Article Text

Abstract
AIMS To evaluate the effects of promotion of residential smoke alarms.
METHODS Electronic databases, conference proceedings, and bibliographies were systematically searched, and investigators and organisations were contacted, in order to identify controlled trials evaluating interventions designed to promote residential smoke alarms. The following were assessed: smoke alarm acquisition, ownership, and function; fires; burns; and fire related injuries. Odds ratios (OR) were estimated by meta analysis of randomised trials.
RESULTS A total of 26 trials were identified, of which 13 were randomised. Overall, counselling and educational interventions had only a modest effect on the likelihood of owning an alarm (OR = 1.26; 95% confidence interval (CI): 0.87 to 1.81) or having a functional alarm (OR = 1.19; 95% CI: 0.85 to 1.66). Counselling as part of primary care child health surveillance had greater effects on ownership (OR = 1.93; 95% CI: 1.04 to 3.58) and function (OR = 1.72; 95% CI: 0.78 to 3.78). Results were sensitive to trial quality, however, and effects on fire related injuries were not reported. In two non-randomised trials, direct provision of free alarms significantly increased functioning alarms and reduced fire related injuries. Media and community education showed little benefit in non-randomised trials.
CONCLUSION Counselling as part of child health surveillance may increase smoke alarm ownership and function, but its effects on injuries are unevaluated. Community smoke alarm give away programmes apparently reduce fire related injuries, but these trials were not randomised and results must be interpreted cautiously. Further efforts to promote smoke alarms in primary care or through give away programmes should be evaluated by adequately designed randomised controlled trials measuring injury outcomes.
- accident prevention
- burns prevention
- smoke alarms
- systematic review
Statistics from Altmetric.com
Residential fires caused at least 67 deaths and 2500 non-fatal injuries to children aged 0–16 in the United Kingdom in 1998.1 Among children aged 0–14, fire and flames are the second leading cause of unintentional injury death.2 Fires detected by smoke alarms are associated with more rapid discovery, lower casualty rates, and less property damage.1 Smoke alarm ownership is associated with a reduced risk of fire death,3-5 and appears particularly effective in households with young children.3 5 Because controlled trials provide the best evidence about effectiveness, we systematically reviewed trials evaluating interventions to promote residential smoke alarms, to assess their effect on smoke alarm ownership and on fire related injuries.
Methods
INCLUSION CRITERIA
We included original studies if: (1) subjects were prospectively assigned to study groups (controlled trials); (2) subjects were not institutionalised; (3) the experimental intervention was designed, either wholly or in part, to promote residential smoke alarms; (4) outcome data were collected concurrently from intervention and control subjects; (5) outcomes included smoke alarm ownership, installation, function, or acquisition; fires; burns; or fire related injuries; and (6) the study was completed or published after 1969 (residential smoke alarms became widely available and affordable in the mid 1970s).
DATA SOURCES
We searched the Cochrane Controlled Trials Register (Cochrane Library 1998, issue 1), Cochrane Injuries Group database (March 1998), Medline (1970 to January 1998), EMBASE (1970 to January 1998), PsycLIT (1974 to January 1998), Cumulative Index to Nursing and Allied Health (CINAHL) (1982 to January 1998), Educational Resource Information Center (ERIC) (1989 to January 1998), Dissertation Abstracts (1970 to January 1998), International Bibliography of the Social Sciences (1970 to January 1998), Index of Scientific and Technical Proceedings (ISTP) (1970 to January 1998), FIREDOC (Fire Research Information Service,http://firedoc.cfr.nist.gov/) (1970 to March 1998), and LRC, the US Fire Administration's online database (http://www.usfa.fema.gov/lrc/) (1970 to March 1998).
We searched Medline by combining a published methodological filter for controlled trials (phases 1 and 2)6 or (volunteer* in ti or in ab) or the mesh headings “EVALUATION-STUDIES” or “PROGRAM-EVALUATION/all subheadings” or “INTERVENTION-STUDIES”, with relevant content terms. These content terms included “ACCIDENTS”/all subheadings, ACCIDENT-PREVENTION, “BURNS”/prevention-and-control, “FIRES”/prevention-and-control, (fire or smoke) near (detector* or alarm or alarms), (accident* or safety) near home, (fire or fires or burn or burns or smoke) near (prevent* or control), (explode “BURNS”/all subheadings or explode “FIRES”/all subheadings or “SMOKE-INHALATION-INJURY”/all subheadings) and (“PROTECTIVE-DEVICES”/all subheadings or “SAFETY”/all subheadings), and other terms (available from author). Similar search strategies were developed for each database. We searched the Cochrane registers, ISTP, FIREDOC, and LRC without methodological filters.
