Article Text

Abstract
Violence continues to grow as a priority for public health practitioners, particularly as its causes and consequences become better understood and the potential roles for public health are better articulated. This article provides the context to “Violence: a glossary (part 1)” published in the last issue of this journal, and updates some of the data, concepts and population approaches presented in the 2002 World report on violence and health. The paper addresses the following questions: What is the magnitude and global burden of injury from violence? What causes violence? Is resilience important? What is the role for public health? What are the key challenges and opportunities? We aim to engage the general reader and to increase understanding of violence as a potentially preventable issue.
- violence
- public health
- prevention and control
- intentional injury
Statistics from Altmetric.com
The 2002 World report on violence and health (WRVH), published in multiple languages and widely distributed and cited,i has ensured that violence, and its multifaceted causes, consequences and responses, can no longer be neglected. The WRVH sought to promote a public health, rather than a clinical or legal, response to violence and challenged practitioners and policy-makers not just to focus on the interface between the parties engaged in violent conflict but to examine the wider socio-political and economic contexts of violence.
This article provides the context to “Violence: a glossary (part 1)” published in the last issue of this journal. We update some of the data, concepts and population health approaches presented in the WRVH. Our aim is to interest the general reader and to stimulate further engagement with the public health response to violence.
The paper addresses the following questions:
-
What is the magnitude and global burden of injury from violence?
-
What causes violence?
-
Is resilience important?
-
What is the role for public health?
-
What are the key challenges and opportunities?
WHAT IS THE MAGNITUDE AND GLOBAL BURDEN OF INJURY FROM VIOLENCE?
Mortality
Violence is among the leading causes of death for people aged 15–44 years.1 In 2000, it was estimated that 1.6 million people worldwide died as a result of violence, an overall age adjusted rate of 28.8 per 100 000. Nearly half of these deaths were suicide, one third were homicides and about one fifth were war related.2
The effects of violence are disproportionately felt by low and middle income countries, in which more than 90% of all violence-related deaths occur.3 In African and Latin American regions, homicide rates are nearly three times higher than suicide rates, while in European and South East Asian regions there are twice as many suicides as homicides.1 Males account for 77% of all homicide deaths, particularly males 15–29 years of age.1 Males also predominate among suicide deaths. Globally, rates of suicide increase with age for both males and females, but particularly for men, and are highest amongst those 75 years of age or older.4
Collective violence results in direct mortality, mostly via small arms, and indirect mortality resulting from increased communicable diseases and an increase in deaths that could potentially be averted with adequate healthcare.5 Most direct mortality occurs in male combatants.6 Many civilian lives are also lost in contemporary conflicts; refugees and internally displaced people in particular typically experience raised mortality.7
If current trends in violence and injuries continue, the World Health Organization (WHO) predicts that violence and suicide will both individually feature in the top 20 causes of death and burden of disease issues confronting global health in 2030.8
Morbidity and impacts
Violence causes many more injuries than deaths, with the latter typically representing “the tip of the iceberg”. For example, estimates of non-fatal violence suggest that for every youth homicide around 20–40 victims of non-fatal youth violence receive hospital treatment.9 However, accurate morbidity data are lacking, as many injuries from violence do not prompt medical attention and there are significant cultural and other barriers to reporting. Surveillance systems are also generally inadequate for identifying incidents attributable to violence.
