Article Text

Abstract
Objectives To examine relationships between violence, age (0–74 years), and deprivation, and to explore in which communities, age groups, and gender the potential for transmission of violent tendencies between individuals is greatest.
Methods Five year (2004/2005 to 2008/2009) ecological study of emergency admissions resulting from violence (n=170 074) into all English hospitals using trend and logistic regression analyses.
Results Hospital admissions for violence peak as individuals achieve legal adulthood (18 years). Risks of admission increase exponentially with increasing quintile of deprivation of residence, with odds overall being 5.5 times higher in the poorest quintile compared with the richest. The greatest absolute difference in violence admissions by deprivation quintile is seen in males aged 18 (218/100 000, richest; 698/100 000, poorest). However, the highest deprivation rate ratios (quintile 5:1) are seen at ages 0–10 years in both sexes and at all ages after 40 years in males (40–58 years, females). In males aged 17–19 years, violence accounts for 20% of the entire gap between wealthiest and poorest quintiles in all cause emergency hospital admissions.
Conclusions Analyses identify four lifetime periods for violence: up to 10 years (prepubescent), 11–20 years (adolescence), 21–45 years (younger adults), and over 45 years (older adults). While violence is most common in adolescence, its concentration in poorer areas during prepubescence and in younger adulthood (parenting age) suggests that poorer children are exposed to much more aggressive communities. This is likely to contribute to the disproportionate escalation in violence they experience during adolescence. Effective interventions to prevent such escalations are available and need to be implemented particularly in poor communities.
- Violence
- injuries
- Socioeconomic factors
- emergencies
- health services
- public health
- socio economic status
- surveillance
Statistics from Altmetric.com
- Violence
- injuries
- Socioeconomic factors
- emergencies
- health services
- public health
- socio economic status
- surveillance
Introduction
Addressing inequalities in well-being and their social determinants is a key public health objective at international1 and national2 3 levels. Among many causes of morbidity and mortality, interpersonal violence shows some of the strongest inequalities gradients.4 5 Such violence accounts for 1% (600 000) of deaths globally each year6; most occur in poorer countries and communities. Thus, across Africa crude death rates for violence per year are 24.7 per 100 000 population compared with 7.4 per 100 000 in the European region.6 Across Europe, rates are around 10 times higher in low and middle income countries than in high income countries.6 Even within high income countries experiences of violence strongly relate to deprivation. For instance, a study in England found strong associations between indicators of deprivation and both investigation of parents for child maltreatment and registration of children (aged under 6) with child protection services.7 In Canada, individuals requiring emergency medical treatment for violent injuries have been found to reside most commonly in areas of social deprivation (eg, higher social housing, lower household incomes),8 while in the UK, individuals living in deprived areas (particularly young males) have shown significantly increased risks of both hospitalisation for violent injury (England)9 and violent death (Scotland).10 In fact, international reviews consistently identify links between deprivation and increased risks of being both a perpetrator and a victim of many forms of violence.11 12 Here, factors related to deprivation, including a lack of education, unemployment, dysfunctional family environments, delinquent peers, and exposure to violence early in life can create environments where individuals are more likely to regard violence as a solution to stressful situations and a mechanism to achieve respect and resources.11
A growing body of evidence suggests that violence may behave in a contagious fashion; being passed between individuals and across generations.13–16 Thus, in the USA, youths who have experienced abuse in childhood show significantly increased odds of bullying, physical fighting, dating violence, weapon-carrying, self-harm, and suicide attempt in adolescence.13 Among adults, such adverse childhood experiences have been associated with increased risks of high perceived stress, difficulty controlling anger, and perpetrating intimate partner violence.17 Moreover, the same individuals are also at increased risk of indulging in other risk behaviours (eg, substance use) and of both contracting infections (eg, sexually transmitted infections) and developing lifestyle-related diseases (eg, chronic bronchitis or emphysema).17 18 Precise mechanisms connecting exposure to violence in early life with the later development of similar behaviours and poor health remain unclear. However, hypotheses include early exposure to abuse resulting in biological changes in brain development (eg, prefrontal cortex) that make children more vulnerable to aggression in later life.19
Understanding the potential for transmission of violence within communities20 requires analyses not only across those age groups where violent tendencies primarily manifest but also at other ages where individuals may effectively infect children and youths. While a number of studies have examined the sociodemographics of violence,8 10 21 22 most have had insufficient power to examine precise (yearly) age-related changes in violence at population levels over a prolonged period. Here, using five years of national data on emergency hospital admissions for violence (EHAV) across England, we examine how relationships between violence and age vary with deprivation. EHAV do not allow direct examination of transmission of violence across generations. However, we explore changes with age in violence prevalence between the wealthiest and poorest communities in order to understand at what ages potentially contagious elements are disproportionately represented in poorer communities. Finally, we examine the relative contribution violence makes to inequalities in all emergency admissions to hospitals in affluent and deprived communities.
