Article Text

Abstract
Background Traumatic brain injury (TBI) in older adults leads to considerable morbidity and mortality. Outcomes among older adults with TBI are disparately worse than in younger adults. Differences in immunological response to injury may account for at least some of this disparity. Understanding how ageing differentially affects the immune response to TBI and how older age and these immunological changes affect the natural history of recovery following TBI are the goals of this study.
Design/methods A prospective multiple cohort design is being used to assess the effects of ageing and TBI on immune makers and to test predictors of impairment and disability in older adults following mild TBI. Older adults (>55 years) with mild TBI are enrolled with three comparison groups: younger adults (21–54 years) with mild TBI, non-injured older adults (>55 years) and non-injured young adults (21–54 years). For the primary analysis, we will assess the association between immune markers and Glasgow Outcome Scale-Extended at 6 months, using logistic regression. Predictors of interest will be inflammatory biomarkers. Multivariate linear regression will be used to evaluate associations between biomarkers and other outcomes (symptoms, function and quality of life) at 3 and 6 months. Exploratory analyses will investigate the utility of biomarkers to predict outcome using receiver-operating characteristic curves.
Discussion A better understanding of the recovery trajectory and biological rationale for disparate outcomes following TBI in older adults could allow for development of specific interventions aimed at reducing or eliminating symptoms. Such interventions could reduce impairment and healthcare costs.
- brain injury
- older adult
- cohort study
- disability
- biomarkers
- immune function
Statistics from Altmetric.com
Introduction
Traumatic brain injury (TBI) in older adults is common, accounting for over 25% of brain injuries in the USA each year and results in considerable mortality, long-term impairment and disability.1 The vast majority (>75%) of these injuries are considered mild.2 Outcomes among older adults with TBI are worse when compared with their younger counterparts with similar injuries. Clinical efforts to treat TBI in older adults have not yielded the expected improvements in outcome.3 These poor outcomes may be due, in part, to the inability to identify those older adults most vulnerable to adverse outcomes early so that interventions, such as rehabilitation, can occur in a timely manner. A critical barrier to the management of TBI is the limited knowledge about potential differences that results from ageing in the response to TBI, and how older age may affect pathology and recovery following TBI.
To date, relatively little is known about the trajectory of symptoms experienced by older adults following mild TBI. Recent studies demonstrate that being older and female is associated with an increased likelihood of developing symptoms as well as the number and type of symptoms.4–8 It is unclear if age or other factors (gender, social support) contributed to the resulting impairment as these factors have not been evaluated. Information on the functional status of older adults following mild TBI is limited. In studies that have examined impairment or disability following TBI in adults, there is evidence to suggest that older adult survivors of TBI have increased dependence as measured by global outcome instruments such as the Glasgow Outcome Scale (GOS)9–11 compared to younger patients with TBI. Adults older than 50 years of age had the highest disability at 1–2 years following TBI,12 further emphasising the long-term functional implications of this disease. Our study will provide critical knowledge regarding the natural history of recovery following TBI in older adults.
Inflammation is one of the primary immune responses of the brain to TBI. Both chemokines and cytokines are released both locally at the site of injury and systemically in response to injury.13 14 Increases in proinflammatory chemokines and cytokines have been reported following experimental and clinical TBI and may be causally related to sequelae of injury.15–21 ‘Sickness behaviour’ is a normal homeostatic syndrome that occurs in response to proinflammatory cytokines in the brain22 23 and is not attenuated with steroid administration.24 Sickness behaviours include decreased activity and socialisation and reduced appetite. Therefore, there is a known physiological and causal mechanism for symptom development that is associated with cytokine release following experimental TBI, making it an appropriate area for investigation and potential intervention. Studies indicate that the concentrations of inflammatory cytokines following TBI vary according to the time postinjury,25 but little information is available regarding inflammatory cytokines in the postacute phase. Furthermore, the natural history of cytokine expression is not well characterised in large clinical samples of adults/older adults.26 No study has identified if symptoms that are present following injury could be correlated to changes in inflammatory cytokine concentrations or impaired cellular immune response. Blood biomarkers show promise for prediction of outcome from TBI,27 but have not been evaluated for prognostic purposes in older adults.
