Article Text

Abstract
Objectives To estimate the likelihood of recovery at 1, 4 and 12 months post injury and investigate predictors of recovery in injured people attending an emergency department (ED) or admitted to hospital in the UK.
Methods Participants completed questionnaires at recruitment and 1, 4 and 12 months post injury or until recovered. Data were collected on injury details, sociodemographic characteristics, general health prior to injury and recovery. We compared three age groups: 5–17, 18–64 and 65 years and above. Modified Poisson regression estimated the relative risk of recovery. Multivariable models were built using backward stepwise regression. Sensitivity analyses assessed the effect of missing data.
Results We recruited 1517 participants, 55% (n=836) ED attenders and 44% (n=661) hospital admissions. By 1 month after injury, 28% (285/968) had fully recovered, 54% (440/820) at 4 months and 71% (523/738) at 12 months. Recovery was independently associated with gender, admission status, injury severity, body region injured and place of injury for 5–17 year olds and 18–64 year olds and with gender, admission status, injury severity and long-term illness for those aged 65+. Injury severity and hospital admission were associated with recovery across all age groups, but not at every time point in each age group. Other factors varied between age groups or time points. Results were generally robust to imputing missing data.
Conclusions A range of factors was found to predict recovery among injured people. These could be used to identify those at risk of delayed recovery and to inform the design of interventions to maximise recovery.
- Outcome of Injury
Statistics from Altmetric.com
Introduction
In England injuries generate approximately 3.2 million visits to emergency departments1 and 0.8 million hospital admissions annually,2 representing a substantial burden on health services. Physical injuries requiring medical treatment frequently have substantial and long-term consequences. For the individual, injuries often result in psychological distress arising directly from the injury3–5 and indirectly from longer-term physical problems such as chronic pain,6 ,7 disability or physical limitation.7–9 Injury sequelae may be of short-term or longer-term duration with psychological morbidity or physical disability reported up to 84 months post injury.10 Injuries can also impact on the individual's family with family members experiencing psychosocial 11 ,12 and financial problems.13 During 2010/2011, 4.4 million work days were lost in the UK due to workplace injuries alone.14 Societal costs include days lost at work and increased healthcare use15 and consequent costs16 ,17 as a result of injury.
To minimise the burden of injury-related outcomes, it is advantageous to assist recovery and identify factors associated with recovery so that interventions can be developed and implemented. However, predicting recovery from injury is complex with individual, contextual and population-based factors all influencing injury outcome,18 ,19 including expectations of recovery.20 Previous studies indicate a range of factors associated with injury recovery including injury severity,21–24 sex, with females reporting poorer outcomes,10 ,22 ,25 ,26 comorbidity,9 ,21 ethnicity with non-Caucasians experiencing poorer recovery10 and age where greater age is associated with poorer recovery.9 ,10 ,21 Recovery from injury in older people is also significantly associated with social support.19
The objective of the analyses presented here is to examine predictors of recovery among those with a range of injuries of varying severity presenting to emergency departments (EDs) or admitted to hospital in the UK, using data from the UK Burden of Injury study (UKBOI).27
Methods
The methods of the UKBOI study have been described in detail in the published protocol.27
Study design
The UKBOI study was a prospective longitudinal study set in four acute National Health Service (NHS) Trusts in Swansea, Nottingham, Bristol and Guildford.
Participants
Participants were people aged 5 years and over attending EDs or admitted to participating hospitals with any injury regardless of intent. This included a wide range of injuries, for example, fractures/dislocations, lacerations, bruises/abrasions, sprains, burns/scalds, and head, eye, thorax and abdominal injuries.27 ,28 Injuries had to have occurred within 2 weeks of attendance for patients treated in the ED and 4 weeks for patients admitted to hospital. Participants had to be able to give consent and complete questionnaires or have a proxy who could assent to their inclusion and agree to complete future questionnaires. Those without permanent UK addresses were excluded. Participants were recruited face-to-face during hospital admission or ED attendance between September 2005 and April 2007 until the required sample size (as described in the published protocol27) was achieved.