We examined reference lists of reviews,7-12 conference proceedings,13-16 and case study collections.17-20 To find internal or unpublished documents, we contacted national and international organisations involved in fire and injury prevention, such as the Home Office (United Kingdom), National Fire Protection Association (United States), Centers for Disease Control and Prevention (United States), Centre d'Information et de Rencontre pour la Prévention des Accidents d'Enfants (France), and International Society for Child and Adolescent Injury Prevention.
STUDY SELECTION
Title, abstract, and keywords of all citations were reviewed and, using the first four inclusion criteria, ineligible studies were excluded. The full texts of remaining citations were reviewed and those that failed to meet these four inclusion criteria were excluded. We contacted corresponding authors of all remaining studies to determine eligibility, request outcome data, or other details, and identify additional trials. When the corresponding author was deceased or untraceable, we contacted additional authors.
DATA EXTRACTION
Two investigators independently extracted data on participants, interventions, outcomes, loss to follow up, and methods of allocation concealment and outcomes assessment (as quality indicators21). Allocation concealment was rated as adequate if methods convincing of concealment were used (for example, sealed, opaque, numbered envelopes) and otherwise as inadequate (for example, alternation).21 Outcomes assessment was rated as blinded if data were collected either by researchers blinded to intervention status or by postal survey. Subjects were not blinded in any trial. Differences were resolved by discussion.
ANALYSIS
Primary outcome measures included post-intervention proportions with owned, functional, newly acquired, and newly functional smoke alarms, and incidences of fires, burns, and fire related injuries. When data on acquisition of alarms or of functional alarms were unavailable, we estimated these data by subtracting pre- from post-intervention prevalence for each group. We planned subgroup analyses of the effects of (1) safety advice as part of routine child health surveillance; (2) discounted/free smoke alarms; (3) adequate allocation concealment; and (4) blinded outcomes assessment.
We performed meta analysis to combine odds ratios (OR) between intervention and control groups, using a random effects model.22 A test for heterogeneity,22 that is, whether observed differences among the results of included trials were greater than could be expected by chance, used a significance level of 10%. Except where specifically noted, there was no statistically significant heterogeneity. Results from non-randomised trials were not quantitatively combined.
No authors of cluster randomised trials provided cluster specific outcome data. We therefore reduced their subject numbers to “effective sample sizes”23 using published estimates for the intraclass correlation coefficient: 0.017 for medical practices24 and 0.02 for school classes.25 As sensitivity analyses we alternatively: (1) ignored clusters; and (2) used intraclass correlation coefficients five times larger than the above. Neither alternative materially affected the results (data not shown).
As further sensitivity analyses, we accounted for all randomised subjects whose outcomes were not assessed (when numbers randomised to each group were known) assuming: (1) all those lost to follow up had “positive” outcomes (for example, owned alarms post-intervention); and (2) all had “negative” outcomes (for example, did not).
Results
We found 4486 unduplicated citations in electronic databases. From these, we identified 118 potentially relevant citations. We found an additional 28 potentially relevant citations from other sources. We could not retrieve the full text of two studies,26 27 and nine were available only in abstract. Of 135 studies reviewed in full, 15 trials met all inclusion criteria,24 28-45 the eligibility of 16 could not be determined, and the remainder were excluded. To determine the eligibility of the nine abstracts and remaining 16 trials, we contacted all 24 authors. From 22 responses, we identified six eligible trials.46-51 We also found five trials in progress through organisational contacts (written communication, P Harvey, Centers for Disease Control and Prevention, 2 July 1998). Hence, we identified 26 relevant trials (tables 1 and2).
Summary of randomised controlled trials of interventions to promote smoke alarms
Summary of non-randomised controlled evaluations of interventions to promote smoke alarms
RANDOMISED CONTROLLED TRIALS
Main analyses
Among 13 randomised controlled trials, eight interventions were delivered in the clinical setting (including prenatal, well child, and parenting classes held in clinics and hospitals),24 28 30 33 44-47 four were delivered at home,36 48 50 51 and one in school31(table 1). Eleven have been completed.