Methods
Data were extracted from the national Hospital Episode Statistics (HES) dataset which records episodes of inpatient care at National Health Service hospitals across England, including private patients. Within this dataset, a unit of care, or finished consultant episode (FCE), equates to the period an individual spends under the care of a single hospital consultant; several of these FCEs may make up a continuous period of inpatient care, or spell. For this study, a pseudo-anonymised identifier was used to count individuals once per year, where their first FCE within a spell was categorised as an emergency rather than planned attendance, and where they were under 75 years of age at the point of admission. This upper age limit was applied as the populations within single year age bands were considered too small above this limit.23
Codes extracted for analysis were: assaults (ICD-10 codes X85–X99, Y00–Y09; ie, all types of assaults including by bodily force, sharp object, blunt object, firearm, chemical, or other means24) and all emergency admissions regardless of cause. An annual count of these data was broken down by age at admission and sex for the years 2004/2005 to 2008/2009. Each 12-month period ran from 1 April–31 March (ie, annual cycle for HES data collection). The total number of records extracted over the five-year period was 170 074 for violence and 13 448 932 for all emergency admissions.
In order to assign individuals with a measure of deprivation, their postcode of residence was mapped to lower super output areas (LSOA; geographical areas (population mean=1500) designed to standardise reporting of small area statistics in England and Wales).9 This allowed linkage with the Index of Multiple Deprivation 2007, a composite measure of deprivation combining