Article Text

Abstract
Objectives Concussion is the most common match injury in professional Rugby Union, accounting for 25% of match injuries. The primary prevention of head injuries requires that the injury mechanism be known so that interventions can be targeted to specifically overall incidence by focusing on characteristics with the greatest propensity to cause a head injury.
Methods 611 head injury assessment (HIA) events in professional Rugby Union over a 3-year period were analysed, with specific reference to match events, position, time and nature of head contact.
Results 464 (76%) of HIA events occur during tackles, with the tackler experiencing a significantly greater propensity for an HIA than the ball carrier (1.40 HIAs/1000 tackles for the tackler vs 0.54 HIAs/1000 tackles for the ball carrier, incidence rate ratio (IRR) 2.59). Propensity was significantly greater for backline players than forwards (IRR 1.54, 95% CI 1.28 to 1.84), but did not increase over the course of the match. Head to head contact accounted for the most tackler HIAs, with the greatest propensity.
Conclusions By virtue of its high propensity and frequency, the tackle should be the focus for interventions that may include law change and technique education. A specific investigation of the characteristics of the tackle is warranted to refine the approach to preventative strategies.
- rugby
- concussion
- injury
- head
- injury prevention
Statistics from Altmetric.com
Introduction
Rugby Union is a fast-paced collision sport with a high incidence of head injury and concussion.1 2 Concussion is now the most common match injury in the professional game, accounting for 25% of all match injuries.3
Rugby Union’s governing body has been acknowledged for ‘leading the way’4 on important issues such as the formulation of an operational definition of concussion5 and its management. However, limited progress has been made to date on the primary prevention of concussion in Rugby Union.4 Until the game-specific risk factors for head injuries are established, appropriately targeted interventions to reduce the risk of head injury in professional Rugby Union cannot be developed.
The all-injury propensity of various match events has been described previously in professional Rugby Union, highlighting the tackle as the most injurious event.6 7 Two studies have conducted preliminary video analyses of tackles leading to concussion specifically, reporting that high tackles8 in senior Rugby League and poor technique 9 in high-level schoolboy Rugby Union players are significant risk factors.
To our knowledge, no large-scale video analysis study has investigated match-specific risk factors for head injuries in professional Rugby Union, though similar smaller studies exist for Rugby League,8 Australian football10 and American football.11 The aim of the present study, part of a series investigating the mechanisms of head injury in rugby, is to describe the match events leading to a head injury that satisfies the criteria for a head injury assessment (HIA) in order to identify opportunities for primary head injury prevention that may warrant more detailed analyses in the future.
Methods
This prospective cohort study was conducted between 2013 and 2015 in six major professional elite Rugby Union competitions. These were both international (Six Nations, Rugby Championship and Rugby World Cup) and national (England Premiership, Super Rugby, Top 14, Pro 12 and European Champions Cup) competitions. Ethics approval was obtained from the World Rugby Internal Ethics Committee, and all players participating in the professional leagues provided written informed consent as part of the World Rugby HIA prot ocol.
All professional competitions included in this cohort agreed (as part of the competition agreement) to adopt a standardised HIA and management protocol termed the HIA protocol.12 Operationally, the HIA protocol identifies 11 criteria 1 signs and symptoms including loss of consciousness, ataxia, convulsions and tonic posturing, which require the immediate and permanent removal of the player without further assessment. If a player experiences a head impact where the diagnosis is not immediately apparent, the team doctor is allowed to access a temporary 10 min substitution to undertake an off-field assessment using a standardised pitch-side triage tool as part of the HIA1 phase.
For this study, an HIA event was defined as any event that led to a player (a) being immediately and permanently removed from play, (b) receiving a pitch-side assessment resulting in removal from play or (c) receiving a pitch-side assessment before returning to play. Events were captured in a central database as part of the World Rugby’s HIA protocol. This database was used to identify every reported HIA over the 3-year study period. One hundred and twelve concussions reported as delayed or evolving after the match were excluded from the present analysis as they could not be directly associated to a specific match event.