Violence has physical, psychological and social impacts. Periodic survey data have shown that between 10% and 50% of women experience physical violence at the hands of an intimate partner during their lifetime, and between 40% and 72% of all women who have been physically abused by a partner are physically injured at some point.1 Women who have been the victims of intimate partner violence have poorer physical health overall, are at higher risk of homicide and suicide, and have a greater risk of developing mental health problems, reproductive health problems and somatic and medical symptoms.10 A recent Australian study estimated that intimate partner violence was responsible for more ill health and premature death in women under 45 years of age than any of the other well-known risk factors, including high blood pressure, obesity and smoking.11
Globally, 15–25% of women report having ever been sexually assaulted and 5–10% of men and 20% of women reveal a lifetime prevalence of childhood sexual victimisation.12,13 Sexual violence can result in pregnancy and gynaecological complications, sexually transmitted infections, mental health and behavioural problems in adolescence and adulthood, suicidal behaviour and social ostracism.14 Child sexual assault is estimated to be responsible for 0.6% of disability adjusted life years (DALYs) globally.12
Ill health caused by child maltreatment makes up a significant component of the global burden of disease. Child abuse commonly results in psychological damage and experiences of violence in childhood, such as parental discord and domestic violence, are strongly associated with adverse outcomes for children’s development.15,16 There is evidence that major adult forms of illness, including ischaemic heart disease, cancer and chronic lung disease, can be linked to child maltreatment and other adverse experiences in infancy and childhood, mediated through the adoption of behavioural risk factors.17,18
Information on the morbidity associated with elder abuse is limited. Some studies report a rate of abuse of 4–6%, if physical, psychological and financial abuse and neglect are included.1,19 Because of frailty and dependency in old age, the physical and emotional consequences of abuse of older people can be severe.
Collective violence results in physical injuries, ongoing physical disability such as loss of limbs, increased sexual violence, an increase in water-borne, vector-borne and other communicable diseases, poorer reproductive health outcomes, acute and chronic malnutrition and mental health problems, including anxiety, depression, post-traumatic stress disorder and suicidal behaviour.5
Economic costs
The economic costs of violence include the direct costs of medical, policing and legal services, and the indirect costs of lost earnings and productivity, lost investments in human capital, life insurance costs and reduced quality of life. Estimates of costs across countries vary widely due to the use of different methodologies, including the measurement of productivity losses via foregone wages and income, which tends to undervalue losses in low income countries.3 Despite these differences, there is no doubt that violence results in staggering costs across the world, much of which is borne by the public sector.3 For example, violence is estimated to cost the USA the equivalent of nearly 3.3% of the gross domestic product (GDP).3 Intimate partner violence is estimated to account for 1.6% of the GDP lost in Nicaragua and 2% of GDP lost in Chile.3 The costs of violence in England and Wales have been estimated at US$40.2 billion (approximately £20 billion) annually.3 Direct medical costs alone per abused child in the USA are calculated at between US$13 781 and US$42 518.3
WHAT CAUSES VIOLENCE?
Theories of violence
Violence is a complex, multifaceted problem, and there are many different theoretical perspectives on its causes. These vary in the emphasis placed on psychological, interpersonal and structural factors, and in their underlying assumptions about whether human behaviour arises from free will or is determined by external factors. The most important theories in the psychological and criminological literature have been well summarised in Zahn et al.20
Perspectives on how power operates within societies vary according to whether power is conceptualised as a dominating structural force or rather is acting in the discourses of everyday relations.21–23 As a predominantly post-positivist science, public health tends to focus on the forms of violence that are amenable to rigorous, quantitative analysis.24 However, the pervasive nature of violence, the many levels on which it operates and the need for intersectoral action to prevent violence provide an opportunity for greater cross-disciplinary attention.