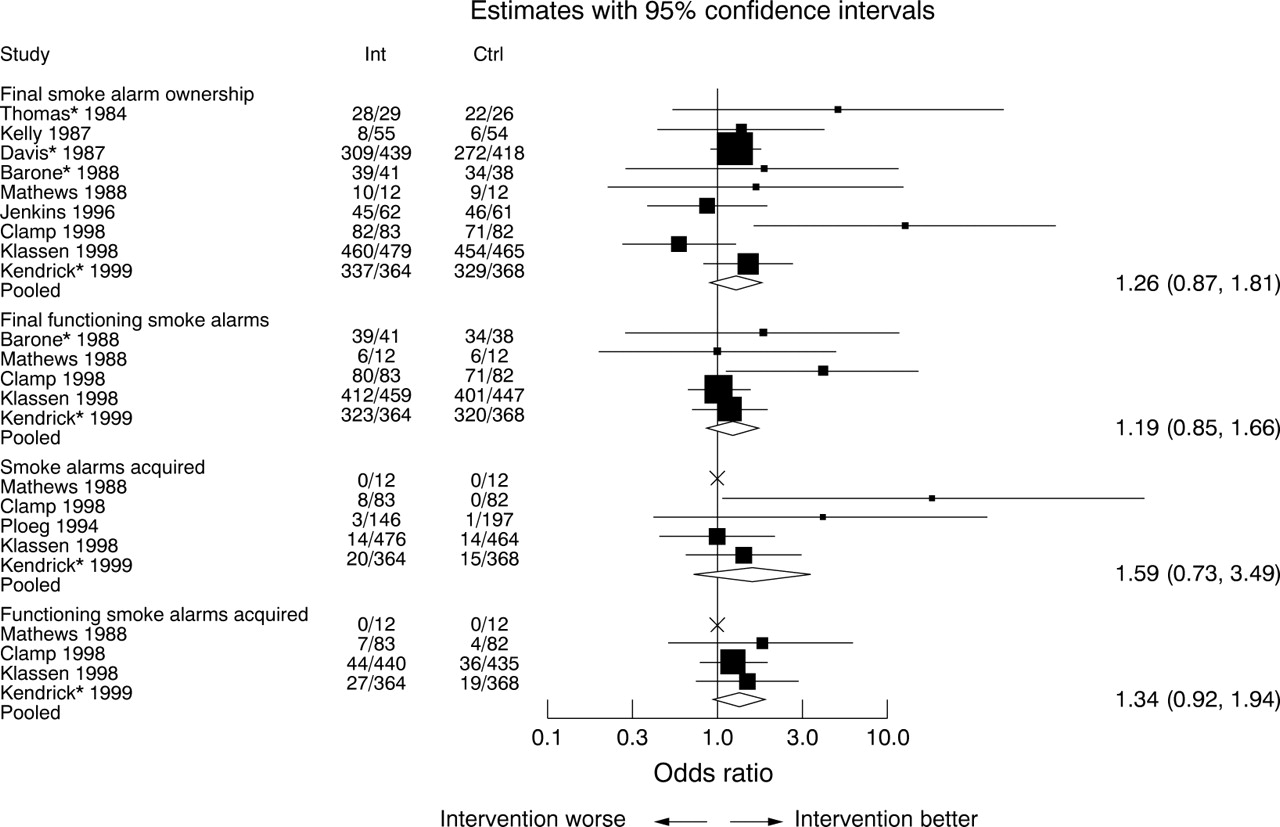
Ten completed trials collected data on smoke alarm ownership. We were unable to obtain these data from one trial,45 which reported “no significant difference” in alarm ownership between study groups. Combining the other nine trials, smoke alarm ownership at follow up appeared somewhat more likely in the intervention group (OR = 1.26; 95% confidence interval (CI): 0.87 to 1.81; fig 1). Similarly modest positive, statistically non-significant effects on functioning smoke alarms, and on new acquisitions of smoke alarms and functioning smoke alarms, were found (fig 1). Assumptions of all positive or all negative outcomes resulted in similar or even smaller effect estimates (data not shown).

{kind=link}
Effects of intervention on smoke alarm ownership, function, and acquisition: individual and combined odds ratios and 95% confidence intervals. *Cluster randomised trials, for which effective sample sizes were used in the analysis. The adjusted denominators used were as follows—Davis: 314 (I), 299 (C); Barone: 34 (I), 29 (C); Thomas: 28 (I), 25 (C), Kendrick: 274 (I), 277 (C). Box sizes indicate relative weights assigned to studies, which depend on sample size and on overall prevalence of smoke alarms.
Two trials collected injury outcomes,24 33 but fire related injury data were unavailable. None of the trials reported fire incidence.
