Article Text

Abstract
Objectives: To critically synthesise current knowledge of the patterns of injuries and risk factors for injury in school-aged children, to summarise the evidence and support effective child injury prevention initiatives.
Design: Systematic review.
Selection criteria and methods: Prospective cohort studies reporting unintentional injuries in healthy children aged 5–18 years were identified by searching 15 electronic databases and additional grey literature sources. A narrative synthesis was conducted of papers meeting quality criteria, with risk factors analysed at individual, family and environmental levels. Limitations of existing evidence were considered.
Results: 44 papers from 18 different cohort studies met the inclusion criteria. There were broad and consistent patterns of injury across time and place. Male sex, psychological, behavioural and risk-taking behaviour problems, having a large number of siblings, and a young mother were all associated with increased injury occurrence across more than one cohort and setting.
Conclusions: Descriptive epidemiology and risk factors for injury were derived from prospective cohort studies, but few studies used the full potential of their design. Opportunities to use repeated measures to assess temporal changes in injury occurrence, and the exploration of risk factors, particularly those related to the child’s environment, have rarely been undertaken. Few studies were conducted in low/middle-income countries where the burden of injury is greatest. These findings should be considered when planning future research and prevention initiatives.
Statistics from Altmetric.com
Childhood injury continues to be an international public health problem. More than 875 000 children die each year as a result of injury, with 95% of child deaths occurring to children in low/middle-income countries. For every child who dies, many more receive injuries resulting in disability and discomfort. Non-fatal injuries affect the lives of 10–30 million children and adolescents each year.1 Reducing this substantially preventable burden requires the collation and interpretation of existing data on childhood injury to contribute to hypothesis generation and intervention development.23
The development and implementation of effective intervention programmes requires a knowledge of risk and protective factors for childhood injury. These factors can be explored at a number of different levels: an individual level, a family level and the level of the environment in which the child lives. There are differences in injury occurrence between countries, and between groups within countries, thus understanding the factors beyond the individual child are important for identifying risks in different settings and populations.3 Reports of injury occurrence and risk factors for injury are derived from a variety of study designs including case–control, cohort and population registry follow-up studies. The primary advantage of prospective cohort studies over other study designs is the collection of information on the circumstances surrounding the injury and individual characteristics of children, before the occurrence of injury. This temporal relationship reduces the potential for recall bias that threatens the validity of case–control study findings, and is often absent from population registry follow-up studies. Prospective cohort studies reporting injury in children are therefore more likely to be valid than other study designs as a means of examining prevalence and associated risk factors.
Systematic reviews have a well-established methodology that overcomes the biases in traditional methods of reviewing the literature.45 This paper presents the findings of a systematic review of child cohort studies reporting unintentional injury in school-aged children. It summarises the knowledge and gaps in injury epidemiology, exploring risk factors for injury at individual, family and environmental levels, and identifies methodological issues that may be of relevance for planning future cohort studies.
METHODS
Inclusion and exclusion criteria
Inclusion criteria for studies were: (a) the study design was a prospective cohort, longitudinal or follow-up study in which healthy children up to 18 years old were recruited through personal or parental consent; (b) outcomes were unintentional physical injuries sustained between the ages of 5 and 18 years. Studies were excluded if: (a) they used population-based or record-based cohorts, where no active recruitment to the study occurred; (b) children were either selectively recruited because of a specific diagnosis, disability or injury, or undertook an activity that placed them at increased risk of injury, eg, competitive sports; (c) if the study only collected outcomes related to psychological or psychiatric injuries. No language or date restrictions were applied.
Search process
Electronic databases were searched using a search strategy developed in Medline through an iterative manner to achieve optimum sensitivity, while retaining practical specificity. The strategy explored the three concept areas of children/young people, injuries, and cohort studies using a combination of text and thesaurus terms (supplementary electronic data; box 1). The strategy was adapted and applied to 14 databases (supplementary electronic data; box 2). Searches took place in January and February 2006. Using reference management software where possible, duplicate references and ineligible studies were excluded on the basis of their design, recruitment, population, or study outcomes (where specified in sufficient detail). The full texts of remaining references were obtained, and further ineligible studies were excluded using the same criteria.
Grey literature sources included the bibliographies of included studies; authors of potentially eligible studies were contacted to confirm eligibility, and, if eligible, to request details of further published and unpublished work, departmental or institutional reports or additional unpublished data; a Medline author search (1966 to 2006) was undertaken for further publications by the lead author of included studies; an internet search for websites relating to known child cohorts was conducted to identify contacts and search publication lists for papers and reports of injury outcomes.