An ecological model
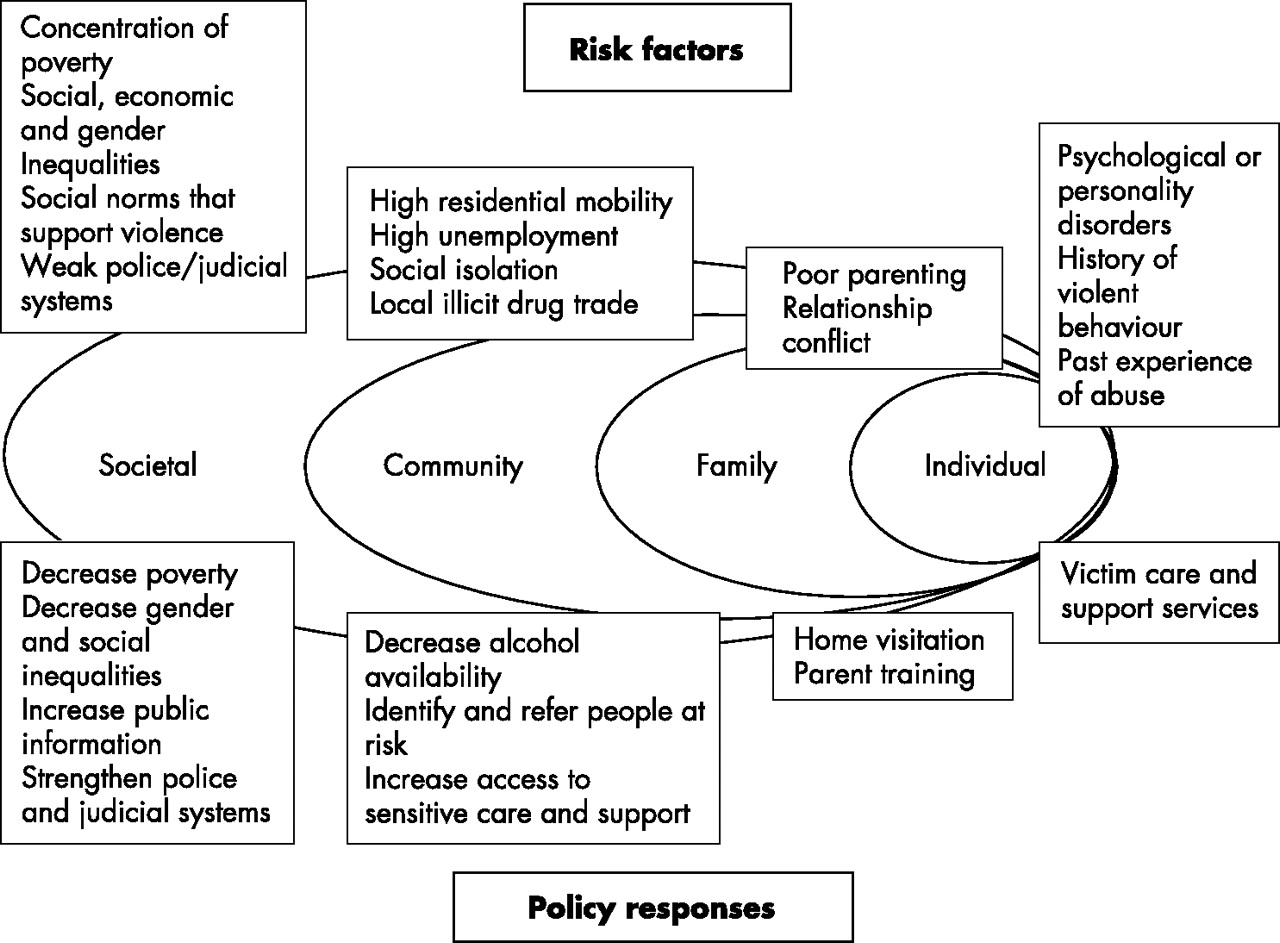
An ecological model for understanding violence has been used extensively by public health and other practitioners and researchers. This allows an examination of the multiple levels relating to violent behaviour: each operates in relation to others with individual factors modifying and interacting with relationship, community and societal factors. Powell et al argue that a model does not need to provide a comprehensive understanding of the causes of violence to be useful, but can identify risk factors that can be modified.25 Figure 1 demonstrates the ecological model, with examples of risk and preventive factors that may operate at each level.
{kind=link}
An ecological model for understanding violence.
Cross-cutting factors
While each type of violence may have a specific set of contributory factors and determinants, a number of these are common across different types of violence. Drug and alcohol use, certain demographic factors, access to firearms and social, economic, gender and other inequalities in the distribution of or use of power, all increase risks of a range of types of violence.
