities to construct an appropriately completed certificate.18,20 Therefore, it has been suggested that greater interventions should be introduced before a second audit within the same hospital. The findings of James and Bull (1995) indicate that pathologists are less likely to make errors in certification and may be able to provide a consultation service to clinicians on a more formal basis than exists at present.16 However, in view of the current staffing conditions, the extra time required to provide this service may not be available to most.
The value of multidisciplinary team meetings is not in question. Many paediatric centres currently hold mortality meetings; a scenario that has been previously highlighted for use in adult cases.21,22 Within such meetings, necropsy findings may be relayed to the clinicians, using digital image projection facilities to complete the circle of education. This may also help to stem the rapid decline in hospital necropsy requests currently experienced within the UK,21,23 and also allow the recurring errors in certification to be highlighted.
A more labour intensive method of screening every certificate has been suggested in previous reports.8,17,24 This practice is commonplace in Finland and although it would enable the correct information to be gathered, it requires the full cooperation of not only the physicians completing the certificates, but also the pathology department. In Leicester, we aim to trial this method in the near future, using a paging system to ensure rapid turnaround of cases. This will ensure minimal delays, thus not adding to the burden of stress experienced by the relatives at such a difficult time. The service will initially be provided by a pathologist, although if it proves to be successful it may be an appropriate position for a clinical coder to adopt, given their training and intimate knowledge of ICD-10.
From the onset of our audit we were aware of previous studies examining issues similar to those discussed within this article; however, most have been outdated by the subsequent changes to the medical school curriculum that these same papers suggested. Therefore, our aim was to produce a “baseline” study into current practice, which the current governmental review could use to produce relevant recommendations and compare future changes against, and that would enable those teaching death certification practices to undergraduate students or preregistration house officers to recognise deficiencies in practice. Thus, relevant emphasis on topics may be placed in subsequent training sessions, a task that often falls to pathologists.
The initial findings of our audit appear to confirm those of previous studies and, although based only on a single hospital within a large county, it is highly likely that our findings are representative of the country as a whole.25 Although a finding of 55% completed to an acceptable standard sounds encouraging, the legality of such a document and the implications an inaccuracy could generate should be considered. It is disheartening that on entering the new millennium certification practice has failed to improve since the introduction of formal education into the medical student curriculum, or that the joint publication by the Royal Colleges has continued to go unheeded for over 18 years. Future Home Office recommendations may require the passing of statutory laws by the government to ensure a reversal of this situation, unless individual trusts tackle the problem themselves. We continue to expect that our own birth certificates have the correct names of our parents and that our marriage certificate has our partners name placed in the correct line, why should we expect any less accuracy of our death certificates?
Take home messages
-
Only 55% of the death certificates were completed to a minimally accepted standard, although many of these failed to provide relevant information to allow adequate ICD-10 coding
-
Nearly 10% were completed to a poor standard, being illogical or inappropriately completed.
-
These results show no improvement in the state of certification since the introduction of formal education into the medical student curriculum
-
Future Home Office recommendations may require the passing of statutory laws by the government to ensure a reversal of this situation, unless individual trusts tackle the problem themselves
Acknowledgments
We are most grateful for the coding information and advice provided by Ms A Pringle, Leicester General Hospital, during the completion of this audit.