Subgroup analyses
All five completed trials of safety advice as part of routine child health surveillance showed positive effects on smoke alarm ownership, function, and acquisition.24 28 30 33 44Among these, intervention families were more likely than control families to own an alarm (OR = 1.93; 95% CI: 1.04 to 3.59) and to have a functioning alarm (OR = 1.72; 95% CI: 0.78 to 3.78). There were strong, statistically non-significant effects on acquiring an alarm (with significant heterogeneity, p = 0.09) and acquiring a functioning alarm (data not shown), but these analyses were based on few trials and were heavily influenced by one trial.24
Four trial interventions combined discounted or free smoke alarms with education.24 30 44 48 Offering discounted alarms had a stronger effect on smoke alarm ownership (OR = 1.81; 95% CI: 0.63 to 5.19) than did education alone, but the trial results were significantly heterogeneous (p = 0.015). Effects on function and acquisition were similar to those in the main analyses (data not shown).
Among five trials with inadequate (or unstated) allocation concealment,28 31 33 36 44 the combined effect of intervention on smoke alarm ownership (OR = 1.33; 95% CI: 0.97 to 1.82) was only slightly higher than that in trials with adequate concealment (OR = 1.22; 95% CI: 0.56 to 2.65, with significant heterogeneity, p = 0.025).24 30 47 48 There was even less difference between trials with and without adequate allocation concealment in the effect of intervention on functioning alarms (data not shown).
Among trials with unblinded (or unstated) outcomes assessment, smoke alarm ownership and function were substantially more likely with intervention (OR = 2.1; 95% CI: 0.94 to 4.69, and OR = 2.21; 95% CI: 0.91 to 5.39, respectively). However, among trials with blinded outcomes assessment,24 33 47 48 50 intervention had little effect on ownership (OR = 1.01; 95% CI: 0.64 to 1.59) or function (OR = 1.07; 95% CI: 0.77 to 1.49).
NON-RANDOMISED CONTROLLED TRIALS
Of 13 non-randomised controlled trials, eight are completed (table2). Two evaluated safety advice during routine child health surveillance visits40 49 and one evaluated education during mandatory tenants' meetings.37 The other five evaluated community programmes involving mass media, school or community education, clinical counselling, free smoke alarms, and/or alarm installation.29 32 34 35 38 39 41-43Allocation concealment was rated inadequate for all non-randomised trials.
Smoke alarms
Five completed trials reported smoke alarm outcomes (table2).32 40-43 49 Two involved safety advice during routine child health surveillance.40 49 Results of one of these were similar to those from randomised trials reported above.40 The other trial reported modest effects from free smoke alarms but none from counselling alone.49 However, post-intervention ownership in all groups was greater than 95%, and the study did not control for significant differences among groups in home ownership, education, and income, all of which are associated with alarm ownership.52
Two trials of community wide injury prevention education reported no effects on alarm ownership32 or installation41 42 (table 2). In contrast, installation of free smoke alarms increased the prevalence of functioning smoke alarms by 19% (table 2).43 In the latter trial, efforts were made to match intervention and control areas on injury rates, sociodemographic characteristics, and geographical location, to reduce the likelihood of selection bias.
Fires
After a mandatory lecture and video targeting fire safety and prevention, fire incidence in intervention (new tenant) households was one fifth that in control (existing tenant) homes (table 2), even though, before intervention, fire incidence was higher in new tenancies than in existing ones.37 Community wide distribution of fire prevention brochures with free smoke alarms had little effect on fire incidence (table 2), although the intervention and control areas differed significantly in their fire injury risks prior to intervention.35
Fire related injuries
Four community trials measured burns or fire related injuries (table 2).29 32 34 35 38 39 43 After direct provision (with or without installation) of free alarms, fire related injury rates fell significantly in intervention communities but not in control communities (written communication, D Schwarz, Children's Hospital of Philadelphia, 17 July 1998).35 43 In one trial, however, the intervention area was selected because it had the highest baseline injury rate, hence regression to the mean may explain some of the decline.35
Community injury prevention education produced a modest, non-significant effect on burn injuries,29 32 and there was no apparent benefit from community burn prevention education.34 38 39 Because these trials assessed all types of burns but excluded smoke inhalation, results are not directly comparable to those from the trials of alarm give away programmes, which assessed fire related injuries.
Discussion
Evidence from randomised controlled trials indicates that, in general, counselling or education to promote smoke alarms is likely to have only a modest effect, if any, on smoke alarm ownership, function, or acquisition. The results were sensitive to decisions on imputation of missing data and to study quality. In particular, trials with blinded outcome assessment showed no apparent effect from educational interventions.