Alcohol and other drugs
Alcohol plays an important role in many forms of violence and has been documented as a risk factor for elder abuse, interpersonal violence, sexual violence, suicide and youth violence. The relationship between violence and alcohol is complex and the role of alcohol and the ability to address the issue publicly varies between cultures.26 Those who are victims of violence may also be at increased risk of substance misuse, whether this be tobacco, alcohol or other drugs. Substance abuse has been found to increase the likelihood of men committing sexual violence and some forms of youth violence. The drug trade itself increases the risk of violence as those individuals dealing in drugs are significantly more likely to carry handguns, while gangs involved in trafficking drugs have higher levels of violence than those that are not.27,28
Demographic factors
Recent research suggests that certain demographic factors significantly increase the risk of collective violence, especially civil conflict. These factors include having a high proportion of young adults (more than 40%, referred to as a “youth bulge”), high levels of youth unemployment, rapid rates of urbanisation, low availability of cropland (and associated disputes over farmland distribution) and scarcity of renewable fresh water.29
Social and economic inequality
Inequality between groups in society is an important risk factor for violence, especially collective violence, while gender inequality has long been recognised as a contributor to gender-based violence in many settings. Improving the status of women in general, including through enhancing access to education and reducing discrimination in the workforce, will in the long term decrease women’s vulnerability to interpersonal violence and increase the avenues available for them to protect themselves from and respond to risk of attack. Whilst few studies have explored the sex- and age-specific correlations between violence and economic inequality, one recent study of homicide suggests that economic development, economic inequality and homicide rates in children and youths have complex relationships that are strongly mediated by the victim’s sex and age.30 The economic indicators explained a significant amount of variance in homicide rates for males and females aged 15–24, although associations were much stronger for males than females in this age range. By contrast there were no significant associations between the economic measures and homicide rates for males and females in the age range 0–9 years.
Health workers have an important role to play in monitoring health-related indicators of inequity (such as avoidable disparity in diseases associated with poverty and economic inequality, discriminatory access to health services and marked discrepancies in survival rates for treatable conditions): early assessment of such indicators may help identify the need to learn more about how this comes about and what if any interventions could be pursued.
Firearms and their availability
Having access to weapons, particularly firearms, is an important factor in violent outcomes, particularly deaths from homicide, suicide and unintentional shootings. Firearm availability among specific populations increases the likelihood of a violent outcome. For instance, both women and children exposed to firearms are more likely to be the victims of gun violence than be protected by it.31 Both young people and the elderly are more likely to commit suicide if they have access to a gun.31
Approximately 200 000 people are killed annually by firearms in non-conflict situations, and approximately 300 000 people die annually in armed conflicts.31 It is frequently estimated that in modern conflicts over 90% of casualties occur among civilians and that these often result from the use of relatively unsophisticated small arms and light weapons. Arms manufacturing is an enormously profitable industry and it has been estimated that the five permanent members of the UN Security Council are responsible for 85% of conventional arms transfers.32 The continued proliferation of small arms and light weapons trade will have significant consequences for civilians, especially in conflict settings. Effective intervention in the area of weapons and arms trade requires a collaborative effort by legislators, police and health workers at national and international levels. The design of less lethal weaponry has also been promoted.
In some countries, such as Laos and Cambodia, landmines and unexploded ordinance continue to be significant problems. Widespread exposure continues to exert a negative effect on health and wellbeing, well after the cessation of particular conflicts.
IS RESILIENCE IMPORTANT?
Some individuals and groups are able to survive adversity and indeed to challenge it or grow as a result of their experiences. Resilience can be defined as “manifested competence in the context of significant challenges to adaptation or development”.33 Resilience may therefore ameliorate some of the risk factors for violence identified in the ecological model. For example, the links between being abused as a child and later abusing others have been widely documented, but this is clearly not an inevitable outcome. A deeper understanding and focus on how victims of child abuse recover to lead non-violent adult lives is required to inform intervention and treatment.