Data collection
Participants completed questionnaires at recruitment and by post at 1, 4 and 12 months post injury. Those reporting full recovery at any time point were not sent further questionnaires. Questions included injury circumstances, place of injury, motor vehicle involvement and injury intent. Sociodemographic data included questions on accommodation type, number of rooms, people and cars in household, ethnic group and employment status. The participant's postcode was obtained at recruitment, and from this, the Townsend deprivation score was obtained.29 Disability or long-term health problems limiting usual activity prior to the injury was ascertained using a dichotomous question. Follow-up questionnaires collected data on recovery, ascertained by asking whether the injury still affected the participant in any way on the day of questionnaire completion, with response options of ‘Yes, my injury still affects me’ or ‘No, I have completely recovered’. Data on body part injured and severity was ascertained from medical records and scored using the Abbreviated Injury Scale (AIS).30 Where participants had more than one injury, they have been categorised by the most severe injury.
Statistical analysis
Participant characteristics are described and comparisons between responders and non-responders at follow-up time points were made using χ2 tests for categorical variables and two-sample t tests or Mann–Whitney U tests for continuous variables as appropriate.
We ran separate analyses for three age bands: 5–17, 18–64 and 65 years and above, as previous studies suggest recovery varies by age. As the outcomes (recovery at 1, 4 and 12 months) were commonly reported, modified Poisson regression, with a robust variance estimator31 ,32 was used to estimate the relative risk of recovery at each time point. Multivariable models were built using backward stepwise regression forcing age, gender and study centre into the model and retaining other variables if the Wald test for their removal was significant (p<0.05). Deprivation was categorised in tertiles as it had a non-linear relationship with recovery. Injuries were grouped using the Dutch 13 group classification.33 As there were only small numbers of participants within some of these groups, we further categorised these 13 groups by body region into upper limb, lower limb and other injuries. This is consistent with findings from a recent individual level meta-analysis of health status post injury demonstrating different recovery patterns for upper and lower limb fractures and similar recovery patterns for dislocations, sprains and strains as for limb fractures.34 Injury severity was categorised into minor (AIS=1), moderate (AIS=2) and severe (AIS=3). As the number of severe injuries was small, moderate and severe injuries were combined. Observations with missing data were excluded. Models were checked for collinearity. Sensitivity analyses assessed effects of missing data using multiple imputation and combining imputed datasets using Rubin's rules.35
Results
Participants and baseline characteristics
We recruited 1517 participants at baseline, a participation rate of 66%.28 There were 818 (54%) male and 699 (46%) female participants, with 298 (20%) participants aged less than 18 (60%) aged 18–64 and 305 (20%) aged 65 and over. In all, 55% of participants (n=836) only attended the ED and 44% of participants (n=661) were admitted to hospital. Admission status was not known for 20 (1%) participants. There were 638 (42%) participants with minor injuries, 761 (50%) with moderate and 118 (8%) with severe injuries. Among participants with minor injuries 147 (23%) were admitted to hospital, compared with 400 (53%) for moderate injuries and 114 (97%) for severe injuries.
Table 1 shows baseline characteristics in three age bands (5–17 years, 18–64 years and 65+). In the two younger age bands most participants were male (64% and 59%), but in those aged 65+ the majority (72%) were female. A higher proportion of older participants (68% in 65+ years) had moderate or severe injuries compared with the younger age groups (56% and 55%), and a higher proportion were admitted to hospital (56% in 65+ years compared with 34% and 43% in the younger age groups).
