Article Text

Abstract
Objective To determine the mortality burden associated with unintentional injuries among children younger than 5 years of age in India.
Methods The Registrar General of India conducted verbal autopsy for all deaths occurring in 2001–2003 in a nationally representative sample of over 1.1 million homes. These verbal autopsy reports were coded by two of 130 trained physicians, who independently assigned an ICD-10 code to each death. Discrepancies were resolved through reconciliation and, if necessary, adjudication. The probability of death during the first 5 years of life (per 100 000 live births) was estimated from the 2005 United Nations' population and death estimates for India, to which the proportions of deaths from the mortality study were applied.
Results Unintentional injuries were the sixth leading cause of death among children under 5 years of age. In 2005, unintentional injuries led to 82 000 deaths (99% CI 71 000 to 88 000) among children under 5 years of age, a mortality rate per 100 000 live births (MR) of 302 (99% CI 262 to 323). Mortality was higher in rural areas (MR=339, 99% CI 282 to 351), mostly due to more drowning deaths, than in urban areas (MR=173, 99% CI 120 to 237), where falls were the leading cause of child injury mortality.
Conclusion Unintentional injuries, specifically drowning and falls, lead to substantial mortality in children younger than 5 years of age in India. There is a need for continued monitoring of the injury burden and investigation of risk factors for evidence-based effective injury prevention programmes.
- Child
- developing nations
- public health
- surveillance
Statistics from Altmetric.com
Introduction
It is estimated that each year unintentional injuries cause 279 000 deaths in children younger than 5 years of age worldwide.1 Although childhood injury mortality has declined by 50% in high-income countries, indirect studies suggest that it may be increasing in low- and middle-income countries.2 3 Among children younger than 5 years, India alone accounts for one-fifth of the global deaths.4 Children younger than 5 years of age constitute 11% of India's population,5 but over 20% of all deaths.6
Globally, substantial work has been performed to identify possible measures for injury prevention in children,7 but these programmes remain greatly underutilised in low- and middle-income countries, potentially because of the lack of direct estimates of the burden of injury deaths and absence of mechanisms for injury prevention and control.8 As major investments have been made, and continue, to prevent childhood deaths by reducing incidence of infectious conditions, ensuring better nutrition and promoting safe motherhood,4 avoidable death due to injury has received substantially less attention in countries such as India, where death registration systems are usually limited or non-existent.9
The National Crime Records Bureau of India publishes statistical reports on injuries based on police records,10 but these may suffer from gross under-reporting of injury events.11–13 Other potential sources of injury mortality data are the Registrar General of India (RGI), namely the Survey of Causes of Death (SCD, 1982–1999), for rural areas14 and the ongoing Medical Certification of Cause of Death (MCCD) for urban areas,15 which are not nationally representative and thus cannot be used for estimating injury mortality in India.16 Estimates from the few community studies17–19 and a literature review20 indicate that overall under-5 injury mortality in India ranges from 34 to 147/100 000 population.
Here, we provide the first ever direct estimates of unintentional injury mortality among children younger than 5 years in India from a large ongoing nationally representative mortality study.
Methods
In the absence of reliable data for cause-specific mortality in India, the RGI has introduced an enhanced form of verbal autopsy, called Routine, Reliable, Representative, Re-sampled Household Investigation of Mortality with Medical Evaluation (RHIME), into its nationally representative Sample Registration System (SRS).6 This survey is part of the ongoing Million Death Study (MDS), which seeks to assign causes to all deaths in the SRS from 2001 to 2013. Details of the MDS design, methods, quality-control checks, validation and preliminary results have been previously published.6 21–25
Study setting
The SRS covers about 6.3 million people in over 1.1 million homes and monitors all vital events. This sample is based on the 1991 census, in which India was divided into nearly one million small areas, with ∼1000 inhabitants in each. In 1993 the RGI randomly selected 6671 of these areas for a representative sample of the population at each rural/urban stratum for major states. For each household in the sampling frame, household characteristics were recorded and subsequent births and deaths were enumerated twice a year.5
Data collection for the MDS
Since 2001, verbal autopsy interviews have been conducted for all SRS population deaths. These interviews were conducted by one of the 800 trained non-medical field workers who periodically visited the sampled households to record vital events. These workers are full-time employees of the RGI and have knowledge of the local languages. The respondents were family members or a person close to the deceased, preferably someone who had spent time with the deceased during their illness and were aware of the circumstances surrounding the death.
