Article Text

Abstract
Background The recent popularity of domestic trampolines has seen a corresponding increase in injured children. Most injuries happen on the trampoline mat when there are multiple users present. This study sought to examine and simulate the forces and energy transferred to a child's limbs when trampolining with another person of greater mass.
Methods The study used a computational biomechanical model.
Results The simulation demonstrated that when two masses bounce out of phase on a trampoline, a transfer of kinetic energy from the larger mass to the smaller mass is likely to occur. It predicted that when an 80 kg adult is on a trampoline with a 25 kg child, the energy transfer is equivalent to the child falling 2.8 m onto a solid surface. Additionally, the rate of loading on the child's bones and ligaments is greater than that on the accompanying adult.
Conclusions Current guidelines are clear that more than one user on a trampoline at a time is a risk factor for serious injury; however, the majority of injuries happen in this scenario. The model predicted that there are high energy transfers resulting in serious fracture and ligamentous injuries to children and that this could be equated to equivalent fall heights. This provides a clear take-home message, which can be conveyed to parents to reduce the incidence of trampoline-related injuries.
- Accident prevention
- musculo-skeletal
- paediatrics
- research
- paediatric injury
- paediatic orthopaedics
- wounds
Statistics from Altmetric.com
Introduction
Children often present to emergency departments with injuries sustained during the use of back-garden trampolines. Recent studies have recognised this and described the epidemiology of the presentations effectively, highlighting factors and themes associated with injury. These include: multiple users on the trampoline, absence of adult supervision, adult use while intoxicated, type of injury and age groups most affected.1–4
This research project was prompted by a previous prospective study of trampoline-related injuries conducted in June and July 2006 at Ninewells Hospital, Dundee, UK, which found that in the case of 50 children under 16 years old, 84% of injuries occurred on the trampoline, and in 80% of cases when there were two or more children on the trampoline.5 The publication of this research received wide media exposure and reflected a pattern seen in other work.3 5–10 Similar studies have echoed these findings; the majority of trampoline-related injuries have been shown to occur on the trampoline mat when bouncing (57–86.5%) as opposed to the more commonly assumed mechanism of injury, when a participant falls off the trampoline (9–39%).11–17 Trampoline manufacturers often state in their product literature that only one person should use the apparatus at a time. Despite this, studies continue to report high instances of individuals hurt when there is more than one person on the trampoline, with rates quoted between 64% and 83%.11 12 14–18 Studies have also revealed that the lightest person is 5–14 times more likely to be injured when multiple people use a trampoline simultaneously.1 18 These risk factors and the mechanism of injury were described over 20 years ago, when children bouncing with a second heavier individual were reported to have suffered tibial fractures as a result of a fall onto the upward recoiling trampoline mat.19
Having identified that more than one user bouncing on a trampoline is an important risk factor for serious injury; an attempt was made to illustrate transference of energy between two masses as the fundamental factor. This is important because the exact mechanism of injury is currently not clear, and only by clarifying the mechanism can further injuries be prevented. By clarifying the energy transfer involved, it will be possible to provide a clearer understanding of the guidelines for safe trampoline use, and, by communicating this in a readily accessible way, encourage concordance with the guidelines.
A number of approaches are available to better understand the interaction of trampoline users and their associated energy. A purely analytical approach employing Newtonian or classical mechanics could be adopted; a single mass attached to a spring can be completely described in this way. This becomes far more difficult with multiple masses, which are periodically not attached to the spring, and does not offer a practical solution if the behaviour of the system with respect to time is required. Another option would be to use an experimental approach; this may involve using masses dropped onto a trampoline surface or volunteers attempting to recreate the conditions of energy transfer. In both cases some means of recording motion could be used, for example accelerometers or an optical motion capture system. It would be necessary to conduct multiple experiments to adequately explore the behaviour of the system, and it would be difficult to control or separate many of the variables present. There are also obvious ethical problems of exposing volunteers to potentially injury-causing situations. An approach that lends itself to this type of problem is to model the system by computational simulation. This enables quantitative prediction and control of all the system variables, and gives visual representations of system behaviour with respect to time. Models constructed by these means range from the very simple, rigid single bodies on linear springs, to the very complex, multi-segment viscoelastic or deformable bodies on non-linear springs; the latter attempting to closely simulate real-world conditions. The usual approach is to start with a simple model and add complexity in an incremental manner, comparing model behaviour against the real world at each step. The computer simulation model reported here is a simple rigid body model, and, as such, may be considered as a first or preliminary model.
