Article Text

Abstract
Objectives To establish the effect of preventive measures and assert the optimal prevention strategy for acute lateral ligament injury to the ankle.
Methods An electronic literature search was employed to look for published randomised controlled trials, a controlled trials or time interventions containing research questions regarding the prevention of lateral ankle ligament injuries. Two reviewers reviewed relevant studies for strengths and weaknesses in design and methodology, according to a standardised set of predefined criteria. A total of 24 relevant studies met the criteria for inclusion and were analysed.
Results Overall taping, bracing and neuromuscular training were all effective for the prevention of ankle-sprain recurrences. The RRs of these prophylactic measures are of similar magnitude, ranging from 0.2 to 0.5 when compared with control groups. Although preventive effects have been reported in a general athletic population, evidence suggests this overall effect is due to a strong preventive effect in previously injured athletes and that any effect on fresh ankle sprains is either non-existent or very low.
Conclusions Based on these outcomes, a combination of an external prophylactic measure (tape or brace) with neuromuscular training will achieve the best preventive outcomes with minimal burden for the athlete.
Statistics from Altmetric.com
Introduction
Participation in physical activity is beneficial for health.1 For this reason, people are encouraged to participate in regular physical activities and sports. However, injuries are unwanted side effects that accompany participation in such activities. Without a doubt, the most common location of injury is the ankle joint,2 most frequently, acute lateral ligament injuries, that is sprains, which occur during forced plantar flexion and inversion of the foot.3 Individuals who suffer an ankle sprain are more likely to reinjure the same ankle,4,–,6 which can result in disability and can lead to chronic pain or instability in 20–50% of these cases.7
The high incidence of ankle sprains, the associated economic burden8 and the potential negative chronic consequences call for preventive measures. Prophylactic taping, braces, specially designed shoes and neuromuscular training (eg, balance board training) have been postulated as preventive measures against ankle sprains.9 10 Multiple reports have been published in which the effects of each of these preventive measures have been studied.
What is already known on this topic
Ankle sprains are the most common injury encountered in sports. Over the years, various preventive measures against these injuries have been proposed and tested for effectiveness, and have been the topic of multiple literature reviews. Based on current evidence, it could be stated without controversy that external measures and neuromuscular training are both effective for the prevention of recurrent ankle sprains.
What this study adds
Previous reviews only valued the scientific significance of effect studies. However, the available study outcomes also hold practical value, which is best valued alongside the scientific significance. This combined view sheds insight into the optimal prevention strategy for acute lateral ligament injury to the ankle.
The last systematic review valuing the results of studies on various preventive measures against ankle sprains was published in 2001.9 In the between years, a relatively large number of studies have been conducted and published, adding to the evidence presented in currently available reviews. More recently, two systematic reviews have been published looking specifically at the preventive effect of either external ankle supports11 or neuromuscular training.12 These recent systematic summarisations of the literature do not value the preventive effect of the various measure against each other. In addition, previous reviews only valued the scientific value of the literature. However, the available evidence also holds practical value, which is best valued alongside the scientific significance. Therefore, an updated critical review and practical appraisal of available literature is warranted to establish the effect of preventive measures and to assert the optimal prevention strategy for acute lateral ligament injury to the ankle.
Methods
Study selection
The current review is an update of a previously published critical review on the same topic.10 The same sensitive search strategy was used for the current review, identifying papers published between January 1999 and January 2009. Published studies relating to preventive measures for ankle sprains were identified using a computerised literature search in PubMed, Sportdiscus and EMBASE. Keywords used in the search were ‘ankle sprain’ AND ‘prevention’ in combination with respectively (1) brace OR bracing OR orthosis, (2) proprioception OR neuromuscular training OR training, (3) shoes and (4) tape OR taping. Reference lists of identified studies were also searched for relevant literature.
A study was included if: (1) the study contained research questions regarding the prevention of ankle sprains; (2) the study was a randomised controlled trial (RCT), a controlled trial (CT) or a time intervention; (3) the results of the study contained incidence rates of ankle sprains as study outcome; and (4) the study met a predefined cut-off score set for quality.