economic, social, and housing data,25 also available at LSOA level. Midyear population estimates for 2004–0823 were applied as denominators for the calculations of rates. For each HES year, data were then separated into population quintiles of deprivation, and for each quintile, single year of age rates (for assault and all emergency admissions) were calculated separately for each sex. As all rates were calculated for single-years of age, individual genders, and specific quintiles of deprivation, further standardisation techniques were not required.
Data were initially formatted using Access, with final datasets at LSOA levels transferred to SPSS V.17 for statistical analysis. Deprivation rate ratios were calculated as the ratio of violence rate in the poorest quintile to that in the most affluent; for the purposes of analysing age trends this was then smoothed by applying a five-year rolling average to calculate smoothed deprivation rate ratios (SDRR) by sex for ages 2–72 years. Differences between each deprivation quintile and temporal trends in EHAV were examined using backwards conditional logistic regression. Other statistics used include linear regression to examine separate trends in EHAV rates by age, sex, and deprivation; t tests to compare regression slopes between quintiles of deprivation; and Wilcoxon signed rank tests to compare rates between demographics.
Results
Males
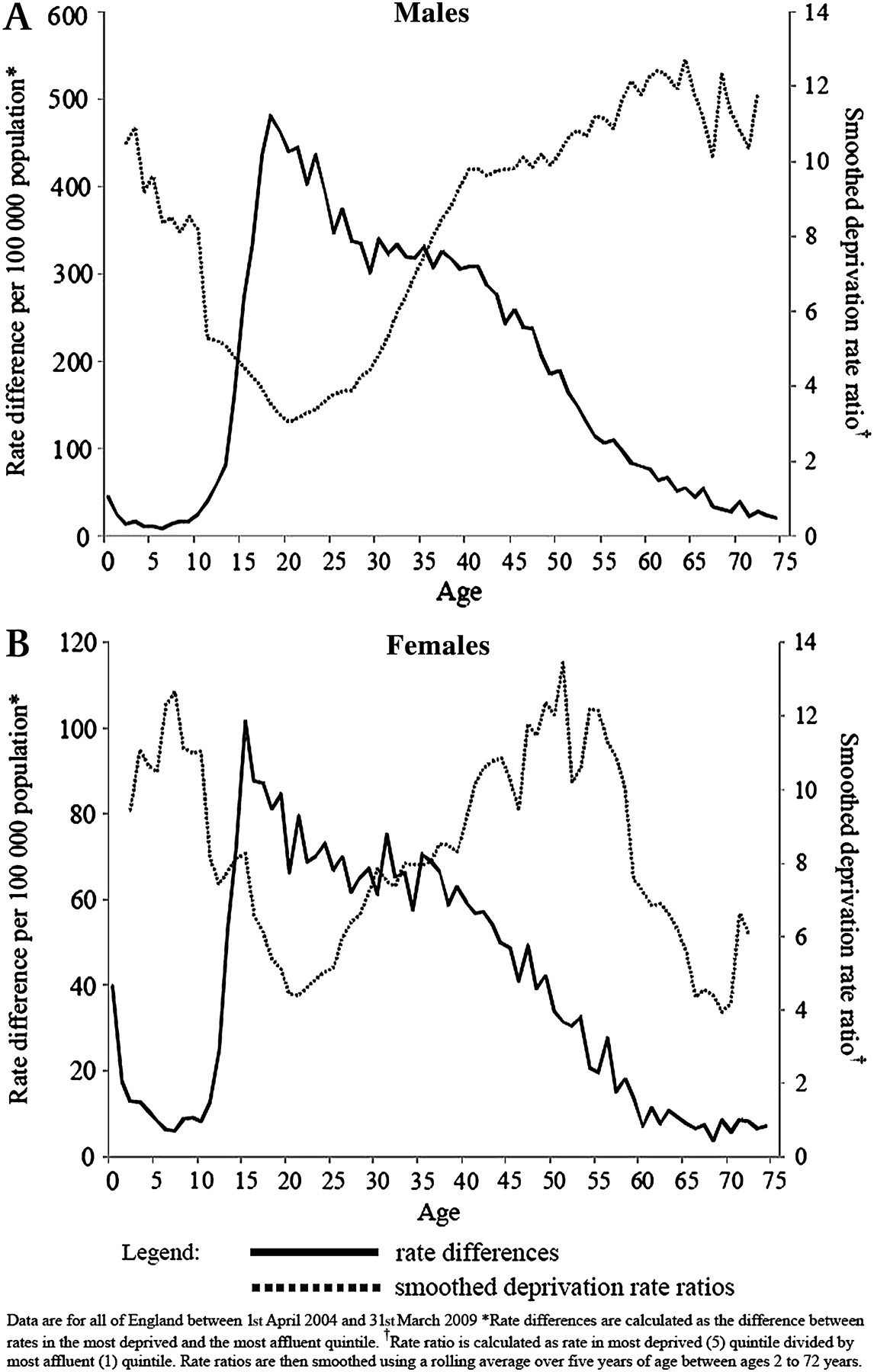
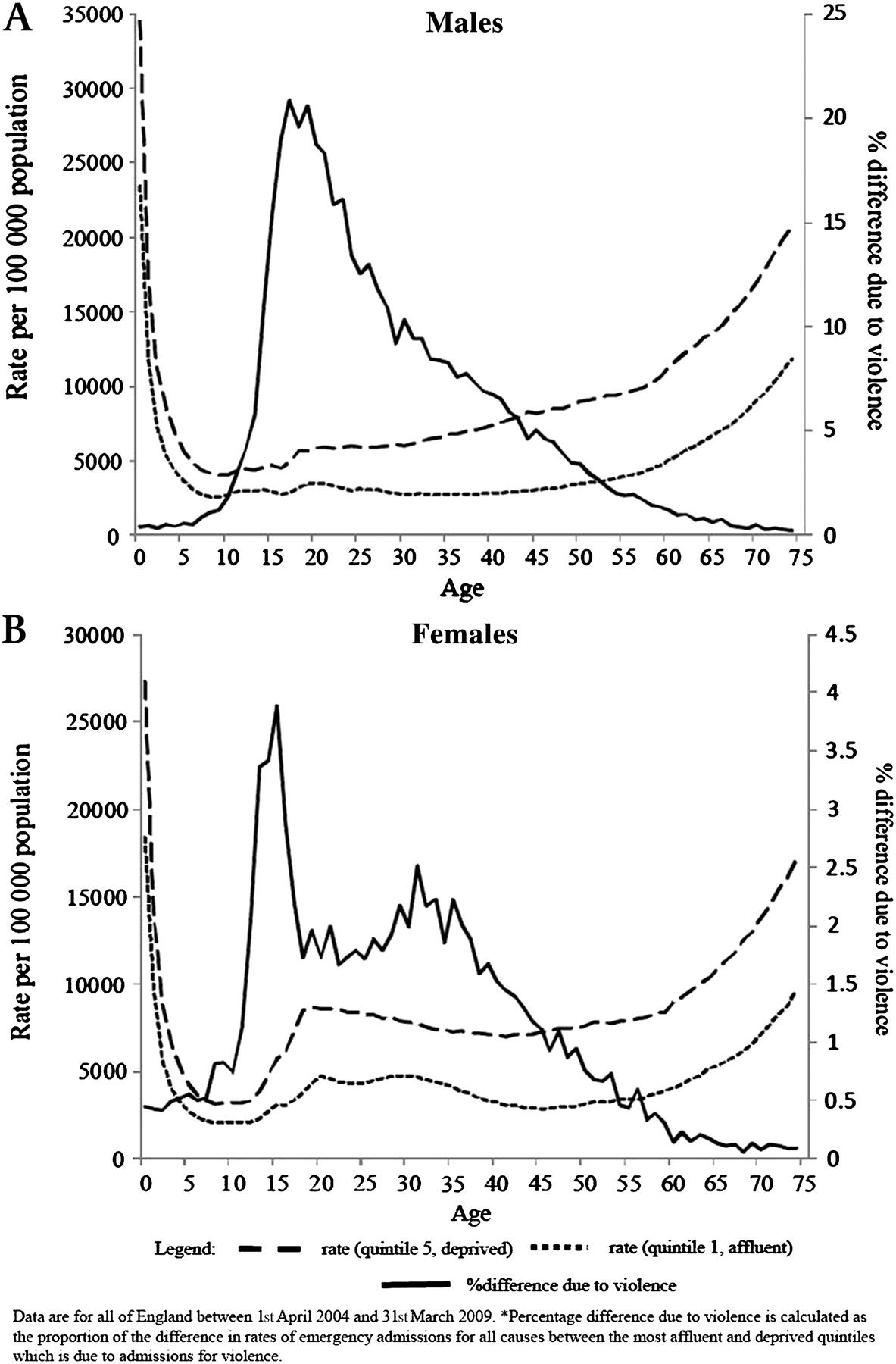
Across all tiers of deprivation, annual rates of EHAV in males rise steeply from the age of 10 years (figure 1A). From 10 to 20 years rates rise from 5 to 245/100 000 (R2=0.920, p<0.001) in the most affluent quintiles, but over the same period rise from 31 to 685/100 000 (R2=0.946, p<0.001) in the poorest quintile. Consequently, with