Verbal autopsy instrument
Verbal autopsy interviews used specific questionnaires for neonatal deaths (0–28 days) and child deaths (29 days to 14 years) with a combined open/closed format. A closed question was asked regarding injury history and its mechanism. The question asked was ‘Did s/he die from an injury or accident?’ If the answer was ‘yes’, the kind of injury or accident was enquired about, and the response options were: (1) road traffic crash; (2) fall; (3) fall of an object (on to the person); (4) burns; (5) drowning; (6) poisoning; (7) bite/sting; (8) natural disaster; (9) homicide/assault; (10) unknown. These questions were followed by an open narrative of the events preceding death in the local language.
Assignment of cause of death
Field reports were scanned and sent to two of the 130 trained physicians, who independently assigned codes for the underlying cause of death from chapter XX of the International Classification of Disease, 10th Revision (ICD-10). The codes were assigned on the basis of a review of the written narrative and objective questions, using structured guidelines (available online).26 In the case of disagreement between the two physicians about the assigned three-character ICD code, each was asked, anonymously, to reconsider. Persistent differences were adjudicated by a third senior physician. In the case of sub-chapter disagreement for injury deaths, if the codes were within the same block, the more specific of the two codes was chosen.
Calculation of cause-specific mortality
Proportional cause-specific mortality was derived from the sample of deaths captured by the MDS during 2001–2003. These proportions were weighted by the inverse probability of household selection within rural and urban sub-divisions of each state to account for the SRS sampling design.27 The proportion of deaths from each cause was used to estimate the number of deaths by cause for the year 2005 in India. The year 2005 was selected for estimation because of availability of the most accurate and stable population denominator estimates. Live births and death estimates by sex and rural/urban area for children younger than 1 year, children aged 1–4 years, and for all children younger than 5 years of age were proportionally corrected to match the UN Population Division estimates for 2005.28 The underlying assumption is that there were no changes in proportion of cause-specific deaths in the population from 2001–2003 to 2005.24 All death rates are presented per 100 000 live births. Details of the analysis are available in an online appendix. The estimates of the proportion of deaths due to unintentional injuries for each group excluded cases where age was missing (n=95 or 0.4%). CIs (99%) around the cause-specific proportions and mortality were based on the number of sample deaths in the mortality survey, and calculated using the variance estimated by Taylor linearisation.29 All analyses used Stata V.10.1. Regional comparisons within the country were made for six major regions - North, South, West, Central, Northeast, and East6 - and a division of states with historically higher child mortality, poverty levels, and lower life expectancy.30 These states (Bihar, Jharkhand, Madhya Pradesh, Chhattisgarh, Orissa, Rajasthan, Uttar Pradesh, Uttarakhand) are called the Empowered Action Group states to which Assam has been added (EAG&A).
Results
In the SRS mortality survey, 24 841 deaths were reported in children younger than 5 years of age in 2001–2003. Of these cases, 93% (23 152) had complete information on age and sex and were coded by two physicians. Intent of injury could not be determined for seven deaths. A total of 777 unintentional injury deaths were identified among under-5 children based on chapter XX (External causes of morbidity and mortality) ICD-10 codes V01–X59, Y40–Y86, Y88, and Y89.
Unintentional injuries accounted for 3% (777/23 152) of all deaths in children younger than 5 years. Of all the unintentional injury deaths in the study population, 10% (777/8023) occurred in children younger than 5 years of age. Unintentional injury deaths in infants were 1% (186/16 207) and in children aged 1–4 years were 9% (591/6944) of all causes of mortality. Only 12% (95/777) of all unintentional injury deaths occurred in a health facility (table 1).
Unintentional injury deaths in children aged 0–4 years in the present study and estimated national totals by sex and place of residence
Application of these proportions to national totals of deaths leads to an estimate of 82 000 deaths due to unintentional injuries of children younger than 5 years in 2005. This corresponds to a mortality of 302 per 100 000 live births (99% CI 262 to 323, table 1). Death rates were similar in boys (301, 99% CI 252 to 337) and girls (303, 99% CI 243 to 324). Mortality was higher in infant (<1 year of age) girls (81) than boys (60), although in this small sample size the difference was not significant (p=0.12). Mortality was higher in rural areas (339, 99% CI 282 to 350) than urban areas (173, 99% CI 120 to 237).
