Article Text

Abstract
Background Pools with lifeguards are often perceived to represent a safe environment for swimming.
Objectives To examine how often fatalities occurred in pools with lifeguards and what factors were common in these incidents.
Design Case series.
Setting USA.
Subjects A case was defined as a death in a swimming pool with at least one lifeguard that occurred in the USA from 2000 to 2008. Potential cases were identified from media accounts using Lexis-Nexis and ProQuest databases. Supplemental information was obtained through internet based searches and review of death certificates.
Results A total of 140 deaths from 37 states were identified. Of decedents, 109 (78%) were children and 93 (66%) were males. African Americans accounted for 44% of deaths among those of known race. 104 (74%) fatalities occurred during May through August; 85 (61%) deaths occurred in outdoor pools. Sites for fatal incidents included 53 (38%) municipal pools, 21 (15%) community organisations, and 20 (14%) schools. The median swimmer to lifeguard ratio was 13:1. Decedents were initially identified in the pool twice as often by non-lifeguards (eg, other swimmers or bystanders) as by lifeguards.
Conclusions Deaths in pools with lifeguards are uncommon, but do occur. Groups most affected include children, males, and African Americans. While lifeguards provide an important layer of protection at swimming pools, they alone cannot prevent all drownings. Additional safety measures are needed.
- Swimming pools
- lifeguard
- death
- drowning
- injuries
- public health
- recreation
Statistics from Altmetric.com
Introduction
Drowning is a leading cause of death from unintentional injuries in the USA. For children 1–14 years of age, drowning is second only to motor vehicle crashes as a cause of injury mortality.1 Besides children, groups considered at greatest risk of drowning include males, minorities, and those with health conditions such as epilepsy.2–5
Adults may incorrectly perceive the risks involved with swimming for both themselves and their children.6–8 Lack of adequate supervision is often cited as a risk factor for paediatric drowning.6 While lifeguards are generally considered to be effective in enhancing safety, their ability to safeguard swimmers has limitations.9–14
Pools have certain safety advantages over natural bodies of water as they represent a controlled environment with regards to water clarity, depth, and surface area. With certain exceptions, pools also lack the currents and obstacles found in rivers and oceans.
Pools with lifeguards are often perceived to represent a safe environment for swimming. However, drownings in pools with lifeguards do occur. We examined how often fatalities occurred in pools with lifeguards and what factors were common in these incidents.
Methods
Case definition
A case was defined as a death in a swimming pool with at least one lifeguard on duty that occurred in the USA from 2000 to 2008.
Case finding
Potential cases were identified by doing keyword searches for ‘drowning’, ‘pool’, and ‘lifeguard’ using two electronic databases of media reports (LexisNexis and ProQuest). These terms were self defined by media sources; however, incidents involving non-standard usage of these terms were excluded (ie, ‘drownings’ that were not fatal, ‘pools’ that were naturally occurring bodies of water, and ‘lifeguards’ that were swimming instructors who were not responsible for the safety of all pool attendees). A total of 1323 documents were retrieved using LexisNexis; 386 documents were retrieved using ProQuest. All documents were reviewed by one investigator (ARP) to determine which involved deaths meeting the case definition. Case finding was enhanced by conducting internet based searches for additional fatalities.
Data collection
Information on each case was abstracted from the media accounts obtained during case finding activities. Supplemental information such as ethnicity and country of birth was obtained through death certificates and internet based searches. Data from death certificates were obtained from the Consumer Product Safety Commission and state health departments. For certain variables (eg, whether a pool was located indoors or outdoors), missing data were obtained by telephone and email requests.
Data analysis
Variables with missing data are noted by providing the sample size available for analysis. Population figures were obtained from the US Census for 2004, the mid year for the study period.
Human subjects review
The study was reviewed by the Centers for Disease Control and Prevention and determined not to be research involving human subjects, as all cases were deceased and no follow-up occurred with family members or persons involved in the fatal incidents.
Results
Study subjects
A total of 140 fatalities were identified (table 1). Of decedents, 109 (78%) were <18 years of age. Ninety-three (66%) decedents were males. The percentage of deaths among African Americans was higher than expected given the population distribution of the USA. Mortality by ethnicity and country of birth appeared consistent with the country's population distribution.
Characteristics of fatalities in swimming pools with lifeguards—USA, 2000–2008 (n=140)
Selected cases
The following are three examples of cases.