Quality assessment
Methodological quality of on-topic identified studies was scored using a set of 14 predefined criteria (table 1). The 14 criteria in table 1 were originally adapted from de Bie13 and Borghouts et al,14 and also applied in the previous review.10
Criteria list for the assessment of the methodological quality score of studies on the prevention of lateral ankle ligament injuries
Two reviewers (KB and EALAMV) reviewed relevant studies for strengths and weaknesses in design and methodology, according to this standardised set of predefined criteria. Each item of a selected study that met a criterion was assigned a ‘1’ (positive). If the item did not meet a criterion or was not described at all, a ‘0’ was assigned. Thus, the highest attainable score was ‘14.’ It was planned that in a consensus meeting, both reviewers would try to reach agreement on items on which they might have different opinions. If no consonance was reached, a third external reviewer should make the final decision. This latter situation, however, did not occur. In order to establish the validity and proper use of this set of predefined criteria, the inter-rater agreement, expressed as Cohen's κ, was calculated.
Studies scoring 60% or more (‘9’ or more) of the maximum attainable score were considered to be of sufficient quality and were taken into further analysis. The choice for this cut-off score was completely arbitrary, and in accordance with Verhagen et al,10 who used the same arbitrary choice of cut-off score and stated this to be the best way to make a discrimination between ‘high-quality’ and ‘low-quality’ studies.
Results
Selected studies
The previous review reported on studies published between 1980 and December 1998,10 and included eight studies.15,–,22 With the exception of the study by Amoroso et al,15 these studies were used for the current update. The outside-the-boot brace investigated in their study differs too much from the external supports used in a sports setting.
A total of 18 additional on-topic studies published between 1999 and April 2010 were found.23,–,40 These were added to the remaining seven studies of the previous review.10 This resulted in a sample 25 studies being identified as relevant: 17 RCTs,17 18 20,–,22 24,–,30 32 33 35 37 38 40 five CTs,23 31 34 36 39 two prospective cohort studies16 24 and one retrospective study.19
The method of establishing methodological quality did not differ from that in the previous review.10 Therefore, the quality of the original seven studies was not reassessed, and a score was assessed only for the additional 19 studies. The results of the methodological quality score of the 26 studies are presented in table 2. The initial agreement of the total quality assessment of the newly included trials was high with a Cohen κ of 0.92. The methodological quality score had to be adjusted for the seven non-RCT studies.16 19 23 24 31 34 36 39 For five CTs, a score could not be assessed for criterion B.23 31 34 37 40 For the other three trials, a score could not be assessed for criteria B, C and G.16 19 24 Maximal attainable scores were adjusted accordingly.
Methodological quality score of relevant studies
With 54%31 and 43%38 of the maximal quality score, two studies scored below the predefined cut-off score of methodological quality. These studies were not considered in the further analyses. An overview of the reviewed studies and their main characteristics is given in table 3.
Overview and summary of included studies
Critical review
Shoe type and/or shoe design
Four studies looked into the effect of shoe type on ankle sprain risk.17,–,19 24 It remains speculative whether shoe type has any effect on ankle-sprain incidence. Although an effect of shoe height is being mentioned, albeit contradictory, this is found in studies in which shoe height is combined with tape18 or brace.19 This leaves unresolved the extent to which shoe height might play a role in lower-ankle sprain risk. Only Barrett et al17 and Curtis et al24 directly investigated the effects of shoe design on the incidence of ankle sprains. Neither study found any difference in injury risk between different shoe designs. They suggested that shoe height does not play an important role in injury prevention, but the efficacy of shoes lies more in the newness of the footwear.17
Tape
Although taping of the ankle is arguably the most commonly used preventive measure against ankle sprains, only four studies investigated the effect for the prevention of ankle injuries.18 19 32 34 Two- to fourfold lower ankle sprain rates were found for taped ankles when compared with no preventive measures. Taping seems to be particularly effective for previously injured athletes. When compared with bracing, the effect of taping remains inconclusive. Mickel et al32 found no differences in effect, while Rovere et al19 reported braces to be more effective. Even though it remains unclear which external prophylactic method is superior from a preventive standpoint, bracing is arguably the cheaper option.
Brace
Since the previous review,10 two new eligible studies on the effectiveness of bracing have been published.33 With the exclusion of Amoroso et al's study15 for the current review, six studies on bracing remained.19,–,22 32 33 Four of these evaluated the effectiveness of a semirigid brace against a control group in a RCT.20,–,22 33 All but one study33 reported braces to be effective for the prevention of ankle sprains. RRs range from 0.15 to 0.5 between groups, in favour of the braced groups. Two of these studies also reported separately on recurrent ankle sprains in previously injured participants.21 22 Braces were found effective only for this subpopulation, thus suggesting that braces are only effective for the prevention of ankle-sprain recurrences.