Data extraction
A data extraction form was developed and piloted on five papers by three authors (JM, ET, MB) and modified accordingly. Independent dual data extraction (JM and either ET or MB) was undertaken from all included studies on the number and description of study participants, study design, methods and outcomes recorded. Reviewers were not blinded to the names of journals, the authors or institutions, or the results when extracting data on study methods. Data were compared and differences resolved through discussion or clarification with the author where possible.
To assess study quality, each included paper was critically appraised using questions adapted from CASP (Critical Appraisal Skills Programme “12 questions to help you make sense of a cohort study”).6 These published quality criteria were adapted by excluding one question relating to local application of evidence, since local relevance was not applicable to an international review of the literature. The two authors extracting data undertook the quality assessments. These were collated, and discrepancies were resolved by discussion. A judgement on the overall quality of the study was made after discussion, and an author-designed quality rating was assigned, where A = sound methodology and clear reporting, B = minor methodological or reporting concerns (but not to the extent that the validity of the reported results was questioned), and C = significant methodological or reporting concerns such that serious doubt was placed on the validity of the reported results. Studies given a C quality rating were not considered suitable for inclusion in the synthesis of the review.
Data analysis
Synthesis was achieved through a two-stage narrative process: firstly, a within-study review of papers reporting specific cohort studies, to determine the contribution of that cohort study to the research field and to report consistency of findings between papers reporting that study; secondly, through a between-study review, to summarise the findings identified across different cohort studies, to identify differences and possible reasons for those differences between studies, and to identify gaps in the knowledge base.5 Differences between groups were reported as odds ratios (ORs) or relative risk (RR) where reported, and as p values where no OR or RR was given. Differences were considered important if they were greater than could have occurred by chance (ie, 95% CIs did not include OR = 1.00 or RR = 1.00, or p values were <0.05). Subgroups specified a priori for the between-study review included the age of the child (age 5–11 years designated “primary” school age, and age 12–18 years designated “post-primary” school age), economic status of the country of study (high-income countries versus middle/low-income countries, as defined by the World Bank7), and date of study (studies before 1980 versus those recruited since 1980). Meta-analysis of results of cohort studies was considered inappropriate because of the potential problems associated with unrecognised confounding in observational study designs and the heterogeneity of the studies identified.89
RESULTS
Forty-four papers from 18 different cohorts met the inclusion criteria and had data available for analysis (fig 1, table 1). Attempts were made to contact authors or study directors; nine contacts responded. No unpublished papers were identified. Five cohorts recruited infants at birth, and the remaining 13 studies recruited older children. Fourteen were based in high-income countries (UK, New Zealand, USA and Canada), and four were from middle/low-income countries (Thailand,10 Taiwan11 and China12–14). Four cohorts used a nationally representative sampling method, while the remainder sampled particular geographical areas (often urban). The oldest cohort study was recruited in the UK in 1947,15 and the most recent in China in 2002.13 The quality of the included papers was generally satisfactory, with only one paper given a C rating.16

Flow chart of identified eligible studies. Note: 43 of the papers have data for descriptive epidemiology and 27 papers have data for analysis of risk/protective factors. *Key words and indexing terms were also used to identify ineligible papers where these were available. †The majority of grey literature papers were identified by contacting the author of an included study or by performing an electronic database search for further publications by the author of an included study.
Descriptive epidemiology of injuries
Of papers describing injuries, 15 reported primary school-aged children, 18 post-primary school-aged children and nine described injuries across both age periods. The text below provides an overview of the descriptive injury results, and the tables and figures provide details from specific studies. The range of outcomes reported by individual papers is summarised in table S1 (supplementary electronic data). The average proportion of the cohort sustaining both any injury and multiple injuries varied markedly, largely because of differences in injury and outcome definitions. All papers reporting any injury or multiple injuries by gender found that injuries were more common in boys than girls, with the difference appearing to widen in the post-primary school-age group (table 2). Only nine cohorts reported the ethnic group of the children or their mothers.