Ageing itself has been described as state of immunosenescence, characterised by changes in innate immunity and a chronic low-level proinflammatory status.28 29 These changes have been associated with higher morbidity and mortality.28–31 Cognitive dysfunction and fatigue are also linked to immune changes induced by traumatic injury, but the relationship of these symptoms to immune and inflammatory markers in an older population remains unexplored. In this study, we will test a model of impairment and disability following mild TBI in older adults based on the Institute of Medicine’s Disability Framework32 33 in which ageing is a biological factor that contributes to the pathological response following TBI by modulating the immune response. This increase in inflammation, in turn, is hypothesised to correlate with the increased symptom burden, increased functional limitation and disability and poorer quality of life reported in older adults following TBI.
A better understanding of the trajectory of recovery is important in the prediction of outcomes and the development of interventions for management of symptoms and reduction of disability following mild TBI in older adults. Biomarkers could provide important tools for screening and estimating impairment severity and determining the need for further resources or treatment.
Methods
Study design
A single-centre prospective multiple cohort design is being used to assess the effects of ageing and TBI on immunological biomarkers and to test predictors of impairment and disability in older adults following mild TBI. TBI study participants (Groups 1 and 2) are being recruited within 24 hours of injury from Harborview Medical Centre, Seattle, Washington, USA, an urban level I regional trauma centre. Age-matched and gender-matched non-injured controls (Groups 3 and 4) are recruited from the community. Study findings will be reported in accordance with the STROBE statement.34 Approval for the study was provided by the Human Subjects Division of the University of Washington IRB #41718.
Study site and recruitment
Older adults (>55 years of age) with mild TBI (Group 1) are enrolled with three comparison groups: younger adults (21–54 years of age) with mild TBI (Group 2), non-injured older adults (>55 years of age) (Group 3) and non-injured young adults (21–54 years of age) (Group 4). The decision to use 55 years of age as the cut point for younger and older adults was based on the trauma literature since it appears to be an inflection point for increased mortality after trauma.35 36 In order to achieve the most representative sample of patients who present to the emergency department (ED) for treatment for mild TBI, we are enrolling subjects prospectively in a consecutive manner. Patients seeking treatment for traumatic injury are screened for initial eligibility by trained research staff working in the ED. Written informed consent is obtained from all participants or their legally authorised representative at time of enrolment.
To be eligible, older adult mild TBI subjects (Group 1) must have a clinical diagnosis of mild TBI from blunt trauma within the past 24 hours based on CDC criteria (see box 1)1; be ≥55 years of age; speak and read English and have a documented home address within western Washington State. Younger mild TBI subjects (Group 2) will meet the same criteria as Group 1, but must be 21–54 years of age.
Clinical diagnosis of mild TBI1
Signs and symptoms consistent with a diagnosis of mild TBI (require one or more of the following):
confusion or disorientation,
amnesia near the time of the injury and Glasgow Coma Scale (GCS) of 15 by 24 hours,
a loss of consciousness up to 30 min,
neurological or neuropsychological problems and/or
an initial score of 13 or higher on the GCS.
Inclusion and exclusion criteria were developed to maximise generalisability. In order to increase the likelihood of subjects from all groups completing the protocol, we exclude those persons (1) planning to leave the area within 6 months or (2) who have a documented estimated life expectancy <6 months. Persons taking drugs that might alter the inflammatory response, (3) oral or injectable steroids within the last 30 days, Non-steroidal anti-inflammatory agents (NSAIDS) more than 3 days per week, COX-2 inhibitors, biological inhibitors of cytokines and other immune modulating agents will also be excluded. As the following conditions significantly alter the recovery pattern from mild TBI, we exclude persons who have: (4) cervical spine trauma at time of injury; (5) previous TBI or stroke in the past year; (6) previous history of dementia. Given the known differences in outcomes between blunt and penetrating injury, we exclude individuals with (7) penetrating head injury as a mechanism. (8) In order to better distinguish the effects of TBI from non-head injury, we exclude (8) persons with injuries to other body regions that are classified as greater than a moderate injury (Abbreviated Injury Scale>2).37
In order to achieve a control sample that most closely represents the injury populations related to transitional factors (figure 1), non-injured older adults (Group 3) and non-injured younger adults (Group 4) are recruited by having injured individuals identify a non-injured friend of similar age to participate. In instances where an individual is unwilling or unable to identify a friend to be approached for study participation, the remainder of the control sample are recruited from the local community. In order to be eligible, non-injured older adult subjects (Group 3) must: (1) be ≥55 years of age; (2) independently perform all activities of daily living;38 (3) speak and read English and (4) have a documented home address and telephone number within western Washington State. Eligibility for non-injured younger adult subjects (Group 4) is the same as Group 3, but 21–54 years of age. As we are seeking healthy non-injured controls, persons with: (1) previous TBI or stroke by self-report in the past year; (2) hospitalisation within the past 6 months or (3) history of dementia are excluded from Groups 3 and 4. Finally, participants in the control groups are excluded if they are taking immune modulating medications (the same as in Groups 1 and 2) at the time of screening.