Characteristics of study participants at baseline by age group (column percentages)
Response rates during follow-up
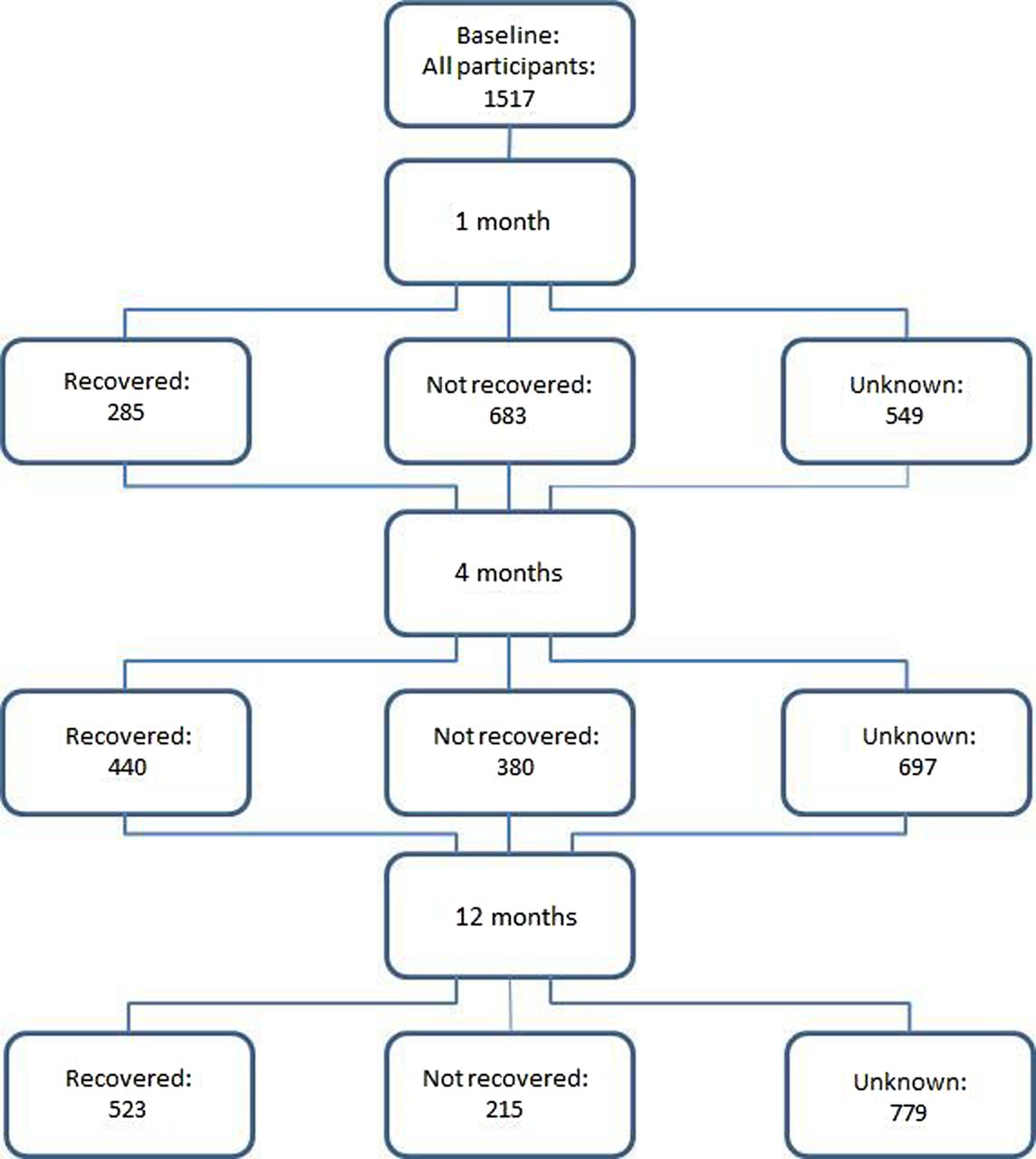
Figure 1 shows frequencies of responses at each follow-up time point. At 1 month, 968 participants (64%) returned questionnaires. At 4 months 535 responses (43%) were received from the 1232 participants who were not known to have fully recovered by this time point; 4-month outcome data were therefore available for 54% (820/1517) of participants, including those fully recovered at 1 month (n=285) who were not sent a 4-month questionnaire and were assumed to still be fully recovered at 4 months. At 12 months 298 responses (28%) were received from the 1077 participants who were not known to have fully recovered by this time point 12 month outcome data were therefore available on 49% (738/1517) of participants, including those fully recovered at 1 or 4 months (n=440) who were assumed to still be fully recovered at 12 months.