Type and mechanism of injury
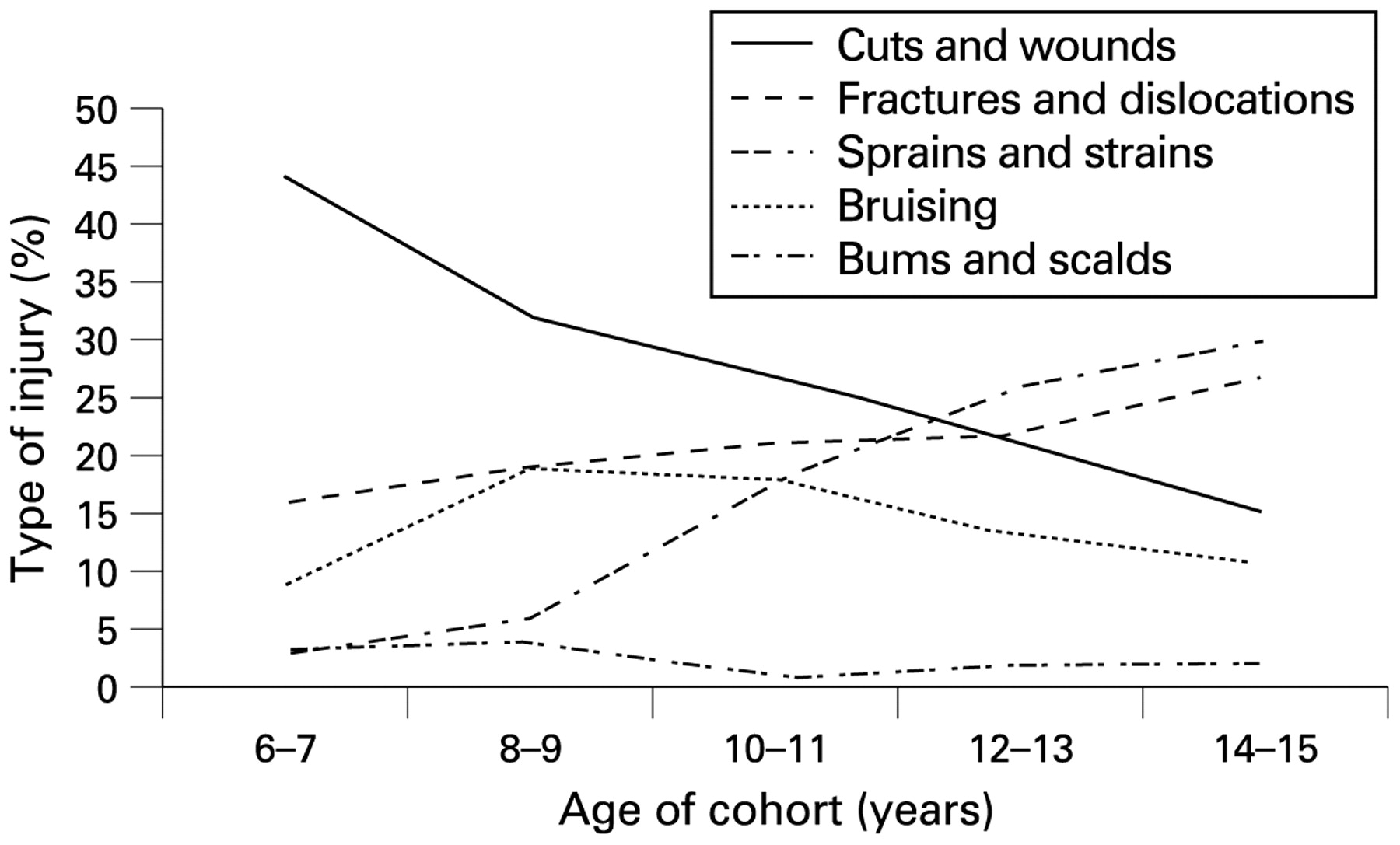
The New Zealand Dunedin Multidisciplinary Child Development Study (DMCDS)17–21 described injuries occurring between the ages of 6 and 15 years, in greater detail than any other study. The changing patterns of injuries with age are illustrated in fig 2, and these findings were consistent with those from four papers from older UK cohorts1522–24 with respect to fractures, and by a paper from a middle-income country with respect to lacerations and sprains/strains.10 The latter paper reported that 12% of injuries were near-drownings. Only two other cohorts reported near-drowning cases; both were older UK studies with rates of ⩽3%.2425
Four papers from three cohorts (UK, New Zealand and China) reported the proportion of injuries affecting different parts of the body.13202123 Upper limbs were affected in 32–36% of injury events reported, lower limbs in 29–39% of events, and the head or face in 19–23% of injury events. One Taiwanese cohort11 found that rates of upper limb injuries were double those affecting the lower limb. Falls were the most often reported mechanism of injury, followed by injuries involving sharp and blunt objects, although the proportions of the latter two categories vary considerably between papers because of different definitions. Injuries sustained during sports participation were rarely specified2126 (table S2).