▶Case 1. A 14-year-old female went to an outdoor public pool by herself in July 2002. She reportedly did not know how to swim. At approximately 15:30, a young swimmer alerted lifeguards that there was a body at the bottom of the deep end in the pool. Approximately 30 swimmers were in the pool at the time of the incident. The water was cloudy making the bottom of the pool difficult to see. The object at the bottom of the pool was thought initially to be a drain cover. A lifeguard put on goggles, dove into the deep end, and was able to retrieve the girl on the second attempt. Efforts to revive her were unsuccessful. She was pronounced dead at a local hospital. Police estimated that she may have been at the bottom of the pool anywhere from several minutes to a half hour. There were two teenage lifeguards on duty at the time of the incident. They were together in a structure approximately 30–40 feet from the pool's edge. One of the two lifeguard chairs overlooking the pool was broken.
▶Case 2. A 2-year-old male visited an outdoor water park in June 2001 with his parents and four siblings. Shortly after arriving, he and his three older siblings, ages 7, 8, and 10 years, entered a pool which went from several inches to 6 feet (1.83 m) of water. His father was caring for a 1-year-old child. His mother was in a changing room. At 17:15 a child in the pool alerted lifeguards that the boy was floating in 3–4 feet (0.9–1.2 m) of water. Attempts to resuscitate him were unsuccessful. He was pronounced dead about an hour later at a local hospital. The water park consisted of three pools. Fifty lifeguards and >2000 people were present at the time of the incident.
▶Case 3. A 26-year-old male was preparing for military induction; he wanted to join the Navy's Special Forces. He was found unresponsive at approximately 14:45 while at an indoor college pool in December 2001. He was declared dead at a local hospital at 15:19. Reportedly he used the pool to swim laps and practise breath-holding exercises. One lifeguard was on duty at the time of the incident.
Time and place of incidents
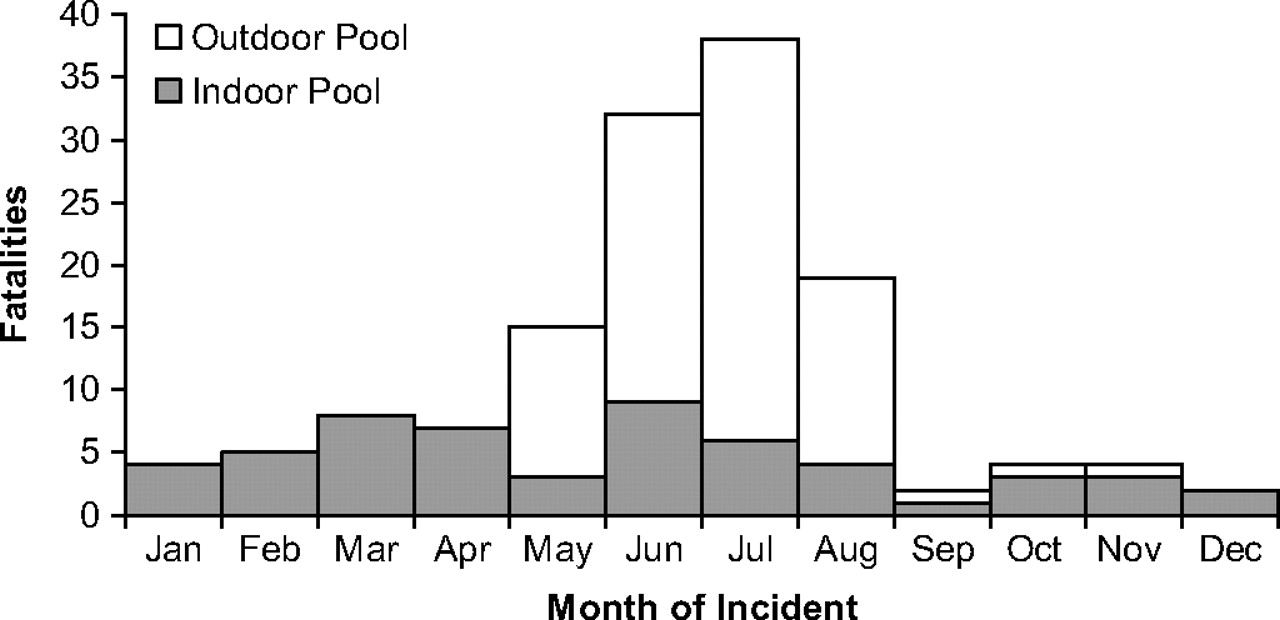
Deaths were identified in 37 states. States with the most fatalities were Pennsylvania (14 deaths); California, Maryland, and Ohio (nine deaths each); Michigan and New York (eight each); and Florida and Texas (seven each). One hundred and four (74%) fatalities occurred during May through August (figure 1). Eighty-five (61%) deaths were in outdoor pools. Deaths in outdoor pools accounted for most of the seasonal variation in mortality; 82 (59%) deaths occurred in outdoor pools from May to August. There was no substantial variation in deaths by day of the week; the most deaths occurred on Wednesdays (26 deaths) and the fewest deaths occurred on Sundays (13 deaths). For the deaths for which the time of the submersion incident was known (n=125), 103 (82%) occurred from 12:00 to 19:59. Sites for fatal incidents included 53 (38%) municipal pools, 21 (15%) community organisations, 20 (14%) schools, 17 (12%) clubs, nine (6%) apartment complexes, seven (5%) summer camps, seven (5%) water parks, and six (4%) other sites.