Neuromuscular/proprioceptive/balance training
By far the most studies reported on injury prevention programmes, balance board training, strength training or a combination of these.16 22 23 25,–,30 33 35,–,37 39 40 RRs of ankle sprain rates range from 0.15 to 0.4 in favour of the studied preventive programme. Most studies do not report specifically on ankle sprain recurrences. However, the few studies that do so report a greater preventive effect in this subgroup and no effect for first-time ankle sprains.16 25 28 29 33 39 It seems as if proprioceptive training is the most effective part of these programmes, as strength programmes alone do not seem to be effective.33 40 A number of studies did not find any preventive effect in the studied training programme.26 27 35,–,37 It is unknown whether this is due to the content of the programme studied, whether conclusions are hampered by the scope of the outcome measures, as these studies tend to look at injuries in general and report on ankle sprains in the sideline, or whether low compliance with the studied programmes resulted in the absence of an effect. This latter is the most likely cause, while two studies that did not find any preventive effect do report a low compliance with the allocated intervention.26 27
Optimising prevention
It can be concluded from the literature that taping, bracing and neuromuscular training are all effective for the prevention of ankle-sprain recurrences. The RRs of these prophylactic measures are of a similar magnitude, ranging from 0.2 to 0.5 when compared with control groups. Although preventive effects have been reported in a general athletic population, evidence suggests this overall effect is due to a strong preventive effect in previously injured athletes and that any effect on first-time ankle sprains is either non-existent or very low. This means that, to some extent, an unpreventable ‘baseline’ ankle sprain risk exists, and current prophylactic measures are only effective from a secondary preventive standpoint.
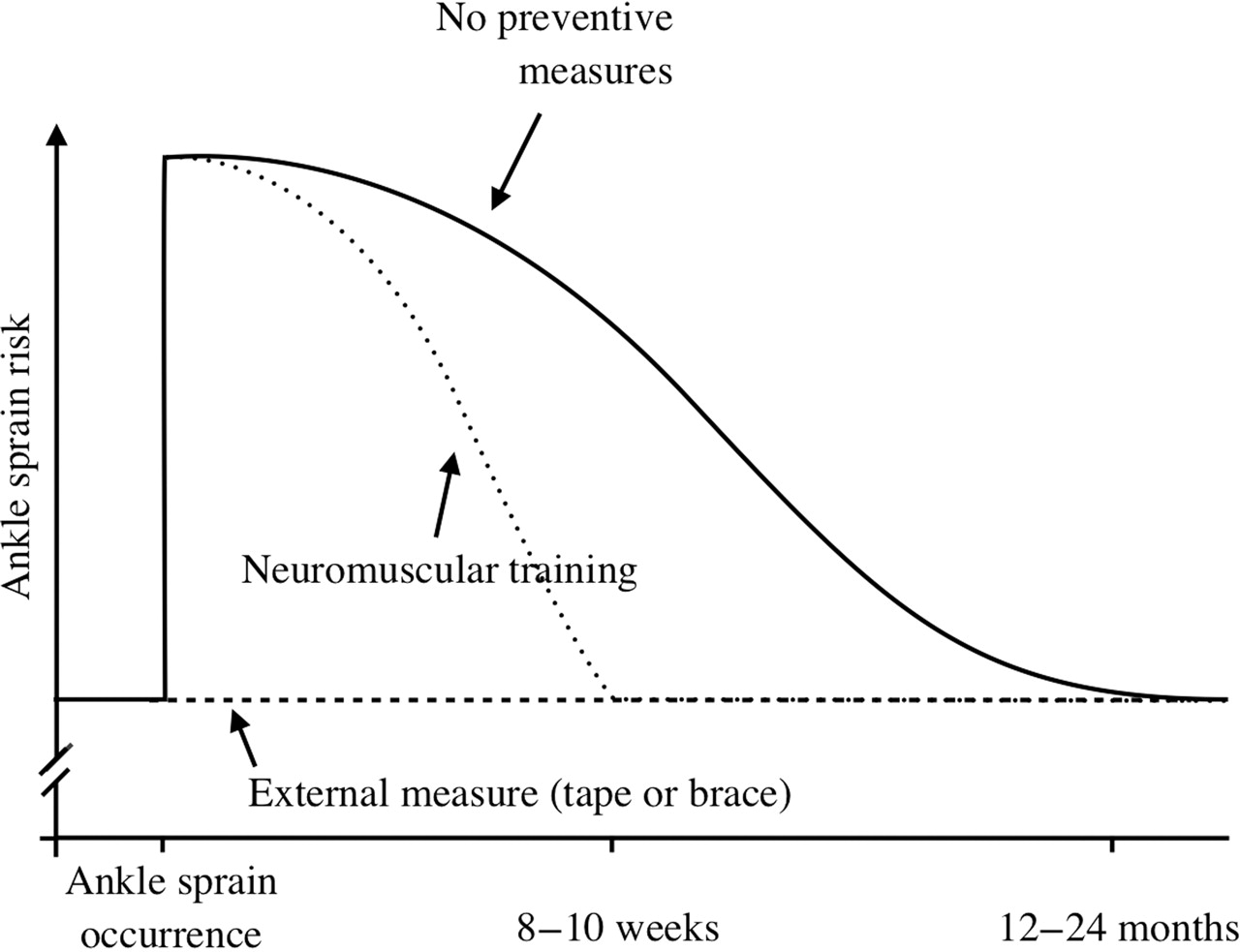
Based on these outcomes, the most practical question would then be: which measure should be preferred for the prevention of ankle sprain recurrences? Naturally, the answer to this question would be that the method that is preferred by the athlete will achieve the best results. After all, this is the measure that the athlete is most likely to actually use.41 42 However, we argue, based on current evidence, that a combination of an external prophylactic measure (tape or brace) with neuromuscular training will, in theory, achieve the best preventive outcomes with minimal burden for the athlete (figure 1).