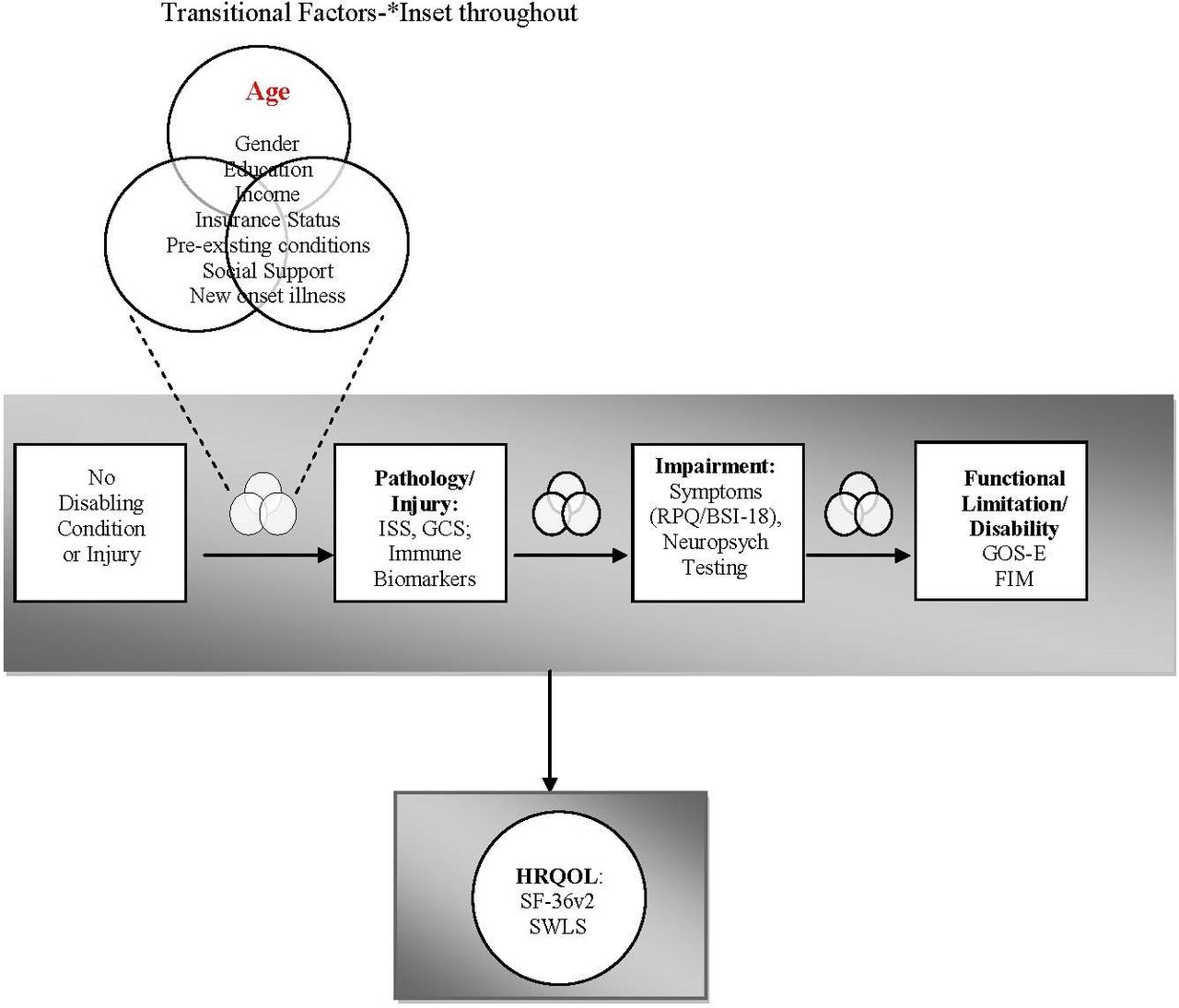
{kind=link}
Conceptual model for development of impairment and disability in older adults following TBI. Ageing is a biological factor that may contribute to the pathological response to TBI by modulating the immune response. These immune changes are, in turn, associated with the increased symptom burden (impairment), increased functional limitation and disability and poorer health-related quality of life (HRQOL) reported in older patients following TBI. Transitional factors are those variables that may either promote or prevent an individual from moving through the stages of acquiring disability. BSI-18, Brief Symptom Inventory-18; GCS, Glasgow Coma Scale;GOS-E, Glasgow Outcome Scale-Extended; ISS, Injury Severity Score; RPQ, Rivermead Postconcussion Symptom Questionnaire; SWLS,Satisfaction with Life Scale; TBI, traumatic brain injury.