Some communities may be able to develop responses to violence and establish mechanisms to ensure that levels of violence do not create dysfunctional community and family structures. In other instances, levels of social trust and social capital may be so eroded that the lack of community support in itself is a major contributor to violence. Working with communities to promote effective, locally controlled mechanisms to boost resilience, reduce vulnerabilities and enhance protection is therefore important. Interventions cannot be imposed from outside – they need to be carefully shaped and determined by local insights and experience.
Recent findings show how the lifelong impact of child maltreatment on high risk behaviours may over decades contribute to the development of life-threatening illnesses.34 Resilience studies that look only for the most obvious symptoms (eg, post-traumatic stress disorder) and restrict themselves to only a few years or even a decade post-maltreatment may miss these important markers of damage due to violence and may over-estimate resilience. It is therefore important to take a life-cycle perspective in understanding resilience.
In the area of collective violence, there are countries that have high demographic risk but have managed to avoid civil conflict. The mechanisms through which this has been achieved will be of interest to policy makers and planners, but to date are relatively under-researched.
One of the challenges for health personnel is to recognise agency and acknowledge that even amidst devastating violence individual and collective capacities exist, and to find effective ways to assist in further developing these coping strategies and responses. Understanding how the cycles of violence and the intergenerational transfer of violence can be interrupted, and how public health practitioners can add to this effort, is an important area for further investigation.
WHAT IS THE ROLE FOR PUBLIC HEALTH?
The public health approach emphasises interdisciplinary, scientifically-based action to prevent harm to entire populations.1 Beaglehole et al35 argue that modern public health practice has five key themes:
-
Leadership of the entire health system
-
Collaborative actions across all sectors
-
Multidisciplinary approach to all determinants of health
-
Political engagement in the development of public health policy
-
Partnership with the population served.35
In relation to violence prevention, the role of public health has been articulated as:
-
Systematically collecting data on the magnitude, scope, characteristics and consequences of violence at local, national and international levels
-
Investigating why violence occurs, including those factors that may be modifiable
-
Exploring ways to prevent violence
-
Implementing promising interventions, determining cost-effectiveness and widely disseminating information.36
The WRVH made nine recommendations to mobilise intersectoral action in response to violence (table 1), and a follow-up publication provides guidelines on how to implement the first six country level recommendations.1,37
Recommendations of the first World report on violence and health1
For the purposes of this paper, we discuss several of these public health roles and priorities in relation to violence prevention in more detail.
Collaborative actions and multidisciplinary approaches
Many sectors are currently engaged in the prevention of violence. For example, violent crime is traditionally addressed through law and justice ministries, suicide through mental health services, child abuse through social welfare services and collective violence through military, United Nations and foreign ministry bodies. Attention has also been focused on violence by different disciplines. For example, feminist organisations and theorists have demonstrated the role of gendered inequities in the occurrence of violence and abuse.38 In developing countries, civil society organisations have been most important in propelling gender-based violence onto the health agenda.39 Criminologists have planned, implemented, evaluated and documented a range of community level crime prevention programs.
Each of the groups working in violence prevention has their own culture, concepts, theory, language, methods and priorities. For example, the “zero tolerance” approach to crime, commonly adopted by police and legal systems, focuses on the impacts of violence on society and punishes offenders on the assumption that this will deter future violent acts. The problem of violence is conceptualised as one of “moral failure”, where free agents have chosen to behave immorally.40 A public health approach, however, is more interested in understanding the causes and determinants of violent behaviour. If violent behaviour is understood as a result of adverse developmental experiences, the problem is then conceptualised “not merely (as) an individual’s moral failure; rather, the problem is a failure of society to provide adequately for its children”.40 These differing approaches could come into conflict at times, particularly when there is strong political investment in maintaining law and order. Indigenous communities in Australia, for example, seek to focus attention on the structural determinants of violence and may see societal interventions as most appropriate, whereas those focused on law and order may see incarceration as an important solution on its own or in combination with other interventions. However, as many of the causes and remedies for violence are cross cutting, collaboration across different groups, and across different disciplines, will be required if the prevention of violence and a reduction in the toll of mortality and morbidity are to be achieved.