A single professional and experienced game analyst coded all HIA events using a predefined coding template. The coding template comprised 15 categorical variables, describing which player sustained the head impact, the match event causing it as well as more detailed descriptions within each match event. These detailed descriptions were based on previous studies investigating injuries in professional Rugby Union.1 7 They included the players’ speed, direction, tackle type, body positions and whether the tackle was deemed foul play. For the present study, the variables analysed were match events, time of HIAs, the nature of head contact causing the HIA and HIAs by playing position.
In addition, a competition representative control group of 20 matches was coded using the same predefined coding template as the case group by the same analyst for comparison in order to calculate HIA propensity and positional differences in match activity.
Descriptive statistics (counts, averages and proportions) were used to summarise the HIA event frequency and the average match events occurring in a match. HIA propensity is expressed as the number of HIAs per 1000 events. Incident rate ratios (IRRs) were calculated to compare the propensity of two events by expressing the calculated HIA propensity relative to one another; 95% CIs were used based on the Poisson distribution and a difference was deemed to be significant if the 95% limits did not overlap.
Results
Match event
A total of 611 HIA events with acceptable video footage were identified in 1516 matches. Twenty-five HIA events were excluded from analysis because video footage was insufficiently clear to identify the mechanism of head impact.
Table 1 shows the match events responsible for HIA events, including the calculated propensity of each event to cause an HIA. The period between HIA events (in matches per HIA event for each game event) is also shown as a measure of HIA event incidence.
Match events responsible for head injuries requiring HIAs
Tackles are responsible for the most HIAs (76%) and have a significantly greater propensity (1.94 HIA events/1000 tackles) than other game events with the exception of kick contests (1.57 HIA events/1000 kick contests). As a result of having the greatest propensity and a high frequency of events per match, tackle situations result in an HIA most frequently (3.1 matches). Rucks are the second most likely game event to result in an HIA event, with a period of 20.8 matches, before a large reduction in the period for all other game events.
Within the tackle, 335 out of 464 HIAs occur to the tackler (72%), whereas 129 HIAs occur to the ball carrier (28%). Tacklers experience a more than twofold higher incident rate than ball carriers (1.40 HIAs/1000 tackles for the tackler vs 0.54 HIAs/1000 tackles for the ball carrier, IRR=2.59, CI 2.12 to 3.18).
Playing position and head injury risk during tackles
Since the tackle has the highest HIA event propensity and occurs so frequently, it was further analysed for playing position and the timing of the head impact event.
Table 2 depicts the HIA event risk during tackles for individuals of each playing position. To account for exposure to the risk event, the number of tackles made by each player within a position group is shown, along with the calculated propensity and the number of matches between HIA events to a player in each playing position.
Calculated HIA event propensity and period by playing position (tackle only)
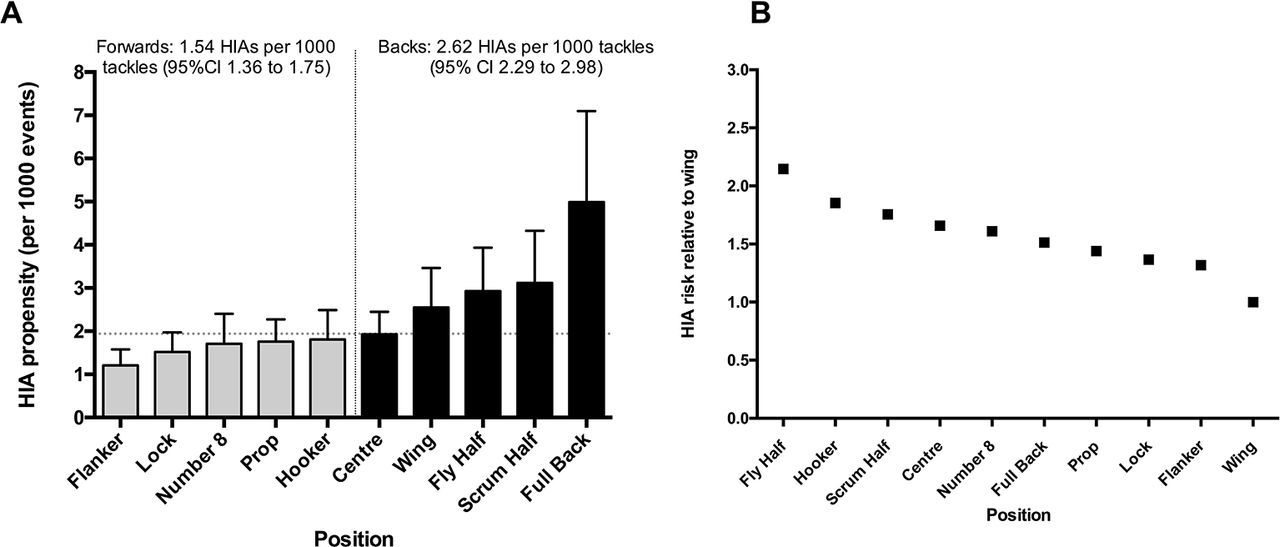
Wings have the lowest overall risk of HIA events, with one HIA event occurring in every 147.9 matches. The fly-half experiences the HIA event most frequently, though differences to other positions with the exception of wings are not significant. This is the result of the interaction between propensity for head injury per tackle and that positional group’s tackle frequency per match. Figure 1 shows the propensity for HIAs to occur during tackles (figure 1A) and the relative risk of players in each playing position relative to that of the wing (figure 1B).

