Article Text

Abstract
Objective To describe the characteristics of childhood burns and scalds, mechanisms and agents to inform prevention.
Methods Prospective multicentred cross-sectional study of children (<16 years) with unintentional burns/scalds from five Emergency Departments (ED), a burns assessment unit and three regional children's Burns Units. Data collected: site, severity, distribution of the burn/scald, age, motor development of the child, agent and mechanism of the injury. Comparative analysis for children <5 and 5–16 years.
Results Of 1215 children, 58% (709) had scalds, 32% (390) contact burns and 116 burns from other causes, 17.6% (214/1215) were admitted to hospital and the remaining treated in ED or burns assessment centre. 72% (878) were <5 years, peak prevalence in 1-year-olds. Commonest scald agent (<5 years) was a cup/mug of hot beverage 55% (305/554), and commonest mechanism was a pull-down injury 48% (66/554). In 5–16-year-olds, scalds were from hot water 50% (78/155) and spill injuries 76% (118/155). Scalds affected the front of the body in 96% (680/709): predominantly to the face, arms and upper trunk in <5-year-olds, older children had scalds to the lower trunk, legs and hands. Contact burns (<5 years) were from touching 81% (224/277) hot items in the home, predominant agents: hair straighteners or irons 42% (117/277), oven hobs 27% (76/277), 5–16-year-olds sustained more outdoor injuries 46% (52/113). 67% (262/390) of all contact burns affected the hands.
Conclusions Scalds to infants and toddlers who pull hot beverages over themselves or sustain burns from touching irons, hair straighteners or oven hobs are a high priority for targeted prevention.
- Epidemiology
- Adolescent Health
- Injury Prevention
- Accident & Emergency
Statistics from Altmetric.com
What is already known
-
Published studies mainly describe childhood burns and scalds that are treated in inpatient Burns Units.
-
Studies look at the overall patterns of burns in children 0–16 years.
What this study adds
-
The majority of childhood burns are seen in Emergency Departments. The mechanisms, agents and patterns of burns are significantly different between children under the age of 5 and those who are older than 5.
-
1-year-olds suffer 10 times as many burns and scalds as any school year age group.
-
Hot beverages are responsible for most scalds in infants and toddlers who reach up and pull them down over themselves. The commonest cause of contact burns are from children touching irons, hair straighteners and oven hobs.
Introduction
Children account for half of all burns and scalds seen in European hospitals.1–3 These are painful, potentially fatal and carry a risk of lifelong scarring and deformity, with associated physical, psychological consequences and long-term healthcare requirements. An estimated 25 000 children attend Emergency Departments (ED) in England and Wales annually with a burn or scald. Approximately 3800 receive inpatient hospital treatment.4
Contributory factors are a complex interaction between the characteristics of the host (child), agent (heat source), mechanism (how the child comes into contact with the agent) and the environment (where the event occurs).5 These factors have a direct relationship to the extent, distribution and pattern of injury that the child sustains.6
Published epidemiology is largely drawn from inpatient data, which captures the serious injuries and may give a distorted picture of the range and extent of childhood burns.7 There are a handful of recent paediatric burns epidemiology studies from the UK or Ireland,6–8 very few describe children who present to ED.9 ,10
This study aims to describe the mechanisms, agents and clinical features of unintentional burns and scalds in a representative sample of children seen in ED and regional Burns Units in the UK and the Republic of Ireland to provide a greater understanding of the injury process in children of different developmental ages and to inform primary preventative strategies.
Methods
A prospective multicentred cross-sectional study of children with burns or scalds presenting to five ED (Cardiff and Vale University Hospital Board (UHB), Birmingham Children's Hospital, UK; The Adelaide and Meath Hospital, Children's University Hospital Temple Street; Our Lady's Children's Hospital, Dublin, Ireland), Morriston Hospital Abertawe Bro Morgannwg UHB Burns Assessment Unit, Swansea, and the three regional children's inpatient Burns Units (Morriston Hospital UHB, Swansea; Our Lady's Children's Hospital, Dublin; and Birmingham Children's Hospital) was conducted.
A clinical assessment and data collection proforma (see web appendix 1) was completed at hospital presentation for children less than 16 years old. Victims of household fires were excluded. The location and distribution of the burn or scald was drawn on a body map. The age of the child, motor developmental milestone and place of injury were recorded together with details of the agent, mechanism and severity of the injury. Each data field on the proforma was completed in more than 90% of cases, with the exception of ‘previous hospital attendances’ and ‘percentage body involved’ that were poorly completed in the ED setting. Cases were anonymised, given a unique case number, and data entered into a Microsoft Access database and exported into PASW SPSS V.18 and Microsoft Excel for analysis.