Frequencies of responses and recovery from injury during follow-up.
Comparisons between responders and non-responders at 1 month showed that responders, were older than non-responders (median 44 years vs 28 years, p<0.001), more likely to be female (51% vs 38%, p<0.001), less likely to live in the most deprived areas (27% vs 40%, p<0.001), had moderate or severe injuries (62% vs 50%, p<0.001), had more upper or lower limb fractures (30% vs 25% for upper, 37% vs 34% for lower, p=0.01) and were less likely to be injured at work/school, on the road or at a sports ground (work/school 14% vs 17%, road 19% vs 22%, sports ground 10% vs 13%, p=0.004). Similar patterns between responders and non-responders (excluding those known to have fully recovered at earlier time points) were found at 4 and 12 months. At 4 and 12 months there were also significant differences in response rates between the four study centres.
Patterns of recovery during follow-up
By 1 month after injury 28% (285/968) of respondents reported they had fully recovered (figure 1). Recovery rates were 54% (440/820) at 4 months and 71% (523/738) at 12 months. Recovery rates were lower for older age groups (figure 2).

{kind=link}
{kind=link}
Percentage recovered from injury during follow-up by age.
Univariate analysis: 5–17 year olds
Univariate predictors of recovery in participants aged 5–17 are shown in table 2. At each time point recovery rates were significantly lower in Nottingham compared with other centres, and were lower in participants admitted to hospital compared with ED attenders, with lower limb injuries compared with other injuries, moderate or severe injuries compared with minor injuries and those whose injuries had occurred at school or on the road, or at sports grounds compared with at home (1 month recovery only). Also participants aged 15–17 were less likely to have recovered at 1 month than participants aged 5–9 and males were more likely to have recovered at 4 months than females.
Univariate analysis of factors associated with recovery at 1, 4 and 12 months in participants aged 5–17 years (row percentages)
Univariate analysis: 18–64 year olds
Univariate predictors of recovery in participants aged 18–64 are shown in table 3. At each time point older participants were less likely to have recovered than younger participants, as were those admitted to hospital compared with ED attenders, those with lower limb injuries compared with other injuries, those with moderate or severe injuries compared with minor injuries and those whose injuries had occurred on the road compared with at home. Also at 1 and 4 months recovery rates were lower in Nottingham and Swansea compared with Bristol and Surrey and in participants with upper limb injuries than other injuries. Self-employed participants were more likely to have recovered at 1 month than participants in paid employment.
Univariate analysis of factors associated with recovery at 1, 4 and 12 months in participants aged 18–64 years (row percentages)
Univariate analysis: 65+ year olds
At each time point participants admitted to hospital compared with ED attenders, those with lower or upper limb injuries compared with other injuries, and those with moderate or severe injuries compared with minor injuries were less likely to have recovered. At 4 months males were more likely to have recovered than females (table 4).
Univariate analysis of factors associated with recovery at 1, 4 and 12 months in participants aged 65 and over (row percentages)
Multivariable analysis: 5–17 year olds
Multivariable analyses for all three age bands are shown in table 5. For 5–17 year olds only admission status and injury severity were associated with recovery at 1 month. Admitted participants were 44% less likely to have recovered at 1 month (adjusted relative risk (RR) 0.56, 95% CI 0.39 to 0.81) compared with ED attenders, and participants with moderate or severe injuries were 31% less likely to have recovered at 1 month (adjusted RR 0.69, 95% CI 0.54 to 0.88) compared with minor injuries. At 4 and 12 months recovery was less likely in participants admitted to hospital compared with ED attenders, in participants with moderate or severe injuries compared with minor injuries and in participants whose injury occurred at school compared with at home. Recovery was more likely in males and in those with upper limb injuries than those with other injuries.