Working across public health disciplines
The recommendations of the WRVH have implications for many sectors within public health. To date, violence has been typically addressed under the framework of “intentional injuries” in the injury prevention field. However, while unintentional injuries have attracted increased attention in a number of countries over the past two decades, intentional injuries, as a general category, have largely been neglected by those focusing on injury control until relatively recently. In addition, the theoretical basis for addressing intentional injuries is not nearly as well articulated as that for addressing unintentional injuries within injury prevention. Some argue that situating violence prevention within an injury framework limits the potential for focusing on structural causes of violence: “while public health professionals may see the causal relationships between social factors and violence in populations, the toolbox from which we draw may limit us to interventions directed towards the agents of injury (such as firearms) and individual level variables such as knowledge, attitudes and behaviours. Thus in some sense the toolbox may define the mindset”.41 Others argue that “the inclusion of injuries regardless of intent in surveillance systems, the commonality of the agencies carrying out prevention and the existence of risk factors which cut across intent argue strongly for the inclusion of intentional injuries within the scope of injury research and prevention”.42 There is scope for many different segments of the public health community to engage more interactively in the prevention of violence and to add to the work being conducted in injury prevention: women’s health, community paediatrics, public mental health, drug and alcohol, community development, policy and management to name a few.
Systematic data collection
Data are valuable in determining the magnitude of a problem, identifying groups or sub-groups that are most affected, detecting patterns in risk of exposure or occurrence of events, measuring baseline and subsequent results of interventions, and providing data around which to advocate for policy changes. Violence can be measured at individual and community levels via mortality and morbidity data, prevalence and victimisation surveys, crime statistics, health and social services expenditure and periodic studies of attitudes, beliefs, behaviours and cultural practices. Population level data on income, education and unemployment rates can highlight specific violence risk and protective factors.
All forms of violence are notoriously under-reported as much violence takes place within the home or street without being officially notified, or without contact with health, police or legal services. Where adequate health facility-based and police recording of violent incidents does exist, there are numerous challenges associated with identifying and linking data sources. These include differences in the purpose of and methodology used for collection of data by different sectors (such as health, legal and crime statistics) and the varied availability and quality of data sources in different countries.
Recent initiatives to better measure violence include approaches to discussing and documenting interpersonal violence that results in attendance at accident and emergency departments,40,43,44 focusing more attention on marginalised groups at risk of violence, such as the high risk of suicide in the “old elderly”,45 documenting the risks of elder abuse in residential homes and the risk of collective violence against minority or immigrant communities, and trialling new strategies to increase reporting such as the use of social marketing techniques to encourage reporting of child abuse.46 Effective systems for collecting data about violence would collate information from, at least, the health and criminal justice sectors, victim surveys and other routine data collection mechanisms, and ensure that the results were widely disseminated.
Developing prevention and intervention strategies
Work in violence prevention, particularly in the last two decades, has demonstrated that:
-
interventions delivered during infancy and in childhood and those sustained over time are more likely to be effective than short-term programs,
-
proven and promising interventions with adolescents and young adults include providing at-risk disadvantaged high school students with incentives to complete their education and
-
comprehensive, scientifically based programs are more likely to be successful.
Despite many ongoing activities, very few violence prevention programs have been rigorously evaluated.1 Few countries have systematic knowledge of how prevention projects operate in their specific settings, what types of violence and risk factors are addressed, the target populations served, intervention strategies employed and how programs are measured and monitored. This is true for countries at all levels of development, although the paucity of outcome evaluation from low to middle income countries is of especial concern.47 WHO is attempting to address this through the development and implementation of guidelines for the systematic documentation of interpersonal violence prevention programs.48 The results from the implementation sites in selected low to middle income countries will be collated into a global database to identify and analyse trends in violence prevention programming as a basis for strengthening systematic and science-based program components. The primary prevention of violence is particularly underdeveloped and requires more sustained activity. Due to the disproportionate burden of violence in poorer countries, mechanisms to support and implement prevention and intervention efforts in these settings deserve particular attention and resources.