From this model, it is inferred that participants of different masses, on a trampoline at the same time, are not exposed to the same type and seriousness of injury, and that the smaller mass is subject to a greater absorption of kinetic energy. The model aims to demonstrate the forces that can affect a child of relatively smaller mass. With reference to the structure and biomechanics of bone and ligament, it aims to provide evidence for more effective awareness campaigns of the possible danger to children of unknowingly misusing this apparatus. Bone is composed of two structurally different components – cancellous and compact bone – and it therefore possesses characteristics that allow it to resist compression, tension and shearing forces.20 Cancellous bone is between 5% and 10% as stiff, and five times more deformable than compact bone, but the stiffness of bone is ultimately dependent on shape, density, where the force is applied and the rate of loading. Bone becomes stiffer and essentially stronger at higher loading rates, but, under such conditions when the structure fails, it does so at a greater load with the release of a high level of stored energy.21 The failure occurs under high energy conditions and is therefore more catastrophic, leading to the significant bony injuries seen in clinical practice. Ligaments also show an ability to stretch and store energy when the loading rate is slow, but, under a fast loading rate, ligaments become ‘weaker’ and may fail. This type of rate-dependent behaviour is termed viscoelastic. This correlates with the preponderance of fractures and ligamentous injuries noted in trampoline-related injury studies mentioned earlier.
The objective of this research is not to discourage children from taking part in an enjoyable physical activity, but to communicate to adults the risks associated with private home trampoline use and to encourage safe, enjoyable participation.
Methodology
The aim was to design a biomechanically realistic computational model of a trampoline on which two objects of different mass bounce. This would allow an animated representation of the energy transference from the larger mass to the smaller, the magnitude of the maximum force experienced by each, the rate of mass loading on each of the respective masses and the phase pattern under which these conditions were present. The parameters set for the model were determined by measurement of the surface displacement and bounce characteristics of a real-life trampoline. Similar methods have been employed to measure the characteristics of trampolines with comparable results.22
A local outdoor toy store provided their most commonly sold trampoline on which to make baseline measurements. Masses in 10 kg increments were loaded onto the centre of the 3.65 m (12') diameter apparatus, and the surface displacement of the trampoline mat was measured. Disc-shaped dumbbell free-weights (as used for body-building and weight-lifting sport) were used to provide the required incremental masses, while maintaining a consistent base ‘footprint’ not dissimilar to the area covered by a pair of human feet. A string was tied tight across the trampoline in contact with the surface of the mat at rest, to represent the mat's unloaded position. The downward mat displacement was measured with a measuring tape rule from the centre of the mat's surface, beneath the added mass, to the taught string above. The displacement was double-checked by measuring the distance between the underside of the mat and the ground below. Figure 1 demonstrates that there was an approximate linear relationship between the mass in kg and the surface displacement in cm. The gradient of the line quantifies the stiffness K (elasticity) of the system. The stiffness calculated from figure 1 was 3.60 N/mm.

Displacement (cm) of surface of 3.65 m trampoline by mass (kg).
A local high school allowed trained supervision of their trampolines in order to film people of three different masses (30 kg, 37 kg, and 90 kg) bouncing individually for a short period of time. This gave a realistic measurement of the height of bounce of people of different masses and the time it took for a bouncing mass to decay to 0. In addition, the 90 kg person also bounced with a tethered 20 kg mass. This showed the pattern of bounce of a smaller mass and the point in the phase at which there was visible energy transference from the larger mass as the smaller mass ‘took off’. The stiffness (K) of the trampoline surface was calculated using the equation,
where F is frequency in cycles per s (Hz), K is stiffness in Newtons/mm (N/mm) and m is mass in kg. With a 90 kg mass and an observed frequency of 0.94 Hz (under conditions where the mass did not leave the surface of the trampoline), K was calculated to be 3.14 N/mm. This is close to the more directly measured value of 3.60 N/mm for K determined from figure 1. The direct measurement was used in the model, as the equation assumes perfect simple harmonic motion. In reality, a trampoline is a more complex system where the mass does leave the trampoline surface, and the relationship between mass, stiffness and frequency will deviate from that described by equation 1.