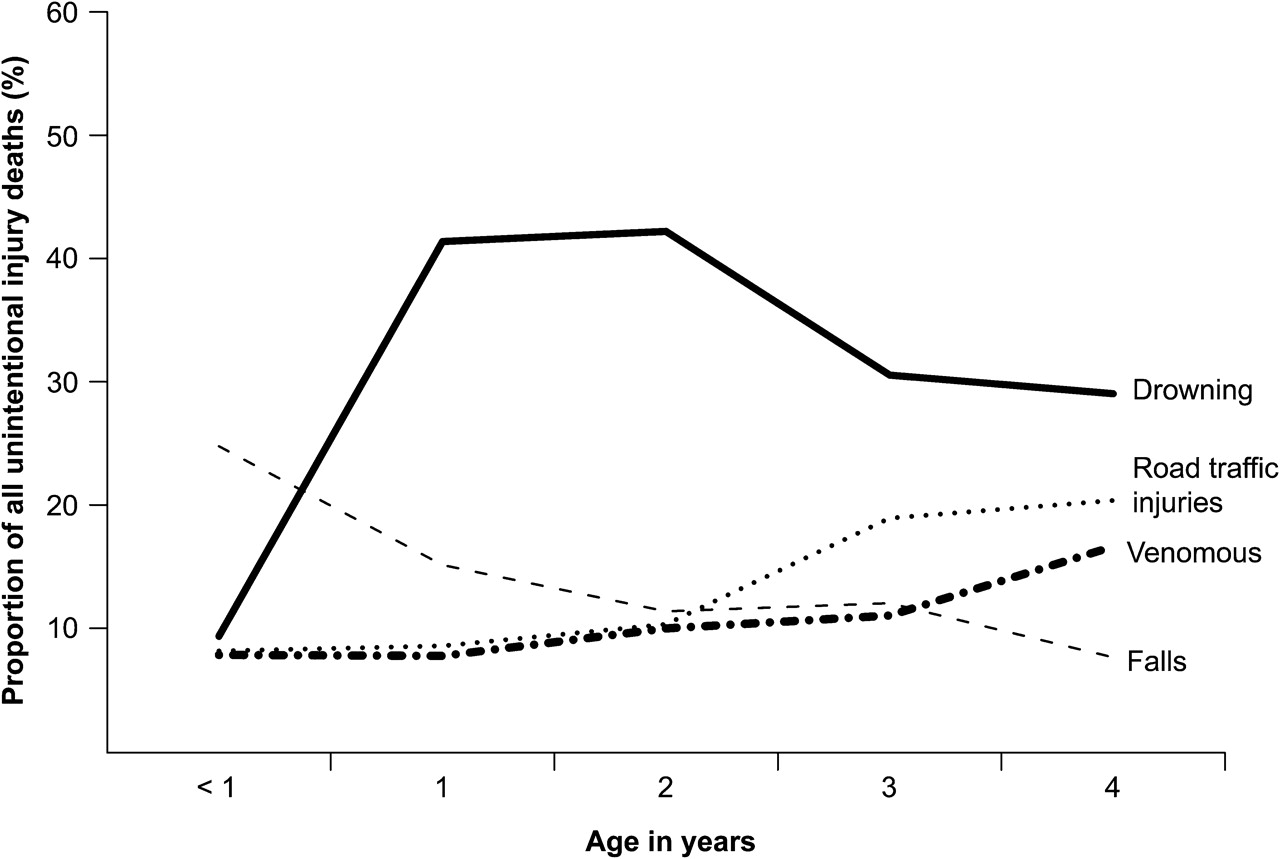
The leading causes of unintentional injury deaths by child age are shown in figure 1. There was a peak in the proportion due to drowning in the 1–2 year age group. The proportion of deaths due to falls declined with age, but road traffic injury and the proportion of deaths due to contact with venomous plants and animals showed an increase with age.

Age-specific proportion of total unintentional injury deaths at 0–4 years of age in India, 2001–2003. Leading causes of unintentional injuries are presented as proportion of all unintentional deaths in the sample.