Negotiation of Research and Development approvals in the hospitals involved meant that there was a staggered enrolment of research centres. Data were collected between July 2008 and December 2010 but for different time intervals for each centre (see web appendix 2).
Data analysis
Proformas were completed by the admitting clinician as frequently as deemed possible, allowing for workload; since data were not collected with any prior selection process in place, simple random sampling is proposed. The ascertainment rates were calculated as a proportion of total hospital attendance figures for children with burns or scalds over the same time periods. Ascertainment rates exceeding 80% were deemed reasonable coverage. Lower rates were evaluated against hospital attendance, age distribution and injury type (where available) to test whether representative samples were attained. Since age was not normally distributed, a Mann–Whitney U test was performed to test a difference in age distribution for each unit.11 A χ2 goodness-of-fit test was performed to assess differences in the distribution of burn type.12
A descriptive analysis compared children less than five completed years of age and those 5–16 years. The distribution of burns and scalds was analysed according to 20 (see web appendix 6) anatomical sites that were affected. For scalds, the uppermost affected site was recorded as the primary site. For contact burns and other causes, the region with the most severe burn was recorded as the primary site. The proportions of the populations affected with 95% CIs were calculated, and two-sample z-tests (significance level of 5%) were employed to examine differences between age groups.13
Results
Ascertainment
A total of 1327 cases were notified. Levels of ascertainment varied between centres, however, the mean age and age distribution of cases notified was not significantly dissimilar to that of the total number of children attending each unit with a burn over the same time period, giving a representative sample for each unit (see web appendix 3). Comparison of the distribution of burn type between our samples and the overall attendance figures demonstrated no statistically significant differences in the distribution of burns and scalds with the exception of Birmingham ED (p<0.0005) where we estimate an under-representation of contact burns by 25 cases (6% of all contact burns notified) and over-representation of scalds by 25 (3.5% of total scald cases).
Epidemiology of burns
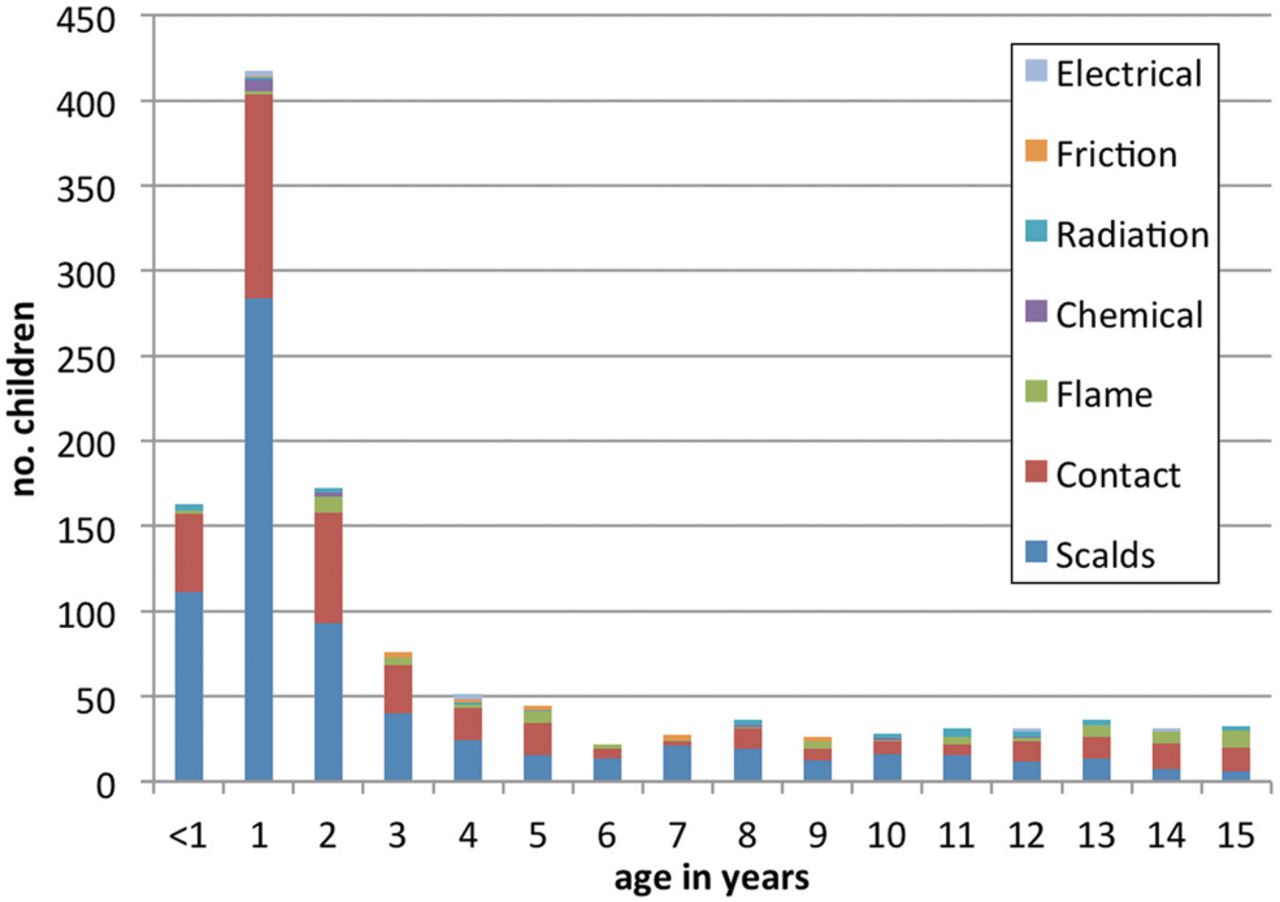
Child maltreatment was suspected in 112/1327 cases and excluded from further analysis. Mean age of the remaining 1215 cases was 3.74 years (SD 4.3). The gender ratio approximated 3 : 2 (M:F). Peak prevalence for all causes, with the exception of flame burns, occurred in 1-year-olds (figure 1); prevalence started to increase at 9 months of age corresponding to the onset of independent mobility (see web appendix 4). Burn depth included full 3.5% (42/1215), partial thickness 76% (924) and erythema in 20.5% (249) of the children.