{kind=link}
Theoretical concept for optimal ankle sprain prevention.
It has been well documented that athletes who experience an ankle sprain have a higher risk of injury recurrence postinjury.4,–,6 This increased injury risk after an initial ankle sprain is generally thought to be caused by a neuromuscular impairment in the ankle owing to trauma to mechanoreceptors of the ankle ligaments and musculature after an ankle sprain.43 Without intervention this increased injury risk gradually declines over a period of 1–2 years postinjury, until the ‘baseline’ risk level is achieved again.4,–,6 44 45 Both external prophylactic measures as well as neuromuscular training are arguably equally effective in reducing this increased risk for ankle-sprain recurrences after an index ankle sprain. However, both have seemingly different pathways through which they achieve this secondary preventive effect.
External measures for the ankle joint have originally been designed with the aim of restricting the abnormal ankle range of motion. Given the aetiology of ankle injuries, it is believed, historically, that the support system that provides the best mechanical restriction is also the system that is superior in preventing ankle injuries. However, the superior mechanical properties of braces as opposed to ankle taping do not translate to differences in preventive effects.10 46 Based on outcomes from clinical and mechanical studies, it is more likely that external measures act primarily by supporting the impaired neuromuscular function after an ankle sprain than by restricting ankle range of motion.7 10 46 The provided support is immediately available when worn, and the recurrence risk is instantly reduced to the ‘baseline’ level. Nonetheless, external measures only support the impaired ankle and do not target the underlying impaired neuromuscular function. As such, preventive effects are only available when wearing the external measure. This means that an athlete should wear the measure for the entire 1–2-year period during which an increased risk is present, in order to benefit fully from any preventive effects.
In contrast, neuromuscular training targets the underlying impairment by re-establishing and strengthening the ligament, muscles and protective reflexes of the ankle.47 48 After completion of the training, the athlete's increased recurrence risk is reduced to the ‘baseline’ level, and in theory, no further preventive means are necessary. However, these exercises do not immediately resort in a reduced injury risk after the first training session. Based on current available evidence, it takes between 8 and 10 weeks for more intensive training programmes to achieve an effect.28 29 One could say that the natural healing process is sped up.
The preventive potential of a combined use lies within the different pathways through which both measures achieve their preventive effect. External measures immediately provide preventive value, but only when worn, as they only provide support for a previously injured ankle and do not target the underlying neuromuscular impairment. In contrast, neuromuscular training targets the underlying risk increasing ‘pathology,’ but it takes some time before a preventive effect is established. When external measures are employed during the period of neuromuscular training, one benefits from an immediate risk reducing effect while targeting the underlying causes of an increased recurrence risk.
Conclusion
Over the past decade, the scientific literature regarding ankle-sprain prevention has more than doubled. The main focus of research has been on neuromuscular training, and there is still scant scientific literature on external prophylactic measures. Nevertheless, it can be concluded from the current literature that despite different preventive pathways taping, bracing and neuromuscular training are individually linked to an approximately 50% reduction in ankle sprain recurrence risk. Based on these outcomes, in theory, a combination of an external prophylactic measure (tape or brace) with neuromuscular training will achieve the best preventive outcomes with minimal burden for the athlete.
References
Footnotes
-
Competing interests None.
-
Provenance and peer review Not commissioned; externally peer reviewed.