a significantly steeper slope (t=7.787, p<0.001), males living in the most deprived quintile already experience higher levels of EHAV at age 15 than those in the most affluent areas experience as individuals aged 20 (figure 1A). Absolute differences in rates of EHAV between the richest and poorest quintiles of deprivation peak in males at age 18, where the difference in rates is 480/100 000 (218/100 000, richest; 698/100 000, poorest; figure 2A). A sustained fall to 50% of peak value is reached in the most deprived quintile at age 40, 22 years after the peak (figure 1A). The same fall to 50% of peak value is reached in the most affluent quintile only 6 years post-peak at age 26. This difference in rates of decline means that the SDRR is typically between 10 and 12 after age 40 (figure 2A), significantly higher than during ages 11–20 (Z=4.892, p<0.001). The SDRR is also high and consistently above 8 up until after 10 years of age (figure 2A). Rates for all emergency hospital admissions are consistently higher across all ages in the most deprived quintile (compared with the most affluent; Z=7.525, p<0.001; figure 3A). However, the proportion of the difference in rates for all emergency admissions accounted for by violence differs dramatically with age. Thus, under 8 years and above 62 years, violence accounts for less than 1% of the gap. However, at ages 17–19 years it accounts for 20% of the difference in rates for all emergency admissions (figure 3A).

Annual rates of emergency hospital admissions for violence across England by sex, age*, and deprivation: (A) males; (B) females.
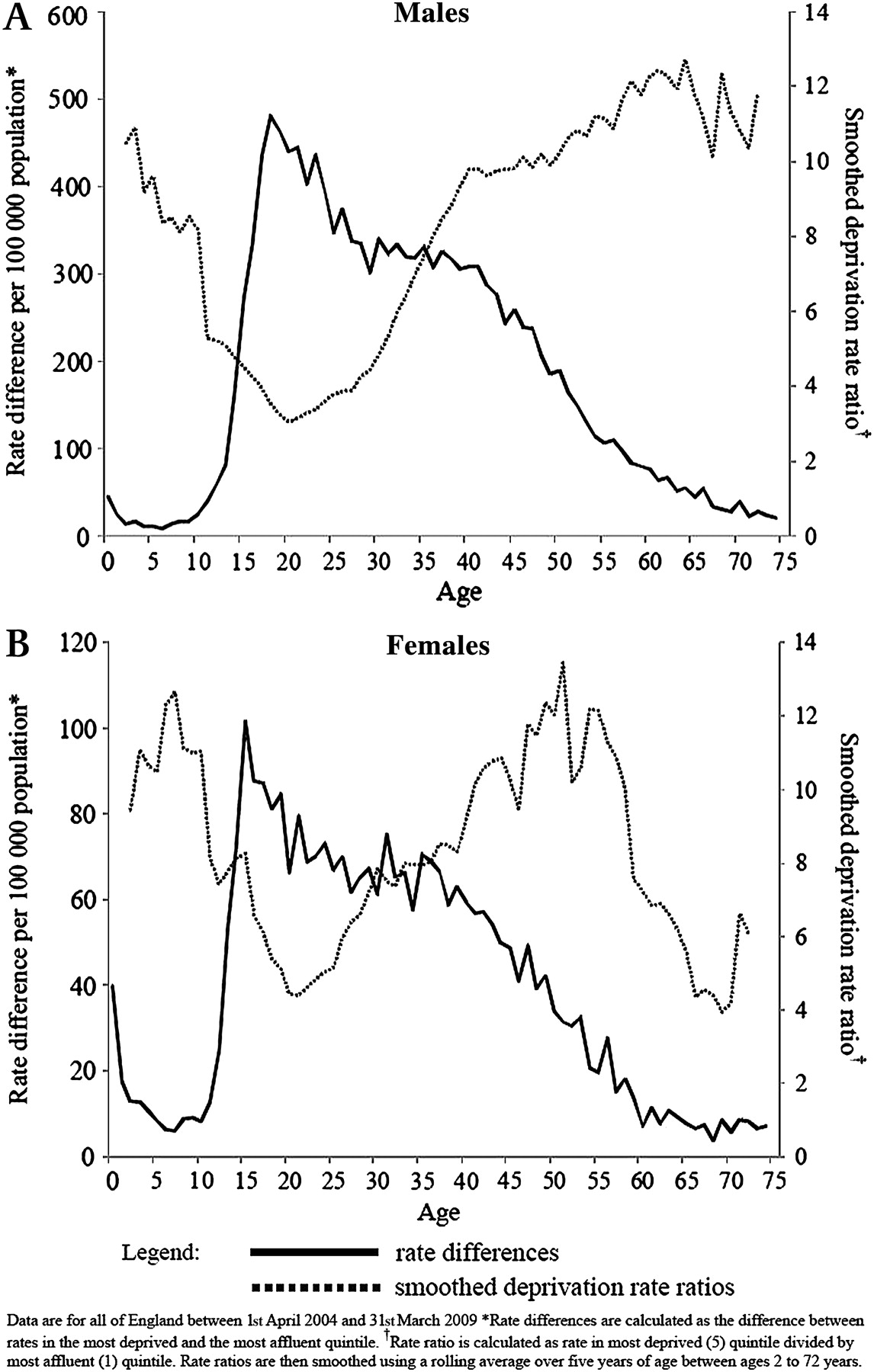
Annual rates differences* and smoothed deprivation rate ratios† for emergency hospital admissions for violence by sex, ages and deprivation: (A) males; (B) females.