Location of injury event
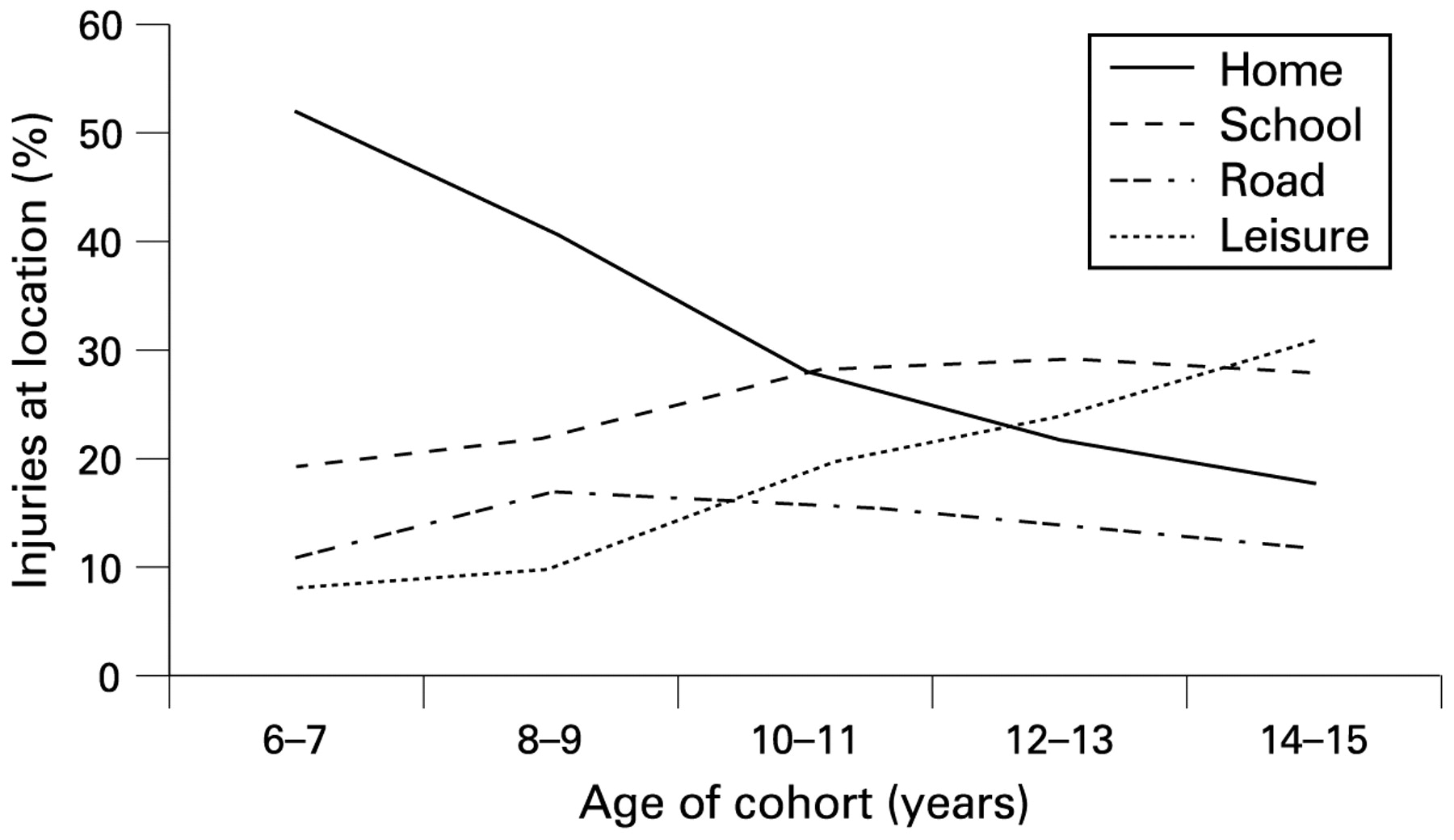
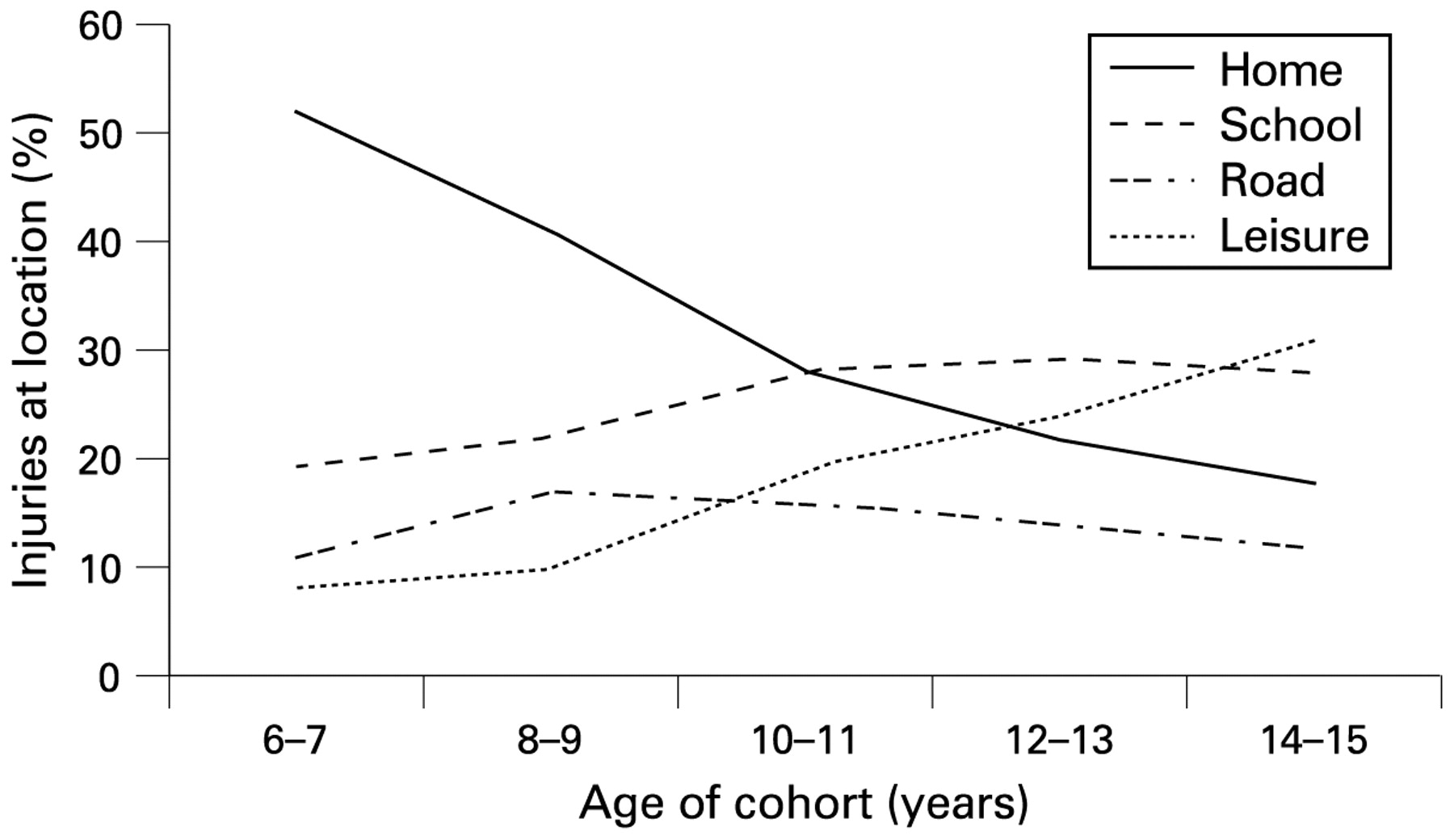
The location of the reported injury event changed as the children aged. The home became less important as more injuries occurred in school and leisure areas. This is shown clearly in the DMCDS cohort17–21 (fig 3). Even at home, injuries became increasingly likely to occur outside, eg, in the garden, yard, driveway or path.182021 Injuries on the road peaked at 8–9 years in the DMCDS, but never formed a large proportion of injury locations. Two UK cohorts27–30 and one from China13 reported similar locations for children of post-primary school age, despite varying in geographical setting and date of recruitment (1969–2005). One older UK cohort15 and one cohort from the USA26 both found a greater proportion of injuries occurring in the road environment (table S3).
{kind=link}
{kind=link}
{kind=link}
Severity and consequences of injury
Comparison of severity of reported injuries was difficult because of the number of methods used to categorise severity of injuries. Seven papers reporting healthcare service use as a proxy for severity often defined an injury as one requiring medical attention. Reported injuries were more likely to have required either primary care (7–33%) or outpatient/emergency room care (13–65%) than hospital admission (<10%) (table S4).1517–2131 Only one cohort stated the proportion of reported injuries receiving care outside of health service settings, with 70% of injuries being