Multivariable analysis of factors associated with recovery at 1, 4 and 12 months by age group (complete case analysis)
Multivariable analysis: 18–64 year olds
Admitted participants aged 18–64 years were 69% less likely to have recovered at 1 month (adjusted RR 0.31, 95% CI 0.20 to 0.48) compared with ED attenders, and participants with moderate or severe injuries had a 60% reduced chance of recovery at 1 month (adjusted RR 0.40, 95% CI 0.28 to 0.58) compared with those with minor injuries. Compared with injuries that occurred at home, recovery was less likely in participants whose injury had occurred on the road (adjusted RR 0.44, 95% CI 0.28 to 0.70) or at sports grounds (adjusted RR=0.45, 95% CI=0.27 to 0.74) and more likely in males than females (adjusted RR 1.41, 95% CI=1.08 to 1.83). At 4 months recovery was less likely in those who had been admitted compared with ED attenders, those aged 45–64 years compared with those aged 18–25 years, those with moderate or severe injuries compared with minor injuries, those whose injuries occurred on the road compared with at home and those with lower limb injuries compared with other injuries. At 12 months recovery was less likely in those who had been admitted compared with ED attenders, those aged 45–64 years compared with those aged 18–25 years and those with moderate or severe injuries compared with minor injuries.
Multivariable analysis: 65+ year olds
Older people with a long-term illness had a 57% reduced chance of recovery at 1 month (adjusted RR 0.43, 95% CI 0.25 to 0.76) compared with those without a long-term illness, while participants with moderate or severe injuries were 81% less likely to report recovery at 1 month (adjusted RR 0.19, 95% CI 0.11 to 0.32) compared with those with minor injuries. Participants with a long-term illness, those admitted to hospital and with moderate or severe injuries were less likely to have recovered at 4 or 12 months. Males were more likely than females to have recovered at 4 months.
Sensitivity analyses using multiple imputation
Using multiple imputation to replace missing values, the estimated proportions of participants who had recovered from their injury were 32% at 1 month, 52% at 4 months and 63% at 12 months. Estimated recovery rates were again highest in the youngest age group. At 1 month 55% of those aged 5–17 had recovered compared with 28% of those aged 18–64 and 20% in those aged 65+; at 4 months these were 73% in those aged 5–17, 49% in those aged 18–64 and 40% in those aged 65+; at 12 months 83% in those aged 5–17, 61% in those aged 18–64 and 51% in those aged 65+. The results of the multivariable analyses using imputed data were generally comparable with the results from the complete case analysis, although they differed in some instances (table 6, online only), for example in participants aged 5–17 after accounting for study centre, sex and age group, the only significant variables predicting recovery were admission status at 4 months and body region injured at 12 months.
Multivariable analysis of factors associated with recovery at 1, 4 and 12 months by age group using multiply imputed data (online only)
Discussion
Main findings
Recovery rates were lower for older age groups at all time points.. The majority of participants recovered by 4 months, with little further subsequent improvement. At 1 year after injury 9% of children and young people, 31% of adults and 43% of older people had not fully recovered. Although responders differed from non-responders at each follow-up point on a range of factors, multiple imputation indicated similar recovery rates at 1 and 4 months in all age groups and that recovery rates at 12 months may overestimate the true recovery rates by between 6% and 8% points across the age groups.
Those with more severe injuries were less likely to recover than those with less severe injuries at each time point in all age groups. The strength of the association between injury severity and recovery reduced over time. Older people with more severe injuries were less likely to recover at each time point than those who were younger. After adjusting for injury severity, being admitted to hospital was associated with a lower risk of recovery at each time point for children and adults, and at 4 and 12 months follow-up for older people. The strength of the association reduced over time in all age groups.
Relationships between other factors and recovery varied. Males were more likely to recover from injury than females in all age groups, but not at all time points within each age group. Long-term prior illness was important for predicting recovery at each time point in older people, but not for children or adults. Place of injury was associated with recovery for children and adults, but not at all time points. Children and adults with upper limb injuries were more likely to recover and those with lower limb injuries were less likely to recover compared to other injuries in the medium to long term.