Procedures
Traumatic brain injury subjects (Groups 1 and 2)
Day 0, 3, 7
Blood samples are collected at time 0 in the ED or hospital for immune biomarkers. The timing for the initial day 0 sample is as close as possible to time of admission to the ED, within 24 hours of injury. Data on demographics, injury data (type, location, mechanism and severity) are extracted from the medical record. Questionnaires are administered for assessment of preinjury functional limitations and health-related quality of life as indicated by the protocol (see tables 1 and 2). Data regarding new medications, ED visits or rehospitalisations are also collected.
Research protocol
Summary of measures
1, 3 and 6 month postinjury visits
Questionnaires are administered for assessment of impairment, functional limitations/disability and HRQOL as indicated by the protocol (see tables 1 and 2). Blood is sampled at each visit. Data regarding changes in health status (new medications, conditions, ED visits, surgery or hospitalisation are also collected.
Blood sampling procedures
Twelve millilitres of blood will be collected from each subject and samples are transported for processing within 4 hours of collection. Two EDTA-containing (Becton-Dickinson) tubes are used to collect blood samples for plasma and peripheral blood mononuclear cell (PBMC) isolation. Following collection, tubes are then centrifuged at 1000×g for 10 min at room temperature in order to separate plasma from the buffy coat interface. Plasma is stored at −70°C until batch evaluation. Ficoll gradient technique is used to isolate PBMCs from the buffy coat layer. Once the cell pellet is obtained, it is washed and cell viability and counts are obtained. The cells are adjusted to a concentration of 107 cells per mL with complete Freezing Media (Fetal Calf serum containing 10% dimethyl sulfoxide [DMSO]) in storage vials (1 mL per vial). These tubes are then put into a room temperature Slo-Cooler box and placed in a −70°C freezer overnight. The next day, these tubes are transferred into liquid nitrogen for long-term storage until batch analysis.
Non-injured Controls (Groups 3 and 4)
Following initial screening via telephone, the subject meets with research staff to obtain informed consent, answer questionnaires and have neuropsychological testing (tables 1 and 2). A blood sample is drawn for immune markers at this visit (Day 0). 1, 3 and 6 month visits occur as per table 1.
Measures
Demographic characteristics
All subjects will be asked about their age, gender, race/ethnicity, formal educational achievement, income level, insurance status and pre-existing conditions. In studies of persons with severe TBI, their preinjury level of functioning was found to be more predictive of outcome than the actual injury severity39 and therefore both of these variables will thus be considered as covariates in our analysis. Further, age, lack of or public insurance (Medicaid), lower income and lower levels of social support have been related to lower HRQOL at 12 months post-TBI40 41 and will therefore also be considered as transitional factors influencing the development of disability and changes in HRQOL.
Inflammatory cytokine/chemokine measurements
Multiplex cytokine assay using a fluorescent microsphere suspension array will be used to detect and quantify protein concentrations of selected inflammatory markers.
Cellular immune response
ELISpot will be performed on bulk PBMCs. In order to determine the number of PBMCs producing interferon (IFN)-γ in response to stimulus, cells will be plated in 96-well plates (Millipore) previously coated with primary antibody along with 10 uL of stimulant (lipopolysaccharide or phytohemagglutinin) or control (media alone) following the protocol of Hagiwara and colleagues.42 All experiments will be performed in triplicate. Cells secreting INF-ʏ when cultured produce a coloured spot in response to the immune assay within the well. Spots will be counted by two independent investigators blinded to group aided by a semiautomated software system.
Impairment, disability and health-related quality of life
We consulted the National Institutes of Health/National Institute of Neurologic Disorders and Stroke common data elements for TBI to select outcome measures and include all recommended core measures within the domains of impairment, function/disability and HRQOL (see table 2).
Analysis
Measurements of inflammatory cytokines will be log-transformed in order to obtain normality of distribution within groups. Means, SD and distributions will be used to describe cellular immune and inflammatory biomarkers, impairment, functional limitation/disability and HRQOL at each time point. Data will be examined to determine if baseline characteristics of those persons lost-to-follow up differ from those participants who complete the protocol. Multiple imputation techniques43 will be used to manage missing data. Sensitivity analyses, for example, counting those lost-to-follow up as all having a poor outcome or all having a good outcome will indicate the degree to which lost-to-follow up may sway outcome in the analyses.