managed by the child or their carer, 27% managed by a primary care doctor, and 4% admitted to hospital.1314 The Abbreviated Injury Scale score was used in five papers18–2123 from two cohort studies (New Zealand and UK) and suggested that, as children became older, the injuries they sustained were likely to be less severe (table S5). Two cohorts used duration of time away from school as a proxy for injury severity and suggested that between 4.0%32 and 7.2% of children missed more than a week from school as a consequence of their injury.13
Three cohorts reported fatal injuries. In the New Zealand DMCDS1933 cohort and a US cohort,26 unintentional fatal injuries were due to road traffic incidents. In the cohort from Thailand,10 0.05% of the cohort (n = 20) died from unintentional injury over 2 years of follow-up, 13 (65%) due to road traffic crashes, and six (30%) due to drowning. Only two cohorts reported any short-term or long-term consequences of the injuries sustained. In one UK study,15 0.5% (n = 3) received long-term severe disabilities. In the New Zealand DMCDS, 70% of the injuries reported at 12–13 years resulted in some limitation of activities from the day after the injury.20 Most were of short duration, but 20% lasted longer than 1 month and 1% (n = 8) resulted in a permanent disability. Similar findings emerged 2 years later when this assessment was repeated.21
Risk factors for injury
Twenty-seven papers from 15 cohorts reported some analysis of risk factors for injury (tables 3 and S6).