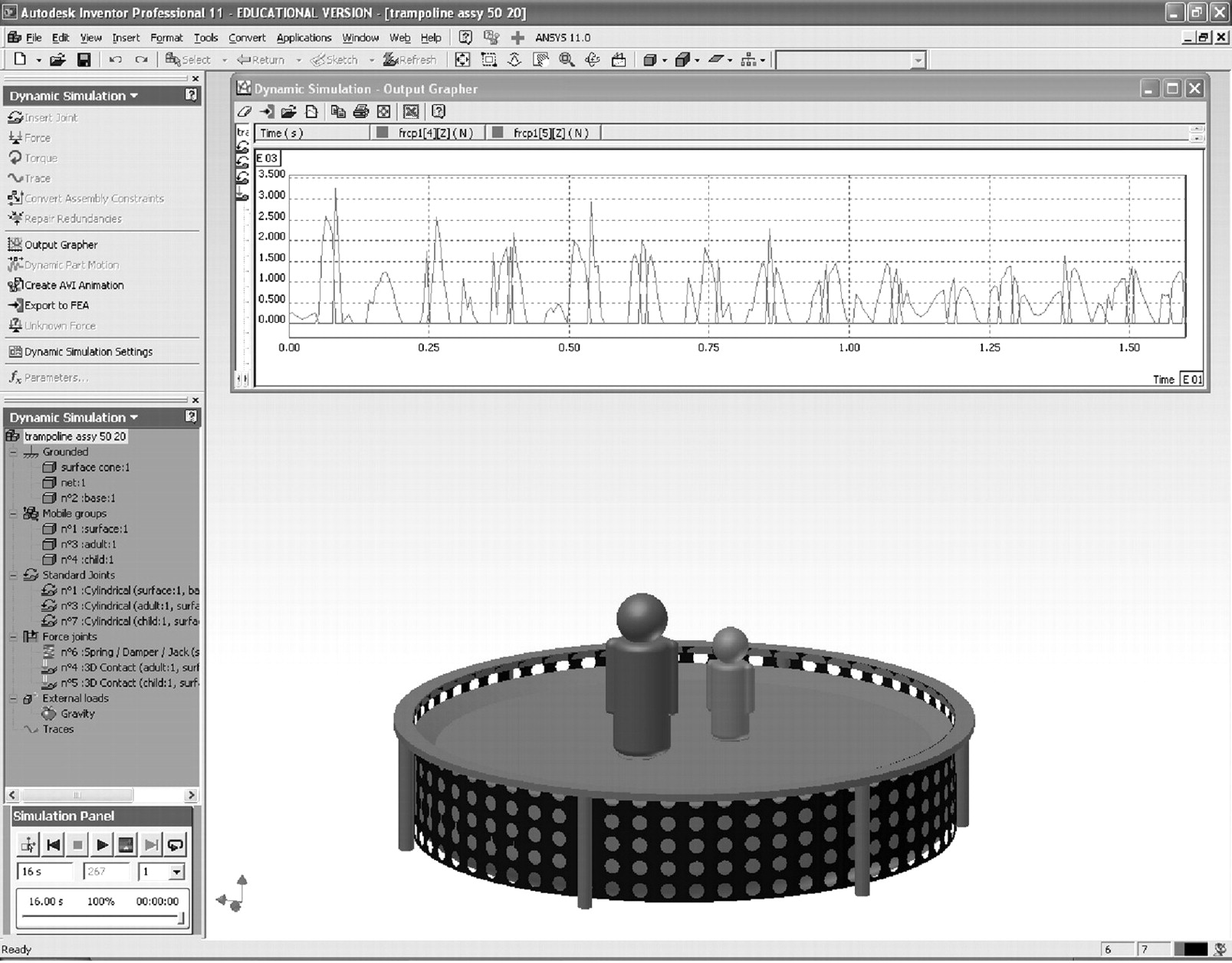
The model was created in Autodesk Inventor v11 dynamic simulation application. This is a rigid body modeller, which means that it was unable to replicate the more complex variable surface of a real trampoline or the complex behaviour of a deformable viscoelastic human body bouncing on the trampoline. Figure 2 shows a still image of the model.