{kind=link}
Age breakdown in years according to burn type for 1215 children.
Type of injury
The majority, 58% (709/1215) were scalds, 32% (390) contact, 5.5% (67) flame, 1.6% (20) radiation, 1% (13) chemical, 1% (11) friction and 0.4% (5) electrical burns. Ninety-eight per cent (1189) presented to ED or a burns assessment centre (80). Overall 17.6% (214/1215) were admitted to a burns inpatient units. The proportion of scalds was the same among children who were seen and treated in ED as for those who were hospitalised. The proportion of contact burns among hospitalised cases was significantly less than those treated in ED or an assessment centre (24% (95% CI 18.6% to 30%) vs 34% (95% CI 31% to 39%)) p=0.002. A greater proportion of hospitalised cases were from flame burns (11.7% (95% CI 8% to 16.7%) vs 4% (95% CI 3% to 5.5%)) p<0.0001.
Scalds
All scald incidents happened in the home. Three categories of agent were involved; hot beverages 49.6% (352), water 37.6% (267) and food 12.7% (90) (table 1). Seventy-eight per cent (554/709) were sustained by children (<5 years), and the commonest agent was a hot beverage in a cup or mug. There were relatively few bath scald incidents, and 11 children fell or climbed into a bath. Twelve cases were from flowing shower or tap water.
Scald agent and mechanism by age (n=709): number of children with scalds from different categories of agent and proportion of each mechanism involved
The mechanisms of injury were related to the age and development of the child (see online supplementary appendix 5) and the agents involved. The commonest mechanism in children (<5 years) was to pull a hot drink (n=186), hot water (n=62) or hot food (n=18) down over themselves, the youngest child to do this was 8 months of age. The youngest child to climb into a bath of hot water was 16 months, and 20/33 scalds that involved an adult tripping or spilling hot liquids were to infants, while spill injuries were recorded from 4 months to 15 years of age.
Distribution of the scalds
Scalds affected the front of the body in 96% (680/709) and rarely affected the buttocks, groin or back (table 2). Children (<5 years) sustained a significantly greater proportion of scalds to the face, arms and upper trunk than the older children who sustained scalds to the lower trunk, legs and hands.
Primary site affected by a scald in 554 children younger than 5 years old and 155 children 5–16 years (percentage of children with scald in each site)
In the children (<5 years), 51.6% (286/554) of scalds extended to adjacent sites as the hot liquid flowed away from the first point of contact. This only applied to 25.8% (40/155) of scalds in the 5–16-year-olds, where scalds were predominantly restricted to one site.