Child factors
Male sex was a significant risk factor for injury across a range of geographical settings (China, USA, New Zealand, UK and Canada) and periods of time (1958–2002).1013223435 In contrast with the descriptive data reported, the two papers that analysed injury risk by age of the child found either no differences greater than chance36 or more injuries in younger children.13 Four US cohorts2635–37 reported no statistically significant differences in injury occurrence between different ethnic groups, in contrast with one study from China13 that found more injuries in minority ethnic groups. Only one paper reported a history of injury as a risk factor for future injury, finding increased risk greater than expected by chance.38
Risk factors related to the physical development of the child were not consistently found to be associated with injury, although cohorts rarely analysed identical factors. Being taller and heavier than their peers was an independent risk factor for fractures in children from New Zealand,39 while post-primary school UK boys were more likely to sustain road traffic injuries if of short stature.40 The latter study also reported increased risk of traffic injuries with sensory deficit (unspecified), in contrast with papers reporting no increased risk of any injury associated with colour vision deficit41 or amblyopia.42 Studies exploring the impact of poor coordination or motor development found little evidence of independent increased risk in cohorts from both the UK40 and New Zealand.43
Learning ability was not associated with risk of injury in the two studies reporting this variable.4043 Children with psychological difficulties were consistently found to have increased risks across both geographical setting (UK and China) and time (1958, 2001 and 2002).121440 Hyperactivity was an independent risk factor in two UK cohorts,4044 but not in a Canadian study.34 Behavioural difficulties (such as antisocial or aggressive behaviours) were reported in 10 different cohorts, with authors reporting increased risk in both primary school-aged children12243845 and post-primary school-aged children,2628293644 and across time and place. A smaller number of papers did not report increased risk of injury with behavioural difficulties.34354346 Risk-taking behaviour was consistently associated with injury greater than expected by chance generally2628 and for specific risk behaviours including daily smoking,39 lifetime marijuana use35 and recent alcohol use.3544
Family factors
Living in a family with many siblings was associated with increased risk of injury greater than chance in three UK cohorts,2428384547 in contrast with a New Zealand cohort of primary school-aged children43 and an adolescent cohort from China.1314 A relatively young mother at the time of the child’s birth was independently associated with injury risk in cohorts from both the UK (where “young” was defined as 20–24 years)38 and China (where “young” was defined as under 22 years).12 Living without either one or both of the natural parents varied from increasing injury risk40 to decreasing the risk13 to making no difference.1443
None of the measures of socioeconomic status (SES) of the child’s family were consistent in associations with injury risk. Cohorts from UK and New Zealand showed no significant differences in injury rates between families of different social class as determined by parental occupation.234348 When income was used as an indicator of SES, higher rates of injury were associated with either lower incomes28 or middle band incomes,13 or no association with poverty was found,36 and increased risk of injury was reported in families with lower13 or higher12 parental education or was not associated with parental education.35 The West of Scotland cohort study30 examined adolescent injury risk using four measures of SES. Unpublished data indicated no significant association with injury for burn injuries or road traffic injuries, but a significant trend for assault injuries in boys (increased injuries in lower SES groups), and a reverse gradient for sports injuries in girls (increased injuries in higher SES groups).