Annual rates of emergency hospital admissions for all causes by ages for most affluent and deprived population quintiles and contribution to difference made by violence related admissions*: (A) male; (B) females.
Females
Albeit at a lower prevalence across all ages (Z=7.525; p<0.001), females show similar circa and post-pubertal increases in EHAV, which are higher for all ages in more deprived communities (figure 1B). Thus, increases in admission rates for EHAV between 10 and 20 years are from 2 to 28/100 000 in the most affluent quintile (R2=0.917, p<0.001) and 10 to 94/100 000 in the most deprived quintile (R2=0.722, p<0.001). Again, the slope of increase in the most deprived quintile (cf. the most affluent) is significantly steeper (t=3.560; p<0.005). For females in the most deprived quintile, rates of EHAV peak at age 15 (at 118/100 000), but in the most affluent quintile do not peak until aged 20, and even then only reach 28/100 000. Like males, the decline to 50% of peak value is much slower in the most deprived group (where 50% of peak is reached at 43 years of age) compared with the most affluent one (26 years of age). As a result SDRR rises to above 10 after 40 years of age in women, but unlike in men, falls markedly from age 55. Consistent with males, however, females also have high SDRRs up to the age of 10 (figure 2B). Rates for all emergency hospital admissions for females were consistently higher across all ages in the most deprived quintile (compared with the most affluent; Z=7.525, p<0.001; figure 3B). However, the proportion of the difference in rates accounted for by violence was significantly lower (Z=7.435, p<0.001) in females. Thus, EHAV account for a maximum of only 3.9% of the gap in all emergency admissions (in females aged 15; figure 3B).