Image of model by Autodesk Inventor v11 with adult and child masses.
The initial condition of the model is where the system is at rest and then an adult mass is dropped from a height of 1.2 m onto the trampoline. The adult and child are single rigid masses and are constrained to move along a predetermined vertical axis and the trampoline surface is flat and rigid, but elasticity is provided by a linear spring element. In reality, trampoline mats are fabricated with relatively non-elastic materials woven from waterproof canvas or polypropylene webbing. The bounce factor and mat displacement are usually due to the action of the trampoline's metal springs, which link the mat to the frame, rather than properties of the mat itself. The spring stiffness of the model is based on measurements from real trampolines (using K value determined from figure 1). No extra energy or forces were applied during the simulation run time, but a small damping factor was applied to the spring element to speed up simulation processing and to aid model stability. A realistic damping factor would be much larger, but, if applied, would necessitate the system to be topped up with energy every cycle (bounce) as happens in the real world by a person pushing off the trampoline.
Results
The model demonstrates that the small mass of a child's body undergoes unexpectedly large forces if using a trampoline with someone of a significantly greater mass. The model made predictions on combinations of masses where the larger mass was between 1.67 and 5 times that of the smaller mass. Individuals of differing mass bounce asynchronously, and it is during periods of mismatched phase of bounce that these transfers of energy are most significant.
The model was set to run with ‘adult’ masses of 50, 65, 80 and 100 kg with ‘children's’ masses of 20, 25 and 35 kg. As well as the greater absolute forces to which the child is subjected with the larger mass, the rate of loading is also quicker when the difference between the two masses is greater. This has implications for the mechanism of injury, which will be discussed later.
The smaller child mass often experiences greater force over a shorter time (often taller and narrower upward spikes) compared to the adult mass, demonstrating the difference in energy transfer and rate of loading.
The energy transfer to the child was translated into equivalent fall heights. This is a graphical and demonstrable calculation of the kinetic energy that is transferred to the child (figure 3). The model predicted that an adult of 80 kg bouncing with a 25 kg 8-year-old could generate forces of about 4kN on the child, which is equivalent to the child falling 2.8 m.

Forces generated by an 80 kg adult mass and 25 kg child mass and relative height.
Table 1 summarises the predicted fall height for children of various masses when bouncing with an 80 kg adult.
Equivalent fall heights of energy transferred to children of various masses by an 80 kg adult
Discussion
The present theory suggests that when there are multiple users on a trampoline, bouncing out of phase, there can be a transfer of energy from the larger to the smaller mass, or person. This model supposes a closed or constant system of energy, which can be summarised as in figure 4. In a mechanical system, potential energy refers to the gravitational force that acts on an object. Other forces that act on the object can be termed ‘applied forces’. Kinetic energy refers to the energy that the object possesses due to its motion.23 At times during the bouncing phase there is a net transfer of kinetic energy (KE1) from the larger mass to the smaller mass, and the smaller mass then has a disproportionately large amount of kinetic energy (KE2). Therefore, if M2 at the nadir of the bounce on the trampoline is conferred KE1 from M1, KE2 is increased, resulting in transferred force to the musculoskeletal system (in the case of human subjects).

{kind=link}
{kind=link}
{kind=link}
{kind=link}
Trampoline model of two users of different masses. KE, kinetic energy; PE, potential energy; M, mass; M1, larger or adult mass; M2, smaller or child mass; SE, strain energy in the spring; C is constant in the closed system of energy.
In this type of physical system, frequency of bounce is determined by two things: spring stiffness and mass. Spring stiffness is, of course, fixed, but if there are two unequal masses within the system the relatively smaller mass will have a higher frequency of bounce than the larger one. Consequently, at some point in time they will cross, even if they start completely out of phase. In effect, the smaller mass will catch up with the larger one, and when this happens the energy transfer effect can occur (especially if it happens at the point in the cycle where the larger mass has just transferred all of its energy to the trampoline). Equation 1 describes this relationship between mass and frequency.