Strengths and limitations of the study
This is the largest UK study quantifying recovery from a wide range of injuries. We recruited two-thirds of eligible patients and have previously reported no major bias in the representativeness of admitted patients who had been recruited to the study, but among those attending an ED but not admitted to hospital study participants tended to have more severe injuries than non-participants.28 Our recovery rates may therefore underestimate the recovery rate among all secondary care attended injuries.
We included patients attending an ED who were recruited within 2 weeks of their injury and in order to enable those with very severe injuries to take part we included those recruited within 4 weeks of their hospital admission. Hence patients who attended an ED more than 2 weeks following their injury will not have been invited to participate in the study. The number of such patients is likely to be small as such injuries are encouraged to use primary care services in the UK. Such injuries are also likely to be more minor than those attending an ED sooner. This may therefore have resulted in overestimation of the effect of admission status on recovery, but as the numbers are likely to be small we consider it unlikely that this would impact substantially on our estimates.
Our response rates at 1 month are similar to a comparable UK study,23 better than comparable studies in The Netherlands,33 ,36 ,37 but lower than for a UK study of road traffic injury in ED attenders.38 Our response rates at 4 and 12 months are difficult to compare with other studies as we only sent questionnaires to those that were not fully recovered, whereas other studies sent questionnaires to all participants, regardless of recovery at earlier time points 23 ,33 ,36–38 or reported response rates using responders to the previous questionnaire as the denominator.37 ,38 While there was evidence of some response bias, multiple imputation suggests our estimates of recovery rates may be overestimated at 12 months, but those at 1 and 4 months are robust to taking account of missing data. Multiple imputation indicated that the factors associated with recovery were broadly comparable in the complete case analysis and the multiply imputed data analysis. Injury severity and hospital admission remained the two characteristics most consistently associated with recovery in all age groups, though were less associated with recovery over time. Male sex, body region injured, place of injury and limiting long-term illness remained significantly associated with recovery at some time points in some age groups, although patterns differed in some instances from those in the complete case analysis.
We defined recovery as the participant reporting their injury no longer affected them in any way. We chose this in preference to EuroQol five dimensions (EQ-5D) instrument scores as previous work has demonstrated conflicting findings regarding normalisation of health status scores (Short Form (36) Health Survey (SF-36)) to pre-injury levels at 6 and 12 months post injury.39 ,40 There was no follow-up of those reporting full recovery at the previous follow-up time point, assuming they remained fully recovered at subsequent time points. This may have failed to capture the later onset of, for example, psychiatric problems and our recovery rates may therefore be overestimated. We did not collect data on psychological or social factors which may affect recovery and which may provide explanations for some of our findings. Some of our negative findings may result from insufficient power; there were only small numbers of children not recovered at later time points and there were small numbers in some subgroups (eg, ethnic group, injury intent). Small numbers of specific types of injuries prevented exploration of the impact of these on recovery.
Comparisons with existing literature
Our recovery rates are similar to those found in similar populations comprising a wide range of injury types and severities.33 ,37 Our findings are consistent with a systematic review which found all studies reported improvements in health between 3 and 6 months post injury.41 Our findings are also consistent with this review and other studies in terms of age, 10 ,42 ,43 female gender,10 ,44 ,45 injury severity,38 ,43–46 hospitalisation45 and prior chronic illness.10 ,45 It is unsurprising that we found admission status and injury severity both independently predicted recovery. We measured Injury severity using the AIS, which was devised as a predictor of survival post injury. Injury survival and recovery are very different outcomes, and while injury severity will impact upon the recovery process, many other factors (eg, psychological, social, occupational factors or access to healthcare), which may be related to hospital admission, will also play a part.
Implications for practice, research and policy
This study has identified predictors of recovery from a wide range of injuries that result in ED attendance or hospital admission. These may be used to identify those at risk of a prolonged or incomplete recovery and who may benefit from more frequent clinical review, additional interventions or support. Further research is needed to explore psychological, social, occupational, financial and legal factors, which may all play a part in recovery to further improve the prediction models we have developed.