Logistic regression
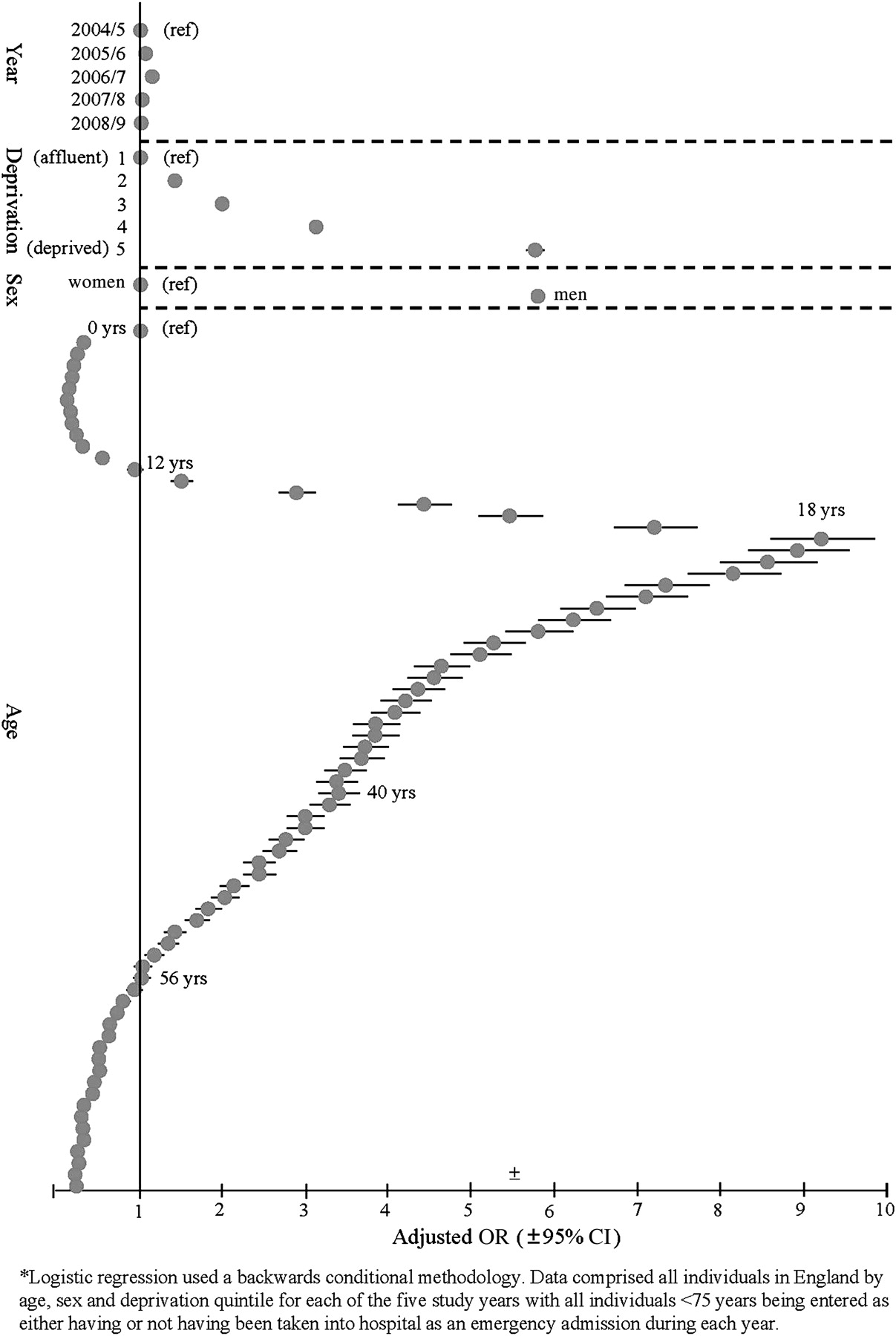
In order to examine the independent contributions of age, sex, and deprivation, and to examine time trends in EHAV, logistic regression analysis was undertaken. Results indicate that increasing quintiles of deprivation show an exponential increase in odds of EHAV (figure 4). Independently, males are 5.42 times more likely to be admitted to hospital due to violence than females. For both sexes combined, EHAV peak at age 18. Levels of EHAV also varied over the five-year study period, with odds of individuals being admitted into hospital due to violence rising by 13% from 2004/2005 to 2006/2007 but then falling again to 2004/2005 levels by 2008/2009 (adjusted OR 1.01±1.02–0.99; figure 4).
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Logistic regression analysis* of temporal trends and demographic risk factors for emergency hospital admissions for violence across England between 1 April 2004 and 31 March 2009.
Discussion
National analyses of age-related trends in emergency hospital admissions for violence show a series of different phases with characteristics that vary with deprivation.