An example of an intervention to reduce youth violence: the United States Multisite Violence Prevention Project
The frequency of violence and other problem behaviours tends to increase with the onset of the multiple developmental changes and challenges of adolescence. The US Multisite Violence Prevention Project was a 5-year, government-funded project to compare the effects of a universal intervention (students and teachers) with a targeted intervention (family program for high risk children) on reducing aggression and violence amongst children in sixth grade (11–12 years of age).49 Thirty seven schools were randomly assigned to four conditions: control, universal intervention, targeted intervention and universal plus targeted intervention. Interventions were based on the GREAT (Guiding Responsibility and Expectations for Adolescents for Today and Tomorrow) student, teacher and family programs.50 Outcome measures assessed included victimisation from and perpetration of relational, non-physical and physical aggression in peer and dating relationships, mediating variables (eg, problem-solving skills) and moderating variables (eg, beliefs and norms about violence).51 Although the outcome measures are yet to be published, some important lessons were learned in the conduct of this large-scale collaborative project.52 An important feature of this project was its attempt to retain the scientific rigour of smaller efficacy trials but expand demonstrated methods into a diverse population in a “real-world” setting. Despite the inherent challenges, the researchers urge a continued move towards the translation of “intervention theory into usable practices” rather than wait years for the accumulated results of smaller-scale systematic studies.
Although the widespread prevention of violence is in its infancy, the evidence base will develop as research and intervention trials proceed and the results become widely known. Public health efforts must balance implementing what is proven to be effective, trialling innovative strategies and preventing harm to individuals and communities in the process. It is important to also consider the ethics of intervention. Efforts to uncover and disclose vulnerabilities and risks should not lead to increased exposure to violence or other adverse psychological or health outcomes. Identifying higher levels of violence in some families and communities poses the risk of stigmatising those families and communities rather than focusing attention on the structural factors which predispose to high levels of violence. Careful evaluation of interventions around such programs as routine screening for intimate partner violence and child maltreatment must be undertaken, and must include analysis of both intended and unintended consequences, positive or negative, if a balanced assessment of the appropriateness and desirability of key interventions is to be made.
An example of a well-meaning and disturbingly popular group of strategies shown through outcome evaluation studies to have adverse outcomes are those that focus on relationships between peers, including those that are designed to change the nature of peer interactions or peer group norms or redirect peer group activities. The latter, for example, have been tried with gangs. There is little evidence to date that these approaches are effective in reducing violent behaviour, particularly as single component programs. Some have also had unintended consequences: mixing of high risk youth has had the unintended consequence of increasing cohesiveness and facilitating antisocial behaviours.47,53,54
Although there are relatively few published economic evaluations of interventions targeting violence, available studies in the area of interpersonal violence demonstrate that preventive interventions cost less money than they save, in some cases by several orders of magnitude.3 Although it is known that there is a relationship between absolute and relative poverty (income inequality) and violence, the research evidence, particularly from low and middle income countries, is lacking. Economic analyses of the cost-effectiveness of violence interventions, the causal relationships between poverty, inequity and violence and the development of methodological guidelines to allow cross country comparisons are important areas for future attention.3
Political engagement and advocacy
Changes in government policies on matters such as the availability of firearms or alcohol or the tolerance of bullying, all have the potential to reduce the level of violence and minimise the consequences of violent behaviour. Health practitioners are in a unique position to advocate for the improved protection for those at risk of violence, improve responses for the victims of violence, recognise violence as a preventable problem, promote awareness of violence as a public, “community” issue rather than a personal or private concern and advocate for increased allocation of resources towards research and intervention to reduce violence in all areas of society.