What is already known on this subject
-
The international literature indicates recovery from injury is associated with a range of clinical and non-clinical factors. Differences in health and welfare systems may limit generalisability of these findings between countries.
-
There is little existing literature examining factors associated with recovery from a wide range of injuries in the UK.
What this study adds
-
Recovery can be slow and incomplete. Most recovery occurs within the first 4 months but 29% of injured people have not fully recovered 1 year after injury and recovery rates are lower in older age groups.
-
Hospital admission, injury severity and gender were associated with recovery in all age groups. Body region injured and place of injury were also associated with recovery in children and working age adults and existing long-term illness with recovery in older people.
Device to prevent sports injury
A Chinese research team has developed running shoes fitted with a device to help joggers avoid injuries by detecting and transmitting signs of fatigue. Apparently fatigue causes the runner's posture to change, which is the main cause of sports injuries. The device combines the use of an accelerometer and a gyroscope with Bluetooth technology. It sends a warning message to the users’ mobile phone if it detects fatigue and reminds users to adjust their posture or to stop running. The technology is to be used by Nike to produce ‘smart’ running shoes.
Wet lab results
To demonstrate how difficult it is to rely on the legal limit for alcohol as an assurance of safety, and to show how much alcohol affects judgment and behaviour, an experiment was conducted in Wyoming. This so-called ‘Wet Lab’ found that by the time participants finished three alcoholic drinks, all were showing signs of impairment. At the end of a second round, each of the test subjects failed field sobriety tests even though some of their blood alcohol levels had not reached the legal limit.
Firearm violence research priorities
In 2010, more than 105 000 people were injured or killed in the USA as the result of a firearm-related incident. As reported previously, part of the problem is the curtailment of funds for research into firearm-related violence. To counter this, President Obama issued 23 executive orders directing federal agencies to improve knowledge of the causes of this type of violence and how it might be prevented. One of these orders directed the CDC to immediately begin identifying the most pressing research problems in this domain. A committee was convened whose agenda will include the characteristics of firearm violence, risk and protective factors, intervention strategies, gun safety technology, and the influence of video games and other media.
Acknowledgments
The authors would like to thank all patients who participated in the study and staff at the four participating hospitals for facilitating the conduct of the study.
References
Footnotes
-
Collaborators UK Burden of Injuries Study Group: S Brophy, A Evans, RA Lyons, S Macey, I Pallister: School of Medicine, Swansea University, Swansea, UK. B Carter, E Towner: Centre for Child and Adolescent Health, University of the West of England, Bristol, UK. N Christie: Centre for Transport Studies, UCL, London, UK. J Sleney: Department of Sociology, University of Surrey, Guildford, UK. C Coupland, L Groom, D Kendrick, C Mulvaney, S Smith: Division of Primary Care, University of Nottingham, Nottingham, UK. F Coffey: Emergency Department, Nottingham University Hospitals NHS Trust, Nottingham, UK.
-
Contributors DK was the principal investigator for the Nottingham site, contributed to study design, analysis plan, and interpretation of results and drafting of the paper. YV contributed to the analysis plan, undertook the analysis and contributed to the interpretation of the results and drafting of the paper. CC contributed to the study design, statistical analysis plan, and interpretation of the results and drafting of the paper. NC was the PI for the Surrey site and contributed to study design, interpretation of results, and drafting of the paper. RAL was the chief investigator for the UK Burden of Injuries study and PI for the Swansea site, contributed to study design, interpretation of results, and drafting of the paper. ELT was the PI for the Bristol site and contributed to study design, interpretation of results, and drafting of the paper. CAM contributed to the analysis plan, contributed to the interpretation of the results and drafting of the paper. All authors approved the final version of the paper.
-
Funding This work is based on independent research commissioned and funded by the Policy Research Programme in the Department of Health (reference number 0010009). The views expressed are not necessarily those of the department.
-
Competing interests None.
-
Patient consent Obtained.
-
Ethics approval Ethics approval was given by the Dyfed Powys Local Ethics Committee (no.: 05/WMW01/23).
-
Provenance and peer review Not commissioned; externally peer reviewed.