Up to 10 years (prepubescent)
Here, levels of EHAV are relatively low, with the exception of infant admissions (under 1 year of age) where odds of being admitted for violence are over four times higher than for individuals aged 5 years (figure 4). This reflects trends in fatal violence that identify infancy to be a key period of risk for homicide both internationally and in England.26 At all ages in the prepubescent period, males have higher admission rates than females, with harm from violence becoming disproportionately more common in males as they age (figure 1A,B). Of course, hospital admissions account for only a small proportion of violent events; often the more severe. There are an estimated 10 emergency department attendances for every hospital admission for violence,9 and many more people again who are treated in primary care, who self-medicate, or whose injuries are treated or hidden by parents and guardians. However, our data identify the prepubescent period as significantly more violent in poorer areas, with the ratio of admissions for violence in the most deprived to most affluent quintiles being consistently above 8 in both sexes (figure 2A,B). While we could not distinguish whether such violence resulted from conflict with or abuse from parents, peers, siblings, or others, exposure to violence during these formative years not only has a major impact on children's life chances, but is also strongly associated with the development of violent tendencies in adolescence and later life.13 17 18
11–20 years (adolescence)
Absolute differences in rates of admissions to hospital for violence between the wealthiest and poorest communities increase in both males and females, although the level of escalation in rates of admissions for violence is substantially greater in males (figure 1A,B). In females especially, data also suggest that the escalation begins and peaks earlier in the most deprived communities. Thus, females in the most affluent quintile have their highest rates of admission at age 20, as they begin young adulthood. Conversely, those in the poorest quintile have already exceeded this rate by age 12 and their rates peak at age 15 while still in childhood (figure 1B). Again, we cannot distinguish whether this violence is perpetrated by family members, peers, or others. However, for some females this period can be the start of a cycle of victimisation through intimate partner violence, but assaults can also include interpersonal violence between females. Further, with teenage pregnancy also focused in deprived areas,27 some of those involved will be young parents whose children may be exposed to a multitude of risk factors for violence, including having a teenage mother, exposure to violence in childhood, and living in a deprived community.11 Throughout this period of adolescence, SDRRs are lower than the prepubescent period, yet are still consistently above 4 in both males and females. For males, the difference in violence emergency admission rates between poor and rich communities is large enough to account for a fifth of the entire gap in all emergency admissions by age 17 years (figure 3A).
21–45 years (younger adults)
While there are falls in emergency admission rates for violence across all levels of deprivation and in both sexes (figure 1A,B), there are important demographic differences. Falls are relatively slower in the most deprived areas, leading to increasing SDRRs (figure 2A,B). Critically, this period also includes the vast majority of child births to adults and parenting of children during their preadolescent years. While again it was not possible here to examine the types (eg, males to females or males to males) or locations (public or private space) of violence that younger adults were experiencing, it is likely that such violence will contribute to more belligerent childhood environments. For instance, it is estimated that between 240 000 and 963 000 children in the UK alone are exposed to domestic violence.28 Exposure to such adult violence in childhood again contributes to the risks of children developing aggressive tendencies.13 17
Over 45 years (older adults)
In both males and females, rates of emergency hospital admissions for violence continue to fall after 45 years of age (figures 1A,B and 4). The disproportionate reductions in rates seen in the most affluent areas for younger adults mean that SDRRs in males remain above 9 throughout the entire period. However, in females after age 55, SDRRs fall as rates for EHAV in the poorest communities stabilise while there are slight increases in levels in those in the most affluent areas (figures 1B and 2B). However, such figures should be treated with caution given the low numerators used in their calculation. Moreover elder abuse in particular, is often a poorly recorded and understudied area of violence resulting in many cases being missed.29
Prevention
In poorer communities, the combination of more involvement in violence before puberty and a greater chance of exposure to younger adult violence during the same period are likely to contribute to the large spike in violence associated with a deprived adolescence (figure 1A,B). Programmes (eg, Nurse Family Partnership,30 31 Triple P Positive Parenting Programme32) have already been developed to help support parents as well as infants and young children through the critical early stages of child development. Such programmes now have an established evidence base which identifies effective reductions in risk of child maltreatment and involvement in violence as children progress through adolescence and into adulthood; overall cost savings associated with programme implementation are also identified.31–34 Their targeted application in areas of higher deprivation should be a priority. Historically, however, responses to violence in England have typically been based on criminal justice data detailing where assaults occur35 36 rather than the residential communities in which violent individuals live. Such intelligence favours criminal justice interventions aimed at violent environments (eg, nightlife settings) rather than early life prevention interventions targeted at communities where violent tendencies develop.
The greatest single increase in violence is seen as individuals move into legal adulthood (ie, from 17 to 18 years of age; see figure 4). This period is strongly associated with increasing alcohol consumption,37 38 and results presented here at the least raise the issue of whether youths are suitably prepared for the unlimited access to alcohol available when individuals reach 18 years of age. Measures to control the availability of alcohol can reduce violence,39 with strategies such as increased alcohol pricing likely to have particular impacts on alcohol use and associated violence in youth.40
Hospital admissions data can play a central role in the continued measurement of the impact of violence on health and assessment of the effectiveness of interventions at policy and practice levels. However, while HES captures some of the most damaging violent events, others, often resulting in no or only minor injuries, are dealt with by emergency departments, general practitioners, or through self-medication.41 At the other extreme HES do not include many assault-related fatalities. Over the study period, across England there were 3445 recorded homicides.42 Such small numbers are unlikely to affect reported HES trends and evidence suggests that the demographic distribution of homicides is consistent with those for EHAV reported here.10 Moreover, data rely on accurate coding within acute hospital settings. In recent years, the broad utilisation of the HES data system has led to improvements in data quality, but coding still relies on clinicians initially exploring, then correctly identifying, violence as a cause of admission.43 Clinician training in screening for issues such as child and elder abuse and domestic violence may increase the ability of staff in some areas to identify violence as a cause of admission and improve referral for appropriate support as well as triggering protection services to reduce further assaults.44 The extent to which such innovations have been employed across different hospitals in England could not be measured in this study. Finally, although we have examined the changes in risk of EHAV with age, we have not tracked individuals as they age but used a series of cross-sectional datasets to describe age and sex related trends in risk by deprivation. The use of an ecological measure of deprivation assumes that the deprivation status of individuals requiring EHAV conforms broadly with that of the area (LSOA) within which they live.