The less visible forms of violence, such as child maltreatment and intimate partner violence, whilst subject to strong taboos in many societies, are still often considered to be less important to address than other forms of violence. Consigning violence against women and child maltreatment to the “private”, “domestic” sphere enables society to abrogate its preventive responsibilities: Fineman and Mykitiuk argue, in the feminist tradition, that “private violence” is a public issue.55 Leadership in the area of violence against women, for example, “must demand that our social understanding of violence shift from one of inevitable human nature to socially created, and, therefore, preventable human behaviour…our efforts and resources (must not be) dedicated solely to the support of victims/survivors or the incarceration of offenders. Such restricted efforts will never end violence”.56
Comprehensive surveillance and data collection will highlight the areas requiring intervention, and may identify inequitable access to resources, such as emergency medical care and rape crisis centres, geographic areas with greater risk and communities with highest levels of exposure to violence. Public health practitioners must place clear recommendations before decision makers regarding action required to prevent violence; doing so, however, requires access to well conducted outcome evaluations of violence-related interventions. As mentioned above, policy and planning to prevent violence requires intersectoral action including working with other sectors such as criminal justice, education, welfare and social policy to deepen understanding of the causes of violence, implementing evidence-based interventions through schools and community structures, working with demographers to predict countries with high risk of civil conflict based on demographic and socio-political data and recommending changes in economic, social and gender policies that can help to reduce economic and gender inequalities.57 Although much more difficult to achieve than individualised solutions, addressing the structural inequalities that contribute to violence is central to achieving long-term solutions.
WHAT ARE THE KEY CHALLENGES AND OPPORTUNITIES?
Key challenges include addressing reticence on the part of governments and other agencies to promote violence prevention, challenging the prevailing belief that violence is inevitable, the lack of “ownership” and therefore championing of violence prevention (including within the public health arena), the relative lack of well conducted and evaluated trials of violence prevention initiatives and therefore risks of implementing ineffective or harmful initiatives, and the lack of data on the cost benefit and cost effectiveness of various interventions. Finding ways to successfully “frame” the prevention of violence is an important next step for public health.
However, there are clear opportunities in the increased recognition that violence is preventable, recent coordinated international efforts to prevent violence and disseminate data on effective strategies and further understanding of the characteristics that make individuals and communities resilient to experiences of violence. Applying the public health approach to violence provides an opportunity to take a sustained, interdisciplinary and scientific approach with the potential to make a significant contribution to preventing violence.
CONCLUSION
Defining the most appropriate roles for public health in the prevention of violence is a challenge. Traditionally the domain of the criminal justice system, violence has only recently attracted a multi-sectoral approach. Public health practitioners have a role in identifying and documenting the range of forms of violence that exists in communities, especially many of the hidden or “private” forms of violence, including child maltreatment, intimate partner violence and elder abuse. Identifying the determinants of these patterns and establishing the scope for intervention is paramount. As more knowledge about violence and its causes emerges, public health must seek to intervene with new and creative solutions that increase policy makers’ confidence in, and understanding of, violence as a preventable problem. This includes conducting well planned and evaluated interventions and requiring cost benefit analyses of initiatives. Projects such as the WHO’s Economic dimensions of interpersonal violence3 deliver an important message to governments and community organisations about the impact of violence and the need to invest in prevention initiatives at a local, national and international level.
What this paper adds
-
A concise description of global burden of violence is provided.
-
Cross-cutting considerations in addressing the problem of violence are discussed.
-
The importance of promoting equity and addressing inequalities if violence is to be prevented upstream is highlighted.
-
The importance of recognising and bolstering resilience is stressed.
Policy implications
-
Public health has an important role to play in advocating for, and shaping, societal responses to violence.
-
Cross-cutting elements to violence prevention include addressing the availability of firearms, the excessive consumption of alcohol and the presence of significant social inequalities.
-
Better recognition and appreciation of how people survive adversity and demonstrate resilience may have important clues for developing future policy responses.
REFERENCES
Footnotes
-
Competing interests: AZ was a co-editor of the World Report on Violence and Health. AB works for the World Health Organization which campaigns and provides technical advice on violence prevention.
Linked Articles
- In this issue