In children (<5 years), scalds affecting the face and upper trunk were twice as frequent from a pull-down injury, 163/267 (61.0 (95% CI 55.1 to 66.7), as from a spill injury, 74/267 (27.8%) (95% CI 22.7% to 33.4%); while scalds to the lower trunk or limbs were equally likely from a pull-down 89/230 (38.7% (95% CI 32.6% to 45.1%) or spill injury 88/230 (38.2% (95% CI 32.2% to 44.7%). Touch or immersion incidents predominantly affected hands or feet. Three of the seven children who climbed into a bath had bilateral scalds to the feet, two had buttock and lower limb scalds and one had scalds to the arm and hand.
Contact burns
Seventy-one per cent (277/390) occurred in children (<5 years). Four categories of agent included: portable 41% (160/390), fixed household appliances 37% (145/390), outdoor agents 19% (74/390) and miscellaneous 3% (11/390). Seventy-three per cent of burns from portable items (117/160) were from irons or hair straighteners and 53% (76/145) of fixed household appliance burns were from the oven hob. Oven doors, radiators, radiator pipes and household heaters were responsible for a further 43% (62/145) (table 3). Eighty-three per cent (252/305) of household incidents occurred in children (<5 years), where the commonest mechanism was touching a hot item. Seventy per cent (52/74) of outdoor incidents were in the older age group, many of which resulted from explosive mechanisms. All except two of the 43 firework incidents were reported from Dublin centres (firework legislation was different to UK).
Contact burn agent and mechanism by age (n=390): number of children with contact burns from different categories of agent and proportion of each mechanism involved
There was no difference in the distribution of contact burns between the two age groups (see web appendix 6). Sixty seven per cent (262/390) affected the hands; 82.4% (216/262) were palmar. Only 11% (42) involved more than one site, in 35 the burns were bilateral, 14 had a symmetrical appearance, coinciding with children standing on hot items or touching an appliance with both hands. Burns to the feet were recorded in 14 children from hair straighteners (8), an oven hob (3), hot sand (1) and barbeque (2). Hair straightener burns affected the sole of the foot (4) or the sole and upper foot (4) and were unilateral.
Other burn types
There were 67 flame burns, 70% (47) in the older children (table 4). Sixteen involved children touching the flames. Twenty-five teenagers were playing with fuel, aerosols or lighters. Burns primarily affected the hands 33% (22/67) or face 18% (12), with 33% (22) extending to more than one site.
Other burn agents and the number of children involved
Radiation burns: eight children (<3 years) sustained facial sunburn, 11 teenagers had generalised sunburn, two sustained full thickness, 12 partial thickness and five widespread erythema. Eight of 11 friction burns were in children who touched treadmills. Chemical burns involved children (<3 years) from a splash (4) spill/pull-down (4) fall (2) touch (2) and one ingestion. Four electrical burns in children who touched electric cables and one intraoperative burn from cautery.
Discussion
Children with 1-year-old sustain 10 times more burns or scalds than any year of school-age children (figure 1). The prevailing mechanism involved the toddler reaching for a mug or cup of tea and pulling it down over themselves or touching household objects including irons, hair straighteners, oven hobs or oven door. This is a clear priority for targeted prevention.
While the high prevalence of childhood burns and scalds in toddlers and the predominance of scalds over contact burns has been described,2 ,6 ,10 ,14–18 few studies describe injury mechanisms relating it to the agent, age of the child and the subsequent pattern of injury. There is a distinct evolution of the mechanism of injury with age (see web appendix 5). Drago et al15 identified the high prevalence of toddlers pulling down containers of hot water over themselves in the kitchen. Having identified a low proportion of tap water scalds in the under 5-year-olds, Lowell et al19 described similar scald agents to ourselves; however, there were fewer hot drink scalds in their US population. The peak prevalence in infants started at 9 months of age when independent mobility begins, infants are exploring their environment without the awareness of dangers. Parents appear to be unready for this developmental stage in terms of preventative strategies. They may underestimate the potential reach height of their toddler. The height of an average 1-year-old is 74–76 cm (WHO growth charts). Their reach height is potentially consistent with the average dining table (standard mean height 75 cm) cooker hob or kitchen work surface (standard height 90 cm). The prevalence of burns and scalds falls dramatically at 3 years of age, which may coincide with an increased cognitive awareness of the dangers of heat, a more vigilant approach by parents or a greater proportion of time spent outside the home.