Gymnastic sport trampolining has a recognised technique known as ‘kipping’.24 A coach can apply their own mass to the trampoline surface deliberately to provide a degree of pre-tensioning and then recoil, which is done at the same time as the gymnast lands prior to their next move. This kipping technique provides a significantly greater uplift for the gymnast in a controlled and predicted manner.
With multiple users on a domestic trampoline the transfer of kinetic energy is uncontrolled and unintentional. Depending on the point in the phase at which this happens, the child may experience an increased height of bounce (as with the kipping effect), or, if it happens when the child and adult are out of phase, the child will land on a hard surface that is coming up to meet them and for which they had not prepared by flexing their knees and hips, injuring the soft tissues or bones of their ankle or lower leg. If the child lands on its outstretched hands, energy is transferred and may result in supracondylar fractures of the humerus. The pattern of force transference – influenced by the position of the subjects' joints at the time of impact – also determines if injury to the bones or ligaments takes place. As there are no other applied forces acting in this system, there is only potential and kinetic energy. The sum of potential and kinetic energy is mechanical energy, and, when there is no other work done by applied forces, the mechanical energy is constant or conserved and is fully transmitted to the limbs of the smaller child. The model followed these rules, which allowed a prediction of equivalent fall heights for children jumping on a trampoline with an 80 kg adult. Depending on the child's mass, the energy transfer may be equivalent to the child falling between 2.2 m and 3.4 m, causing injuries similar to those expected from a drop from a first floor level.
This model provides a helpful and illustrative method of appreciating the forces involved in these injuries. However, due to several simplifying assumptions made in the model it is not entirely representative of the real-life scenario. These assumptions include:
A rigid, non-deforming trampoline surface (real trampoline mats are not elastic, they are not designed to stretch. The elasticity is provided by the springs, which attach the mat to the frame; however, the surface does undergo large deformations).
Unrealistic level of damping.
No work input from adult or child to maintain energy or alter energy present within the system.
Constrained motion of adult and child along a fixed vertical axis.
The human body as a rigid single mass not a multi-linked segment system with viscoelastic properties.
Nevertheless, the behaviour of the model was very similar to the experimental observations made and it is reasonable to conclude that it is useful in approximating the forces and behaviour of a trampoline human-mass system and therefore useful to raise awareness of the dangers.
McDermott et al highlight that current safety guidelines as recommended by the American Academy of Pediatrics and the Consumer Product Safety Commission of the United States are not being followed and more effective guidance and education is needed for parents.17 Adherence to guidelines in the UK is also poor, but the findings from this study help illustrate the potential danger involved. This will aid clearer and more precise explanation of the synergistic forces acting on a child who uses a trampoline at the same time as another user. During discussion with parents who have brought their children to the emergency department, it would appear that many trampolines have been purchased with the intention of simultaneous multi-person activity, due to a miscomprehension that a large domestic trampoline has been designed for such use. Recommendations of this project include communicating the danger of improper trampoline use to parents by giving an easily understandable comparison (falling from a defined height) to the types of forces acting on a child. It is aimed to use these findings to stress the guidelines of trampoline use as outlined by the Royal Society for the Prevention of Accidents, and, in particular, the message of ‘one at a time’.1
This project can now be taken forward and the simulation developed, with the intention for the next phase to model events around the impact with the trampoline mat and to examine the loading forces on children's limbs.
Acknowledgments
Mrs Emma Rudman, Physical Education teacher at the High School of Dundee, Dundee. Active Kids Toys and Adventure Park, Stanley, Perthshire. Professor Rami Abboud, Head of Department of Orthopaedic & Trauma Surgery and Director of the Institute of Motion Analysis and Research, Tayside Orthopaedic and Rehabilitation Technology (TORT) Centre, Dundee.
References
Footnotes
Competing interests None.
Provenance and peer review Not commissioned; externally peer reviewed.
Linked Articles
- Primary survey