Poor maternal mental health was associated with increased risk of injuries in primary school-aged children in two UK cohorts,1545 but not in New Zealand.43 Consistent parenting (defined using the McMaster Family Assessment Device)34 and parental injury-prevention measures (such as the safe keeping of poisons and sharp or hot objects)12 reduced injuries greater than by chance, while the effect of parental supervision was inconclusive.1535 Indicators of poor family functioning were associated with traffic injuries in one UK cohort,40 but no association between family relationships, family adversity or family dysfunction and child injury were identified in two cohorts from New Zealand.4346
Environmental factors
Only one cohort reported the influence of a poor physical home environment, with increased risk of traffic injuries in boys living in homes lacking basic amenities.40 Frequent house moves in adolescence were associated with injury in a UK cohort44 but not in primary school children from New Zealand.43 Three cohorts studied the wider environment; a Canadian study34 explored neighbourhood disadvantage using an index of factors, while one UK study23 and one US37 cohort explored measures of regional disadvantage. None were able to identify an independent association greater than could have occurred by chance.
DISCUSSION
Principal findings
The pattern and circumstances of injuries change as children progress from 5 to 18 years; in general, there is a widening difference in injury occurrence rates between boys and girls, an increase in the frequency of injuries with an apparent reduction in the severity of injuries, and a tendency for injuries to occur in sports and leisure locations. Falls are consistently the primary mechanism of injury, but the type of injury changes with age from cuts and lacerations to sprains and fractures. We were unable to identify patterns relating to the consequences of injury because of very limited reporting.
Most analyses of risk factors were at the individual level (23/27 papers), a smaller number explored family factors (19/27), and very few considered the wider environment (6/27). Male gender, relatively high weight or height, psychological difficulties, behavioural problems, risk-taking behaviour, having a large number of siblings, having older siblings, and having a younger mother were all associated with an increased risk of subsequent injury across more than one cohort and setting. The risk factors related to the individual child often reflect the child increasing their exposure to injury risk situations, or may result in injury from placing themselves in injury risk situations where they lack the developmental or judgement skills to prevent injury. Having older siblings may be a risk factor because carers perceive that older siblings will supervise younger children, when in practice the younger children try to copy their older brothers and sisters. Younger mothers, compared with average age or older mothers, may be less aware of the risks a child will encounter as they develop and grow. Understanding such factors helps to indicate groups and situations where interventions should be considered and the effectiveness of such interventions assessed. Factors not often explored or inconsistently associated with injury risk included a history of injury, having a sensory deficit, poor learning ability, attention, parental health or parenting ability, family dysfunction, SES and the wider environment of the child.
Methodological issues
This review focused on evidence from prospective cohort studies, enabling a wide range of injury events of variable severity to be reported. A consequence of this decision was that very few child deaths from injury were included in the risk factor analysis. Collating data from case–control studies where cases were children who had died from injury might have yielded different results and gained further insight into preventing these severest of injuries. Such research is warranted.
What is already known on this topic
Childhood unintentional injury is a leading cause of preventable disability and death.
Prospective cohort studies have the potential to provide data on the occurrence and risk factors for injury.
What this study adds
Some patterns of injury occurrence and risk factors are consistent across different populations and settings.
Cohort studies have rarely undertaken repeated measures of injury occurrence to illustrate temporal trends.
Risk factors related to the family and the environment of the child are likely to be important but under-researched.
More papers were identified through grey literature searching than from electronic databases, which was often due to the absence of an indexing term relating to the study design. Randomised controlled trials often have their study design indexed by electronic databases, but this review suggests that other study designs, such as cohort studies, are not routinely indexed. Systematic review methodology increasingly considers the inclusion of non-trial and observational evidence to support the development of policy and the implementation of interventions. Hence all study designs require adequate indexing to allow identification. All the included papers were in English, except for one in Mandarin,12 and no unpublished papers were identified, although one author did provide additional unpublished data.30 The predominance of papers in English is not unexpected, since the expense and infrastructure required to conduct cohort studies is likely to have limited them to high-income countries. In this review, four studies were identified from low/middle-income countries, and three of these reported in English. Positive reporting bias was common, with authors stating that they collected or analysed data but they only published selected results, and this risks overestimation of the effects of the reported factors. A further eight papers were identified49–56 that met the inclusion criteria except for reporting data for children younger or older than the 5–18 age group. Despite attempts to contact authors, data limited to the age period of interest were not available, and these papers were excluded. The absence of these data may have influenced the findings and conclusions drawn.