Many studies focus on preschool children;15 ,17 ,19 however, school-age children have a different profile, and scalds were predominantly from spill injuries from food or domestic containers of hot water rather than hot beverages. Contact and flame burns14 ,20 were largely sustained outdoors.
There was a largely predictable relationship between the agent and mechanism, age of the child and anatomical distribution of the burn or scald. The toddler pull-down scald resulted in a scald to the upper part of the body. Older children sustained scalds to the hand or lower limb. Scalds were predominantly on the front of the body, asymmetrical and rarely affected head, buttocks, genitalia or back of the body. Contact burns to the hand in small children may be extensive and carry the risk of long-term disability from contractures and scarring. Children who present with an atypical pattern of burn or scald and an implausible explanation may raise suspicion of intentional injury.21 Child abuse is recorded in an estimated 1% to 14%14 ,20 ,22 of children in the hospital setting with a burn or scald, 8.4% of the total population of children ascertained in this study were referred to social services with suspected child abuse and were excluded from analysis.
Successful prevention is most likely to involve product design or environmental modification as has been shown with installation of thermostatic mixer valves to reduce hot tap water scalds,23 ,24 and the burden of bathtub or hot tap water scalds in this dataset as in other studies19 ,25 was relatively small. However, universal product modification for tea mug scalds is challenging. Ramanathan et al26 measured the temperature of hot drinks in different cup types and estimated that the risk of a disfiguring scald lasts for 11 min after the drink was poured. Prevention is likely to rely upon heightened awareness and behaviour change by carers.27 ,28 Public information messages, children centres, health visitor or family nurse practitioners should address safety education as a matter of routine. There is evidence that intensive interventions of this kind can successfully reduce scalds to children in the home.29 ,30
Irons31 and hair straighteners32 ,33 are common domestic appliances often left on the floor. Hair straighteners reach temperatures of 163–169.5° centigrade and retain a heat of 80°C for 6–8 min when turned off, with the potential to cause full thickness burns.32 While these appliances must be kept out of the reach of children, there is the potential to explore modification to product design to ensure toddler safety.
While Yen et al34 described 14 cases of serious burns to the hands from oven doors that reach variable and high temperatures.35 Oven hob burns do not feature in current published literature. Many modern oven doors have a ‘cool touch’ design. This is not universal and many households have old appliances.
Childhood burns depend heavily on what is present within the domestic environment. These vary over time and between cultures.5 ,18 An ongoing surveillance of childhood burns and scalds would inform relevant preventative strategies. The National Burns Injury database36 fulfils this purpose within the Burns Units; however, it does not include ED where the majority of children present. This study highlights the potential benefits of detailed routine data collection and underpinned a successful bid to the Healing Foundation who have funded The Burns Collective: Children's Burns Research Centre. The project will develop an integrated child burns prevention initiative and ongoing epidemiological data collection.
Acknowledgments
Leads in collaborating Centres: M Mackay, C. Martin, R Summers, E Curtis, G DeBelle.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Files in this Data Supplement:
- Data supplement 1 - Online appendix 1
- Data supplement 2 - Online appendix 2
- Data supplement 3 - Online appendix 3
- Data supplement 4 - Online appendix 4
- Data supplement 5 - Online appendix 5
- Data supplement 6 - Online appendix 6
Footnotes
-
Contributors AK: project design, supervision, principal investigator, data analysis and project write up. SJ: collected the data and entered onto database, database design. ZL: statistical analysis. SM: research design, centre enrolment, manuscript writing and editing.
-
Funding Wales Office of Research and Development MRC Health Care Partnership. This project underpins the ongoing research of The Burns Collective: Children's Burns Research Centre. A Healing Foundation Initiative with partnership funding from NISCHR Wales.
-
Competing interests All authors have completed the ICMJE uniform disclosure form at http://www.icmje.org/coi_disclosure.pdf and declare: SJ had financial support from NISCHR /MRC Health Research Partnership Award for the submitted work; no financial relationships with any organisations that might have an interest in the submitted work in the previous 3 years; no other relationships or activities that could appear to have influenced the submitted work.
-
Ethics approval England and Wales 08/H0504/133 Dublin REC 2009/02/02. Waived consent and the process of data recording were approved by the National Information Governance Board (PIAG4-05(i)2008).
-
Provenance and peer review Not commissioned; externally peer reviewed.
-
Data sharing statement Additional data are on the web-based appendices. Research database would be available for further analysis.