Propensity for HIA events in tackles and risk by position, expressed relative to wing. HIA, head injury assessment.
Combined backs have a significantly higher propensity for HIA events during tackles than forwards (220 HIAs, 2.62 HIAs/1000 tackles, 95% CI 2.29 to 2.98 for backs; 240 HIAs, 1.54 HIAs/1000 tackles, 95% CI 1.36 to 1.75 for forwards, IRR 1.54, 95% CI 1.28 to 1.84).
Forwards sustain a greater number of HIA events in other phases of play. A total of 147 HIA events occurred in game events other than the tackle, and of these, 88 (60%) occurred to forwards and 59 (40%) to back line players.
Timing of HIA events during tackles
The timing of HIA events is shown in figure 2. There were no significant differences in the propensity of tackles to cause HIA events for the four quarters of matches.

{kind=link}
{kind=link}
HIA event propensity by match quarter. HIA, head injury assessment; Q, quarter.
Nature of head contact during tackles
Table 3 shows the HIA propensity for the tackler as a result of various types of head contact, along with the number of tackler HIA events for each contact. Data are shown for the tackler only because time constraints meant that the control cohort was analysed for the tackler only.
HIA number, propensity and proportion to tackler as a result of various types of head contact
Propensity was greatest when the tackler’s head struck the ball carrier’s head (11.3 HIAs/1000 events), followed by contact with the ball carrier’s elbow (IRR 1.78, CI 0.99 to 3.19, head vs elbow), the ball carrier’s knee (IRR 3.65, CI 2.22 to 6.01, head vs knee) and the ball carrier’s hip (IRR 6.57, CI 4.79 to 9.01 head vs hip).
The lowest propensity for an HIA event occurred for contact between the tackler’s head and the ball carrier’s upper body (IRR 24.65, CI 17.02 to 35.71, head vs upper body contact).
Head-to-arm contact, head-to-ground contact and whiplash injury were more likely to cause the HIA event in the ball carrier (table 3). For all other head contacts, the tackler experiences the majority of HIA events consistent with the overall relative proportion of impact events to the tackler and ball carrier.
Discussion
The present study is the first of a series of research studies examining the risk of significant head impacts in the sport. World Rugby’s requirement to document every HIA event in the professional game has enabled us to describe 611 HIA events so that targeted prevention strategies might be developed to reduce head injuries in the sport.13 14
Our first important finding is that the tackle exposes players to the highest risk of head injury, measured as overall proportion (76% of HIAs), propensity and incidence (table 1). This is unsurprising given previous research documenting overall injury6 15 and specifically concussion injury risk1 16 during tackling.
The tackle has been characterised previously,7 with specific reference to all injury types in Rugby Union,6 17–19 revealing that high-speed tackles,17 19 tackles where players are unsighted or off-balance,18 front-on tackles7 and high-collision forces19 were more likely to cause injury.