Heterogeneity existed between included studies with respect to date of study, setting, participants, methodology, and classification systems for measuring risk factors or assessing injury severity. The variety of methods used to classify injury severity reflects the previous lack of widely accepted classification systems. Authors used different definitions of “an injury”, although most defined an injury as that requiring medical attention. Older studies tended to record only the more severe (eg, hospitalised) injuries. The quality of the included papers was generally satisfactory. Only one paper16 was completely excluded from the synthesis because of selective reporting and inability to obtain complete data. However, authors rarely reported comparisons of recruited and non-recruited children, or those lost to follow-up compared with those retained. Loss to follow-up was reported in 71% of papers, and varied between 0.8%13 and 52.7%.44 The modal period of follow-up was 1–2 years but varied between 9 months11 and 15 years.15
Methods for synthesising data from observational studies are still being developed, but the risks of unrecognised confounding when calculating statistical estimates of effect are well reported.8957 The narrative synthesis used in this review has attempted to be a transparent and objective method to summarise the literature identified. Detailed inclusion of cohort studies that are reported in multiple publications (eg, the DMCDS cohort and the National Child Development Study) risks over-weighting their findings, but not including all publications would lose valuable data. The DMCDS was the only cohort providing in-depth sequential reporting of type and circumstances of injury in an increasingly ageing cohort, thereby illustrating changing patterns of risk. Individuals within clusters are more similar than individuals between clusters, limiting the ability to generalise findings outside of the cluster. Only four of the 18 cohorts identified children using a nationwide sampling frame. The remainder were based in geographical areas that will have had some element of clustering effects. The majority of studies came from high-income countries where risk factors may differ from those in middle/low-income countries. It is possible that further studies from low/middle-income countries may have been identified if additional non-English databases had been included in the search strategy.
This review has attempted to be robust in the methodology used and transparent in reporting, in an attempt to provide an unbiased overview of the evidence available. Even so, methodological decisions made along the way have been based on judgement and opinion, and are therefore not immune to criticism. In addition, the findings of this review need to be considered in the context of epidemiological reports of injury in school-aged children that have arisen from other study designs, and the changing social contexts and experiences of children and adolescents. Children engaged in competitive sport were excluded from this review, yet their risks of injury are well recognised. Understanding of these risks and the effectiveness of interventions to prevent such injuries warrant further study.
IMPLICATIONS AND FUTURE RESEARCH
This review has identified a number of gaps that should be considered when planning future research. Cohort studies are expensive and challenging study designs to deliver. Existing studies should maximise the potential of the design by undertaking repeated measures of injury and risk factor occurrence, and following-up children over extended periods of time. The association between low SES and increased risk of injury occurrence failed to be consistently replicated in this review, yet is known to exist from descriptive epidemiology. Comparisons of risk analyses by severity of injury and environmental disadvantage were complicated by the use of variable definitions. The use of internationally recognised classifications of SES, severity of injury and measures of neighbourhood disadvantage would greatly enhance the ability to compare results from different studies. It is possible that real associations between risk factors and injuries may only exist at specific levels of injury severity or for particular definitions of injury and this warrants further exploration. The paucity of studies reporting the impact of the physical home environment and neighbourhoods on injury occurrence suggested that either positive reporting bias or publication bias was obscuring this research, or that it remains to be undertaken. New cohort studies should be considered in low/middle-income countries where the vast majority of child injury occurs. Where established, such studies should be supported by experienced study teams in high-income countries. Risk factors that are consistently associated with injury across international boundaries may be particularly valuable for targeting groups or situations when designing targeted prevention initiatives.
CONCLUSIONS
This review has attempted to summarise our knowledge of unintentional injury in school-aged children that is available from cohort studies. It has shown broad and consistent patterns of injury across time and geographical location, and identified a limited number of factors consistently associated with the increased risk of injury in this age group. The use of repeated measures over time within cohort studies has been rarely used to monitor changing patterns of injury with age, and that follow-up has often been limited to 2 years or less. Individual child factors cannot account for all inter-country variation in injury occurrence, and therefore further research is needed to explore environmental and societal factors associated with increased injury risk, particularly in middle/low-income countries.
This review has also demonstrated the enduring value of cohort studies as a methodology to describe injury occurrence and to assess risk factors for injury. Such patterns are important for the generation of hypotheses of causation and to inform the targeting and development of new interventions to reduce the unnecessary burden of unintentional childhood injury.
Acknowledgments
We thank Professor Alan Emond and Dr Jon Pollock for advice during the development of the review, Ms Esther Heijnens for administrative support, and the Library staff at the University of the West of England, Bristol.
REFERENCES
Supplementary materials
web only appendix 15/2/111
Files in this Data Supplement:
Footnotes
Additional tables and boxes are published online only at http://injuryprevention.bmj.com/content/vol15/issue2
Contributors: All authors of this paper fulfil the criteria for authorship, and there are no other people who fulfil the criteria but have not been listed as authors. All authors were involved in the conception and design of the review. JM developed and conducted the searches and identified the included studies. JM, ET and MB conducted the data extraction and critical appraisal. JM conducted the analyses and prepared the drafts with critical support from ET, MB and SG. JM is the guarantor.
Funding: None.
Competing interests: None.