Conclusions
The last decade in particular has seen an increasing recognition that criminal justice punishments alone are not effective at reducing violence. At the same time a wide range of primary prevention measures, largely aimed at improving early childhood experiences and reducing early exposure to violence, have been identified as both effective and economic ways to reduce the risks of children developing into violent adolescents and adults.11 45 Across England, recent policy analyses46 have identified the need for a wide range of specialist and generalist early life services, including general practitioners, midwives, health visitors, and hospitals and nursery provision, to provide more accessible and better integrated services to those in deprived areas. Such measures are not only likely to result in better educational and health outcomes but should also reduce levels of violence as individuals later pass through puberty and adulthood. Analyses presented here identify those community groups who would most benefit from such interventions and the time in their members' life course by which such interventions have to have been implemented in order to prevent escalations in violence (figure 1A,B). The potential savings associated with employing such interventions are considerable. Reducing the rates of EHAV in the most deprived group to that of just the middle quintile of deprivation would have resulted in 48 381 fewer individuals (aged <75 years) having been admitted into hospital in England as emergencies over this five-year period (28% of all EHAVs). The reductions in attendance at emergency departments would be expected to be an order of magnitude higher. The average economic cost of a violent crime in the UK has been estimated at over £10 000 when health, criminal justice, and societal costs are taken into account, rising to £1.4 million for a homicide.47
The benefits of effectively introducing programmes that immunise young children against developing violent tendencies as they age or otherwise reduce levels of violence may be even more broadly felt. The implementation of many community public health programmes relies on individuals having confidence in their safety. Efforts to encourage outdoor exercise in children, for instance, may be resisted by parents with concerns for their children's safety in unsupervised public spaces (eg, parks). Equally for adults, engagement in initiatives to improve local communities may depend on community members expecting a benefit from interacting with neighbours rather than a need to protect themselves from each other. Even health and social care professional engagement may be undermined when such individuals feel unsafe visiting certain areas. In 2010, England began a new policy direction to create a Big Society with a network of community professional organisers aimed at bringing local individuals together in order to solve their own problems.48 49 The success of such measures will depend in no small part on whether individuals view their local community as a potential source of support or a threat to their family's security and well-being.
What is already known on this subject
Individuals' likelihood of experiencing violence is strongly associated with deprivation.
Children who experience more aggressive or abusive childhoods are more likely to become perpetrators and/or victims of violence in later life.
As well as often major and long term detrimental effects on the health of victims, violence can adversely affect economic prospects, community cohesion, and the local delivery of health and other services.
What this study adds
Rates of emergency hospital admissions for violence in England increase at an accelerating rate as individuals pass through teenage years and peak at legal age of adulthood (18 years), when absolute differences between rates in richest and poorest areas are greatest.
Although most hospital admissions for violence occur during adolescence, the rate ratios (poorest to richest areas) are higher in children (0–10 years) when rates are typically more than eight times higher in poorer areas. Rate ratios fall during adolescence and then rise again as individuals pass through young adulthood (21–45 years).
The distribution of emergency hospital admission suggests that childhood for the poorest in England takes place in substantially more violent communities, and this may contribute to the rapid escalation in violence such children pass through during adolescent years.
Acknowledgments
This work would not have been possible without the support of staff in the North West Public Health Observatory. We are grateful to Jenny Downing who helped with the conversion and formatting of the hospital episode data. We are also indebted to Dr Ian Jarman and Terrance Etchells whose statistical input helped shape the analytical approaches adopted in this paper. Finally, we thank Francesco Mitis and two anonymous reviewers whose constructive comments helped improve an earlier version of this manuscript.
References
Footnotes
Funding This study was conducted exclusively through the support of the Faculty of Health and Applied Social Sciences at Liverpool John Moores University.
Competing interests None.
Provenance and peer review Not commissioned; externally peer reviewed.