{kind=link}
Fatalities in swimming pools with lifeguards by month of incident—USA, 2000–2008.
Underlying and contributing causes of death
For fatalities in which the official cause of death was known (n=122), all but three were reported as due to drowning. The exceptions were the deaths of two males who were 73 and 80 years of age, which were attributed to heart disease, and the death of a 13-year-old male from an undetermined cause. Contributing factors that may have played a role in other incidents included disabilities (eight decedents: one with a physical disability, three with mental disabilities, and four with both physical and mental disabilities), heart disease (seven decedents), a history of seizures (seven decedents), and alcohol intoxication (one decedent). A total of 106 (75%) individuals died on the same day as the submersion incident; 16 (11%) died the following day. The remaining 18 individuals died 2–27 days after the submersion injury. For individuals for whom information was available (n=111), 99 (89%) underwent autopsy. Two decedents had evidence of external trauma—a 19-year-old male with a blunt force injury of the neck and an 8-year-old female with a bruise on the scalp.
Eight decedents, all males, were reported to be practising breath holding exercises before their deaths. All but one were 14–26 years of age. Two individuals, a 4-year-old and a 36-year-old, died in wave pools. Two decedents were lifeguards who drowned while swimming recreationally in guarded pools. Only one (1%) decedent, a 3-year-old female, was wearing a personal flotation device. She drowned after becoming trapped beneath an inflatable raft that she was sharing with her sister in a 50 m outdoor pool with 100 swimmers and 11 lifeguards.
Lifeguards and other swimmers
For incidents in which data were available (n=106), the median number of lifeguards on duty at the time of the fatal incidents was 2 (range 1–50). For 57 incidents, the number of people swimming at the time of the submersion incident was known (median 30; range 1–2000). For 51 incidents, the swimmer to lifeguard ratio was available (median 13:1; range 1:2 to 75:1). The first person to identify the submersion victim in the water was a lifeguard in 31 (22%) incidents and a non-lifeguard (eg, another swimmer or a bystander on the pool deck) in 61 (44%) incidents. The person who initially identified the submersion victim was unknown in 48 (34%) incidents.
Discussion
Groups at risk for drowning
Drownings are often described as quick and silent although the public perception may be otherwise.15 Risk groups for fatalities in swimming pools with lifeguards appeared to be similar to those identified in previous studies of drowning. Children, males, and African Americans have significantly higher mortality rates from drowning than other groups.1–3 16 Lapses in parental supervision are the most commonly cited contributing factor in childhood drownings.17 18 Higher mortality rates in males have been attributed to greater exposure to aquatic environments, more alcohol use, and a greater tendency towards risk taking.3 Racial differences in drowning mortality are most often attributed to swimming ability.2 15 19–21 In one survey, 62% of African American adults reported limited swimming ability compared to 32% of white adults.21 Swimming ability may be particularly relevant in pool drownings where basic survival skills should allow most individuals to reach the side of the pool or float briefly while seeking assistance.