The Northeastern region had the highest unintentional injury mortality of 398, and the Western region had the lowest (153). The values for the Eastern, Central, Northern, and Southern regions were 330, 312, 303, and 212, respectively. Mortality from unintentional injury in EAG&A states (297) was 18% higher than in non-EAG&A states (257), even though injuries represented a lower proportion of all deaths among children younger than 5 years of age in EAG&A states (2.9% vs 4.2%).
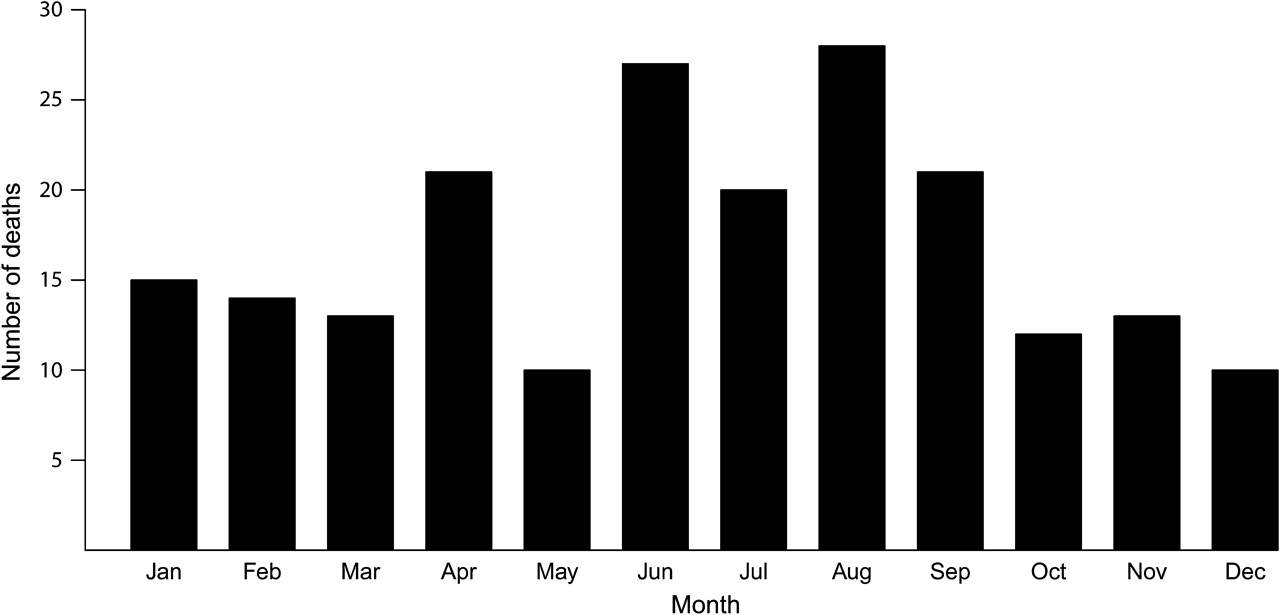
Drowning was the cause of more than 26 000 deaths among children younger than 5 years in 2005 (table 2). Mortality due to drowning was nearly three times higher in rural (110) than urban (35) areas and was higher in boys (97, 99% CI 77 to 121) than girls (69, 99% 85 to 134). Most drowning deaths occurred in the Northeast region, where drowning accounted for 82% of all unintentional injury deaths in children. A seasonal trend was observed in drowning deaths, with a peak in the months of April to September, when different regions of the country have monsoon rains (figure 2). The risk of drowning death was significantly higher than the average annual risk— 27% higher (p=0.002) in the northern monsoon months of July–September. The risk was 16% (p=0.033) higher from April to September, a time period that includes the earlier arrival of monsoon rains in southern parts of India.
Number of unintentional injury-attributed deaths by type, in the present study and estimated national totals for 0–4 years
{kind=link}
{kind=link}
Seasonality of drowning deaths in India, 2001–2003. The monthly distribution of the number of child deaths due to drowning during the study period is presented.