Stronger (and statistically significant) effects were seen among trials evaluating counselling in the context of routine child health surveillance. Based on our results, the estimated number of families clinicians would have to counsel to influence one additional family to own a smoke alarm varies with the baseline practice prevalence: seven families if 50% own alarms, 13 families if only 10% own alarms, and 22 families if 90% already have alarms. Effects on the prevalence of functioning smoke alarms from clinical counselling were less clear. Moreover, several of the trials of child health surveillance used unblinded outcomes assessment, which may have biased their results upward.
Although observational studies support a substantial beneficial effect of smoke alarm ownership on fire related injuries,3-5there were no data from randomised controlled trials on the effects of counselling or education on fire related injuries. Because fire related injuries are the second leading cause of injury death in childhood, the net benefit of educational or counselling interventions may be important. However, its effectiveness and cost effectiveness in relation to fire injuries prevented has not been adequately evaluated.
Community trials suggest that providing free smoke alarms reduces fire related injuries. Because these trials were not randomised, however, selection bias or regression to the mean may have exaggerated their effects. Hence, the benefit of such programmes is not established. Non-randomised trials do not support a beneficial effect of mass media and community based injury prevention education on either smoke alarm ownership or burn incidence. One author attributed this to attenuation in the numbers who hear, then understand, then act on such information.39
EXPLORING HETEROGENEITY
Although there was no statistically significant heterogeneity in the main analysis, subgroup analyses suggested important differences in results according to both setting (primary care versus other settings) and outcomes assessment methods. Post hoc examination of results suggests that variations in other factors may also influence results. In the only two trials involving families of injured children,47 48 ownership and acquisition were equally high in control and intervention families, so there was no apparent effect of intervention. Having an injured child may lead to safety behaviour changes so large that they obscure any safety education effects. Exclusion of these two trials results in a stronger, statistically significant intervention effect on alarm ownership (OR = 1.43; 95% CI: 1.07 to 1.90) and other alarm outcomes. The trial of Klassen et al 48 was also the only one in which the intervention was delivered by a research assistant. When this trial is excluded, there is a stronger positive effect of intervention on smoke alarm ownership (OR = 1.36; 95% CI: 1.02 to 1.82), functioning smoke alarms (OR = 1.44; 95% CI: 0.85 to 2.43), and alarm acquisition (OR = 2.85; 95% CI: 0.72 to 11.25). The relation established between the family and their doctor, nurse, or teacher may be an important aspect of effective intervention, a hypothesis supported by the subgroup analysis of routine child health surveillance.
Finally, in one trial24 the response rate was notably poor (table 1) and there was systematic response bias, in that control responders were more likely than intervention responders to live in rented accommodation, have lower socioeconomic status, and live in deprived areas (written communication, D Kendrick, University of Nottingham, 2 September 1999). Because these factors are associated with reduced smoke alarm ownership,52 the estimate of the effect of the intervention might have been biased upwards. However, results were not materially affected by exclusion of this trial.
LIMITATIONS
Publication bias, which threatens the validity of systematic reviews, may arise if research is unpublished or if outcome data are selectively omitted from published reports, which often occurs because the results fail to reach statistical significance.53 54To minimise this, we searched for unpublished trials and wrote to the authors of any trials in which the methods and intervention were eligible, to ask whether relevant outcomes were measured. Twelve trials were identified after author and organisational contacts, including five completed trials.24 47-50 Many investigators also provided unpublished data on smoke alarm or injury outcomes.24 30 32 43 47 48 50 51
The two authors of three potentially eligible trials did not respond, so we were unable to determine their eligibility. We could not locate the text or authors for two further citations. Four of these were known to be non-randomised, and the fifth,26 as a community intervention, was probably non-randomised. Hence, their omission should not have biased our meta analyses.
CONCLUSIONS
Our review suggests only modest potential benefits from education to promote smoke alarms. Smoke alarm promotion delivered as part of child health surveillance may be more effective. However, several studies on which these conclusions are based suffered from methodological weaknesses. In addition, effects on fire related injuries and cost effectiveness have not been studied.
While community programmes that provide and install smoke alarms appear to reduce fire related injuries, the quality of that evidence is limited. Further trials to evaluate the effect of smoke alarm promotion as part of child health surveillance in primary care, or of community smoke alarm distribution, should assess their impact on fire related injuries, using adequate allocation concealment and blinded outcomes assessment.
Acknowledgments
We thank the investigators who responded to our queries and Dr Ian Roberts for advice and data extraction. Dr DiGuiseppi was funded by the Camden and Islington Health Authority, and Dr Higgins by the National Health Service Research and Development Directorate.
References
Linked Articles
- Archives this month