Indoor versus outdoor pools
Over 60% of incidents occurred outdoors; this finding may reflect the fact that more swimmers use outdoor pools than indoor pools especially during the summer months. Unfortunately there were no exposure or participation data available to address this question. Other possible explanations are that seasonal pools may employ less experienced staff, attract more individuals with limited swimming ability, or have environmental factors (eg, overcrowding, glare, heat) which inhibit a lifeguard's ability to identify and respond to a patron having difficulty.22
Lifeguards
Lifeguards are widely accepted as being effective in enhancing water safety during recreational activities.9 The United States Lifesaving Association estimates that the chance that a person will drown while attending a beach protected by US Lifesaving Association affiliated lifeguards is 1 in 18 million.23 However, there is concern that the presence of lifeguards may result in parents being less observant of their children.9 24 In one survey, 20% of parents believed that the lifeguard was the main person responsible for supervising their children in the water.15 As noted in this study, individuals such as other swimmers and pool bystanders were twice as likely to initially identify submersion victims as were lifeguards. Realising that no single strategy can prevent all pool drownings, lifeguards should be considered as one layer of protection for preventing and responding to submersion incidents.25 Programmes have been developed to educate parents about the need to supervise their children in pools regardless of the presence of lifeguards.26 27
Strengths and weaknesses of this study
The strength of this study was that it was able to examine fatalities over a 9 year period in the USA using two large databases of media reports. Extensive efforts were made to collect additional information through death certificates and internet based searches. To our knowledge, this is the first attempt to study drownings in pools with lifeguards.
Our results represent an underestimate of the true number of fatalities in pools with lifeguards as not all drownings are reported by the media.28–31 In Washington state, 514 (52%) of 983 drownings were reported in newspapers between 1993 and 1998.28 Reporting was better for individuals <20 years of age (71%) than for older individuals (47%).28 Newspapers reported on 42 (72%) of 58 drownings involving individuals <19 years of age in North Carolina in 1988–1989.29 In our study, case finding was likely limited for fatalities that occurred remotely from the time of the submersion injury. Fatalities that occur soon after a submersion appear more likely to attract media attention.
This study was subject to at least three other limitations. First, reliable information on the swimming ability of decedents was not available in most cases. Second, specific information on lifeguards (eg, location in relation to decedents, years of experience, certification) and swimming pools (eg, depth of pool, clarity of water) was often not reported. Third, we did not attempt to identify non-fatal incidents. Focusing only on fatalities underestimates the public health burden of submersion injuries. Among children <15 years of age, it is estimated that for every death there are two non-fatal submersion events treated and released from emergency departments and two more that require hospitalisation.16 Focusing on fatalities also underestimates the protective value of lifeguards as individuals who survived because of lifeguard response are excluded from consideration.
Conclusions
Deaths from drownings in pools with lifeguards are uncommon, but do occur. Based on studies of drowning prevention in general, there are a variety of approaches that might prevent fatalities in swimming pools with lifeguards.
Lifeguards need to be properly trained and supervised; specific training can improve lifesaving skills.32–34 Children <5 years of age should be no more than an arm's reach from a supervising adult (ie, ‘touch supervision’).35 Parental supervision is also needed for older children. Individuals with disabilities or a history of seizures should be monitored closely.36 Whenever possible, all pool users regardless of age should have another person (in or out of the pool) identified to watch and assist them if needed (ie, swim with a buddy).
A policy statement from the American Academy of Pediatrics encourages parents to teach children to swim after their fourth birthday.35 As the majority of deaths in this study was in children 5–14 years of age, this age group should be encouraged to participate in swimming lessons to improve their ability to remain safe in the water. The role of swimming instruction in preventing drowning in younger children has been controversial, but recent research suggests that providing swimming lessons to children 1–4 years of age may be protective.37–39
Additional studies are needed to assess the risk of drowning in pools with and without lifeguards. Such studies should control for aquatic exposure among different population groups.
What is already known on the subject
Drowning is a leading cause of death from unintentional injury.
Groups most affected include children, males, and African Americans.
Pools with lifeguards are often perceived to represent a safe environment for swimming.
What this study adds
Deaths from drownings in pools with lifeguards are uncommon, but do occur.
Groups most affected appear similar to those for drowning in general.
Lifeguards provide an important layer of protection, but alone cannot insure drowning prevention.
References
Footnotes
Disclaimer: The findings and conclusions in this report are those of the authors and do not necessarily represent the official position of the Centers for Disease Control and Prevention.
Funding This work was done by federal employees as part of their normal work activities. There were no external sources of funding for this study. The findings in this report are based, in part, on contributions by Kenneth Ascher, Christy Cechman, Gerald Dworkin and Francesco Pia.
Competing interests None.
Provenance and peer review Not commissioned; externally peer reviewed.