Mortality due to fall injury in children younger than 5 years was 43 (99% CI 31 to 52). Falls were the leading type of injury death in urban areas (24%; mortality 46, 99% CI 21 to 82). Nearly 33% of all falls in the age group were from a height or a building. Among neonates, falls were the leading type of unintentional injury (29% of all unintentional injury deaths). Among infants, 30% (27/90) of unintentional injury deaths among girls were due to falls, compared with 18% (17/95) in boys. Owing to the small numbers, the injury sub-type analysis among neonates is not presented. Overall mortality due to falls in children younger than 5 years was higher in girls (46, 99% CI 30 to 64) than boys (39, 99% CI 25 to 55).
Mortality due to road traffic injury was 39 (99% CI 27 to 48), accounting for 12% of all unintentional injury deaths among children younger than 5 years of age. The proportion of deaths due to road traffic injuries increased with age (figure 1). Road traffic mortality was higher in rural areas (42, 99% CI 28 to 52) than urban areas (34, 99% CI 21 to 68), and higher among boys (43, 99% CI 29 to 53) than girls (37, 99% CI 23 to 69). More than 40% of these deaths were pedestrian deaths from collision with cars or heavy vehicles.
Mortality due to contact with venomous plants and animals was 31 (99% CI 21 to 43). Most of these deaths were caused by snake bites, and the highest number were in the Southern region of India. More than 32% (26/80) of these deaths occurred in July and August. Each of the specific injuries classified as ‘other’ contributed less than 2% to injury deaths among children younger than 5 years.
Discussion
Our nationally representative study based on verbal autopsy has, for the first time, directly estimated that ∼82 000 unintentional injury deaths occurred in India in 2005, which constitutes about 3% of all deaths among children younger than 5 years of age, 1% in children aged less than 1, and 9% in children aged 1–4 years. The findings of our study highlight a significantly higher burden of death due to unintentional injury in children than that estimated by available national sources, particularly for children aged 1–4 years, our estimates for whom are two to three times higher than reported previously.
There are discrepancies between our national estimates and those derived from the rural and urban national sources of mortality data. In the SCD (rural, 1998), 1.3% of deaths in the under-5 age group, 0.7% of deaths in the under-1 age group, and 2.8% of deaths in the 1–4 year age group were due to unintentional injury.14 The MCCD (urban, 2004) reported that a higher proportion of deaths was due to unintentional injury, with 2.5% in children younger than 5 years, 0.6% in those <1 year, and 4.8% in those aged 1–4 years.15 These discrepancies can be explained. The SCD was based on selected primary healthcare centres from selected states. It had methodological issues and problems with coding of cause of death and a high proportion of ill-defined causes of death. Furthermore, MCCD is hospital-based data and hence not representative of cause of death in the population. It also had several limitations such as partial coverage and high proportion of ill-defined causes of death.31 Further, only 12% of the unintentional child injury deaths in our sample occurred in a health facility, and it is possible that these deaths would be missed in datasets that rely on hospital or healthcare centre presentation.
In line with previous research, there were higher proportions of deaths among boys due to drowning, road traffic injuries, and contact with venomous plants and animals.32–34 Increased mobility in children over 1 year and the consequent increased environmental exposure, and lower parental restraint have been suggested as explanations for the increased mortality due to injuries among boys.35 36
Drowning deaths were more common in rural parts of the country where there is greater exposure to open natural bodies of water. This is different from many high-income countries, where drowning is more common in urban areas because of the presence of swimming pools.37 Community perceptions and beliefs related to drowning are also different in this region. A study in Bangladesh reports causal explanations such as enticement of children by ‘evil spirits’, bewitching of mothers so that they forget about the child, and other beliefs related to child drowning. Hence interventions should not only be context-driven, but should also address community beliefs and be culturally acceptable to be effective.38
Drowning deaths were also highest in the Northeastern and Eastern regions, the Ganges delta region, where the states of Bihar and Assam are located. These states are hit heavily by monsoon rains, which cause flooding along the major rivers, such as the Brahmaputra, Ganges, and its tributaries,39 and leave behind several natural open water bodies. Drowning has been recognised as a leading cause of death among children in the neighbouring country of Bangladesh because of similar risk factors.40 It is possible that swimming lessons would prevent drowning deaths,41 although there is a lack of evidence for water safety training in the region. Other effective interventions may include increased awareness among family members about drowning risks, guards for ditches and water holes near households, and organised support for child supervision.42