Transitional factors such as gender, income, insurance type, education, preinjury morbidity (preexisting conditions and function), social support (MOS SSS) and insurance status may be confounders; if they are related to group (p<0.10), they will be treated as covariates in all analyses addressing impairment, functional limitations/disability and HRQOL. To reduce the effects of sample heterogeneity, in all analyses of TBI subjects, we will adjust for additional covariates to include: pupil reactivity and presence of a significant extracranial injury (Injury Severity Score) as per the basic recommendations of the MRC CRASH trial collaborators.44 To adjust for multiple comparisons, we will use the Benjimini-Hochberg testing procedure.45 We will collect data at each visit from the medical record and from subject reports of any new onset or change in illness that could be potential confounders (eg, new medications, surgeries, infections, acute hospitalisations) and determine if any additional adjustment is required between groups.
For the primary analysis, we will assess the association between biomarker concentrations and GOS-E at 6 months, using ordinal logistic regression per the IMPACT study group recommendations (proportional odds methodology). The predictors of interest will be (a) log-transformed inflammatory biomarker concentrations and (b) cell counts. Included in the model will be the aforementioned covariates. Multivariate linear regression will be used to evaluate associations between biomarkers and other outcomes (symptom scores, neuropsychological function, FIM and HRQOL) at 3 and 6 months. We will use error-in-variables regression to account for measurement error in the predictor variable (biomarker) if indicated. Exploratory analyses will investigate the prognostic utility of biomarkers to predict poor outcomes following TBI using receiver-operating characteristic curves.
Linear mixed models for longitudinal data46 will be used to estimate (1) geometric mean number of cells and (2) inflammatory biomarker concentrations and mean impairment, disability and HRQOL across time for the four groups adjusted for covariates (vide supra). Time will be modelled as a categorical variable to detect non-linear effects over time. This model will allow for estimating the response to injury relative to a non-injured control for both younger and older adults. The interaction of age group and injury group will indicate whether there is a more extreme injury effect in older adults. To compare immune function and outcomes among older and younger TBI subjects, a second set of linear mixed models will be used to model immune biomarkers (Th1 response or cytokine concentrations) and outcomes, restricted to groups 1 and 2, which will have more observations per individual. These models will include transitional and injury covariates.
Sample size
Based on pilot data for the biomarkers and assuming a conservative α of 0.0125, we will have 90% power to detect a difference of ±0.6 in log-transformed cytokine concentrations between older and younger adults with TBI with 75 participants in each of the four groups (n=300). This corresponds to one group having four times the cytokine concentration of the other. We will also have will 90% power to detect correlation coefficients greater than 0.42 between biomarkers and functional outcomes with 75 participants in each group. Based on SD estimates for markers and outcomes obtained from our pilot data, we will be able to detect a 40% increase in odds of a worse outcome on the GOS-E given a twofold difference in a biomarker.
Discussion
This study will lead to an increased understanding of the natural history of the recovery and disability trajectory following mild TBI in older adults and hopefully aid in prediction of outcome as well as clinical care. This study will potentially identify biological predictors of poor outcome in older adults with mild TBI that are worthy of follow-up in subsequent studies. The proposed study will begin to examine mechanisms underlying symptoms and functional impairment experienced by older adult patients following TBI to determine if they are associated with changes in cellular immune function and cytokine concentrations. Biomarkers could provide an important tool for delineating the degree of impairment and determining the need for further resources or treatment. Importantly, biomarkers could provide indirect measures of treatment response for use in clinical trials and treatment.
Acknowledgments
We would like to thank Drs John Amory, Patrick Heagerty and Jeffery Probstfield for critical input on the study design as it evolved through the ITHS KL2 program.
References
Footnotes
Contributors HJT was responsible for the initial conception and drafting of the work. All listed authors made substantive contributions to the study design and revision of the work. All authors approved the final version.
Funding This work was supported by the National Institute of Neurological Disorders and Stroke of the National Institutes of Health under award number R01NS077913.
Disclaimer The content is solely the responsibility of the authors and does not necessarily represent the official views of the National Institutes of Health.
Competing interests None declared.
Patient consent for publication Not required.
Ethics approval University of Washington Institutional Review Board.
Provenance and peer review Not commissioned; externally peer reviewed.
Data availability statement There are no data in this work.