Similar risk factors for head injuries in tackles might reasonably be expected, and understanding these may direct interventions ranging from law modifications or enforcement to technical coaching recommendations to effectively mitigate head injury risk. This is recognised as an important area of future research based on the present finding.
The second important finding is that within the tackle, it is the tackler who is at a greater risk of injury . For every HIA event to a ball carrier, 2.6 HIA events are experienced by the tackler. This ratio differs from previous research that examined all injury types resulting from 140 269 tackles in 434 professional rugby matches, finding that the ball carrier was 1.9 times more likely to sustain an injury than the tackler (2.9 injuries/1000 tackles to the bal l carrier vs 1.5 injuries/1000 tackles to the tackler7).
It is, however, similar to a study on concussions rather than HIA events, which found a fourfold increase in the risk to the tackler compared with the ball carrier.20
This may be of significance because the current rugby laws are focused preferentially on the ball carrier, and few laws focus on the tackler. Whether law change in this regard is possible can be explored only if the specific nature of tackler injuries is better understood.
Another area that may be considered in light of this finding is the importance of technique as a contributing factor to injury risk. Previous studies, while small in size and in elite schoolboy rugby players, have found that tackles resulting in all injury and head injury had an inferior technique score than those tackles that did not result in injury.9 21 These studies were conducted in the elite schoolboy players involved in a 1 week tournament, and it may be surmised that their tackle proficiency may differ slightly from professional adults playing in a different match context, but player technique represents an important avenue for further analysis and intervention.
We found that per 1000 tackles, backs are significantly more likely to sustain head injuries than forwards. Indeed, there is a clear separation between the backline positions and the forward positions for propensity, and no forward has a risk of HIA greater than the overall tackle risk of 1.94 HIAs/1000 tackles (figure 1A).
The greater propensity for HIA events in backs is likely the consequence of the specific types of tackles made by backline players. In particular, the speed and direction of the tackle, which have been shown to predict injury risk,7 19 may be important risk factors. This too suggests the importance of tackle technique, a subject that is unexplored in professional adult rugby players, though has, as mentioned, been investigated in elite youth players.9 21 An important concept is that technique is typically taught at junior level, with less emphasis and coaching as players get older. The role of technique on HIA event risk, and the possibility of designing interventions targeted at all ages and levels of play is a topic that must be explored in future studies.
With respects to the timing of head injuries, we find no temporal changes in HIA event propensity (figure 2), a finding that differs compared with recently published observations of concussion in school-aged rugby players.20 22 McFie et al 20 found that the incidence of concussion was significantly higher in the third and fourth quarter of matches, which might be attributed to fatigue, particularly given that this study investigated school-aged players who played four or more matches in a week, possible exacerbating any fatigue effect. Alternatively, it may be the result of an accumulated tackle load where injury risk increases with each tackle.23
The reasons for an absence of such a pattern in our study is not immediately clear. Conditioning and skill levels of the professional players in our cohort may differ compared with youth and community players in a number of the aforementioned studies. It would be instructive to analyse whether injuries occur to substitutes or to players who have played the entire duration of the match, in order to determine whether playing time predicts risk, possibly even correcting for tackles made.
Our final finding was that the type of contact responsible for the most HIA events in tacklers is head-to-ball carrier head, followed by ball carrier hip and ball carrier shoulder (table 3). Head-to-head contacts also had the greatest propensity for the tackler. Of interest is that all contact types with the exception of head-to-arm, head-to-ground and whiplash injuries are more likely to injure the tackler. This invites the possibility that law or technique interventions that reduce the risk of contact between the tackler’s head and the head, shoulder and arm of the ball carrier might preferentially protect the tackler against head injury and not only the ball carrier.
It is important to recognise the difference between this group of heterogeneous head injuries that required an HIA and clinically diagnosed concussion, which have been studied previously1 2 9 20 using a descriptive epidemiological approach. The severity of the head impact event may be considered greater for concussions than for head injury events not later confirmed as concussions. This may have implications not only for understanding their occurrence, but also for interventions. For instance, McFie et al 20 found that concussion formed a greater proportion of time-loss injuries in forwards than in backs despite a similar overall proportion of non-time loss injury, which may indicate that some attribute of head injuries in forwards makes them more severe than in backs. Such possibilities may be explored by comparing head injuries that are subsequently diagnosed as concussions to those that do not meet the diagnostic criteria for concussion.