Falls among children younger than 5 years are also notable in the region of South Asia.43 We found that falls were the second leading cause of unintentional injury death in children, and almost a quarter were falls from building structures. Interventions that may help to reduce falls include the introduction and implementation of safer building laws and codes, safer playgrounds, and increased supervision by parents of young children. Falls were the only type of injury with higher mortality in urban areas for children younger than 5 years, probably because of changes related to urbanisation and multi-storey buildings without safe guards, which increase the risk of children falling from windows and balconies. The ‘Children can't fly’ programme is aimed at preventing child falls from high-rise residential buildings44 and, with adaptation for local context, could be applied in low and middle income countries for environment modification. Similarly for road traffic injuries, system-wide approaches addressing various aspects of the road system, such as development of a safer road environment, measures for better visibility, supervision of child pedestrians, and speed restrictions, may be effective in reducing the burden of road injury in children.45
Falls and fire-related injuries generally occur at home,46 and the rise in all other causes of unintentional injuries, such as road traffic injuries, drowning, and contact with venomous plants and animals, could be associated with the environment outside the home and increased mobility as the child grows, but associations between developmental stage, skills acquisition, and mobility with specific types of injury have been explored in only a few studies.7 47
Verbal autopsy is a reliable method of measuring cause-specific mortality in low- and middle-income countries where medically certified cause of death is not available for the majority of deaths.25 However, it is an indirect method of determining the cause of death and assumes that each disease/condition has a distinct set of signs and symptoms.48 Injuries are quite distinct events and unlikely to be misclassified when reported by the deceased's relatives. Verbal autopsy results for unintentional injuries have previously been validated in adults with high levels of sensitivity (95%) and specificity (85%).49 It is reasonable to assume that, as injury events and related mortality are not unique to any age group, the verbal autopsy methods would perform equally well for child injury deaths. However, in view of the gender preferences in India,23 there may be some misclassification of injury intent, and this may lead to overestimation of unintentional injury deaths, especially among female children.
In conclusion, an estimated 82 000 deaths (99% CI 71 000 to 88 000) were due to unintentional injuries among children younger than 5 years of age in India in 2005. Efforts are required to establish burden of injury-related morbidity, including hospitalisation and disability among children.18 20 In addition, risk factors associated with unintentional injury morbidity and mortality also need to be determined so that evidence-based policies can be designed for prevention and management of injuries among children.
What is already known on this subject
Unintentional injuries are the leading cause of death in children younger than 5 years of age.
Although injury burden is declining in developed countries, it remains high in developing countries such as India.
Data on the epidemiology of unintentional injury in India are scarce.
What this study adds
This is the first study to provide direct estimates of unintentional injury mortality in young children from a nationally representative sample in India.
The study adds to our understanding of types of injury leading to death, which is vital for development of injury prevention policy in the region.
Drowning, falls, and road traffic injuries were found to be the leading causes of injury deaths in children younger than 5 years of age.
Acknowledgments
The RGI established the SRS in 1971 and has continued it ever since, and is collaborating with several of the authors on the ongoing Million Death Study. All study materials are freely available at http://www.cghr.org. The opinions expressed here are those of the authors and do not necessarily represent those of the RGI. A full list of the RGI-CGHR Collaborators can be found at http://www.bmj.com/cgi/data/bmj.c621/DC1/1. We thank Wilson Suraweera for data support.
References
Supplementary materials
Web Only Data
Files in this Data Supplement:
Footnotes
See Editorial, p 145
Funding External funding is from the Fogarty International Center of the US National Institutes of Health (grant R01 TW05991–01]), Canadian Institute of Health Research (CIHR; IEG-53506), International Research Development Centre (Grant 102172), and Li Ka Shing Knowledge Institute St Michael's Hospital, University of Toronto (CGHR support). PJ is supported by the Canada Research Chair program.
Competing interests None.
Ethics approval The SRS enrolment is on a voluntary basis, and its confidentiality and consent procedures are defined as part of the Registration of Births and Deaths Act, 1969. Oral consent was obtained in the first SRS sample frame. The study has been approved by the review boards of the Post-Graduate Institute of Medical Education and Research, St Michael's Hospital, and the Indian Council of Medical Research's Health Ministry's Screening Committee.
Provenance and peer review Not commissioned; externally peer reviewed.