In this regard, one consideration of the present study is the variability of clinical outcomes of the head injuries included in the sample. However, our objective was to describe head impact events that would lead, at a minim um, to a pitch-side assessm ent , and at a maximum, to immediate and permanent removal confirming a concussion diagnosis. We believe this is important because the outcomes of subclinical head impacts have been speculated to be harmful, and because the HIA protocol represents a standardised and objective criteria for the identification of head impacts. If head impacts can be reduced through interventions, then the risk of concussion and the number of players exposed to potentially negative long-term outcomes of head injury will also likely be reduced. Further, future analysis may compare head impacts diagnosed as concussions to those not meeting the concussion threshold, and how they may be affected differently by various game event characteristics.
Further considerations of this study include that a single professionally employed coder performed the video analysis of all 611 head impact events. We chose to do this to eliminate any intercoder variability, and instead ensured that any ambiguous cases, where the coder was uncertain about any variable, would be discussed with another professional game analyst in order to reach consensus. The exclusion of 25 head impact events that had inadequate video footage and 112 concussions where symptoms appeared only after the match is also recognised as a limitation, since the latter in particular may differ with respects to the mechanism of injury compared with those for which video footage could be found.
Finally, with respect to the implications for management, risk reduction may focus on either the propensity of an event to cause injury or on the exposure of players to each potentially injurious risk event. For example, kick contests have a propensity that is statistically similar to that of a tackle (1.57 HIAs/1000, 95% CI 0.93 to 2.65 vs 1.94 HIAs/1000, 95% CI 1.77 to 2.12). However, 27 tackles occur for every kick contest during match play. Given the difference in frequency, it is unsurprising that the total number of HIAs in this cohort as a result of kick contests is only 14 HIA events.
While any reduction in head injuries would be desirable, the greater impact may be made by addressing the 464 HIA events in the tackle and the 73 HIA events in rucks, even though rucks have a significantly lower propensity for head injury (0.3 HIAs/1000 rucks). This can be done either by modifying the risk within a specific event or by shifting behaviour from more injurious events to less injurious events within tackles and rucks.
In conclusion, the tackle is the highest risk match event in Rugby Union, and the tackler is exposed to the greatest risk of a significant head impact event. This invites approaches to reduce the risk of head impacts that first analyses the tackle event in greater detail in order to identify high and low-risk tackle situations. After detailed analysis of the tackle has been conducted, interventions ranging from law change and reinforcement, to technique education and awareness can be considered.
What are the findings?
This study, the largest to date of its kind for rugby, describes risk factors for head injuries requiring a head injury assessment, using a cohort of 611 head injury events over 3 years in professional Rugby Union.
The tackle is the event associated with the greatest risk, both in terms of propensity (head injury events per 1000 events) and incidence (head injury events per 1000 hours).
Within a tackle, the tackler sustains 76% of head injuries, with only 24% occurring to the ball carrier.
Backline players are significantly more likely to experience head injuries than forwards.
Head to head contact is responsible for the greatest number of head injuries, with the highest propensity for injury.
How might it impact on clinical practice in the future?
A focus on reducing head injuries by better understanding and then targeting risk within the tackle situation is warranted based on the present findings.
Interventions including law change, education and technique interventions may be created to address this risk once tackle-specific risk is described.
Specific approaches to individual player positions and to minimise identified high-risk head contact types may be explored for maximum injury reduction benefit.
References
Footnotes
Contributors RT and MR conceived the study and developed the framework for video analysis. SK and MJC provided edits on the proposal, hypothesis and coding framework. BH performed the coding. RT conducted the analysis and wrote the manuscript. MJC, MR, SK and GWF edited the manuscript.
Competing interests RT, MR and BH are employed by World Rugby Pty. World Rugby is the governing body for the sport of Rugby Union and responsible for law changes in the sport. SK and MC are employees of the Rugby Football Union, which is the body that runs the sport in England.
Patient consent Obtained.
Ethics approval World Rugby Internal Ethics Board.
Provenance and peer review Not commissioned; externally peer reviewed.