Article Text

Abstract
Background: The proportion of injury deaths with unspecified external cause codes has been used as an indicator of the level of comprehensiveness and specificity of information on death certificates provided by certifiers.
Objective: To compare the proportion of unspecified external cause codes across countries.
Methods: Multiple-cause-of-death mortality data for people who died in 2001 due to external causes in Australia, Sweden, Taiwan and the USA were used for this international comparison study. The proportion of injury deaths coded as due to an unspecified external cause (International Statistical Classification of Diseases and Related Health Problems, Tenth Revision, ICD-10, chapter XX) to all injury deaths in each block was calculated.
Results: Sweden (33%) had the highest proportion of use of the least specific code (ICD-10 code X59 exposure to unspecified factor), followed by Australia (17%), Taiwan (13%) and the USA (7%). More than two-thirds of the deceased for whom an ICD-10 code X59 was assigned in Sweden and Australia were those aged ⩾65 years, and more than half of them had femoral fractures. The percentage of use of the unspecified codes within specific groups of external causes was relatively high for falls and unintentional drowning.
Conclusions: Caution should be used in examining the compensatory effects of the unspecified external event code (ICD-10 code X59) on specific external causes (especially falls) when making international comparisons. Efforts are needed to educate certifiers to report sufficient information for specific coding so as to provide more useful information for injury prevention.
- ICD-10, International Statistical Classification of Diseases and Related Health Problems, Tenth Revision
- NCIS, National Coroners Information System
Statistics from Altmetric.com
- ICD-10, International Statistical Classification of Diseases and Related Health Problems, Tenth Revision
- NCIS, National Coroners Information System
Ideally, a good classification scheme for external causes of injury deaths should provide relevant information for injury prevention.1–5 A high degree of specificity in mortality data and improvements in the documentation of the circumstances of an injury-causing event is essential for injury prevention purposes.3 For example, the four-character code for transport injuries in ICD-10 (International Statistical Classification of Diseases and Related Health Problems, Tenth Revision) comprises the information regarding the mode of transport of the victim, and also the victim’s counterpart or the circumstances of the injury and the role of the victim (eg, driver or passenger) and whether the event was a traffic or non-traffic accident.6 Many new categories have been added for falls in ICD-10 (W04–W08) to provide more detailed information compared with that available in its predecessor, ICD-9. ICD-10 further separates unintentional drowning into drowning while in water (W65, W67 and W69) and drowning which occurs due to a fall into water (W66, W68 and W70). These two circumstances have quite different implications for injury prevention.6
Realistically, however, certifiers may not report sufficient information on the death certificate to take advantage of the specificity in the classification scheme. For example, if the certifier reported only “accidental head injury” on the death certificate, the coder can only assign an unspecified underlying cause code—that is, ICD-10 code X59 (exposure to unspecified factor, accident not otherwise specified) for this death certificate. If the certifier wrote “head injury due to transport accident” on the death certificate, the coder would assign a less unspecified ICD-10 code V99 (unspecified transport accident) for this case. Only when certifier provides more complete information, such as head injury to a motorcyclist in collision with bus, can the coder give a specific ICD-10 code V244 (motorcycle rider injured in collision with heavy transport vehicle or bus). Therefore, the proportion of injury deaths with unspecified external cause codes can be used as an indicator of the level of sufficiency and specificity of the information reported by certifiers on the death certificate for external causes of death.
There are two injury-prevention implications in examining the proportion of unspecified external causes. If a country has a large number of injury deaths coded as ICD-10 code X59, there would be compensatory effects on the number of deaths due to other specific external causes, such as motor vehicle crashes, falls or drowning. This will result in underestimation of the magnitude of these deaths and biased interpretation of international comparisons may result. Furthermore, if a country has high percentage of unspecified codes for particular external causes—for example, ICD-10 code W19 (unspecified falls) there will be insufficiently detailed information about the circumstances of the fall (such as falls involving wheelchairs, beds, chairs or other furniture and so on) for designing relevant injury prevention programs.
Several studies conducted in the past have dealt with the reporting of unspecified injuries,5,7 risk factors associated with unspecified causes8 and the quality of certification9; but no study has assessed the specificity of information reported on death certificates at an international level. Conducted as part of the International Collaborative Effort on Automating Mortality Statistics (ICE) initiated by the USA National Center for Health Statistics,10 the aim of this study was to compare the proportion of injury deaths with unspecified external cause codes between Australia, Sweden, Taiwan and the USA. The results of this study will provide some evidence to identify the extent of gaps between the ideal and the reality in classifying external causes of death in different countries.
Because the number of deaths coded to ICD-10 code X59 would have compensatory effects on the number of deaths due to other, more specific, external causes, a more detailed analysis of the use of ICD-10 code X59 was conducted. One important change between ICD-9 and ICD-10 is the failure to include an ICD-10 equivalent to ICD-9 code E887 (fracture, cause unspecified) with the falls block (in ICD-9, codes E880–E888). If a fracture is mentioned without external cause specified, the underlying cause of death is coded to E887 in ICD-9 and X59 in ICD-10. X59 does not distinguish between fracture- and non-fracture-related causes. We used multiple-causes-of-death data to determine how many of the deaths among elderly people in X59 had femoral fracture.
METHODS
Multiple-causes-of-death mortality data for deaths in 2001 with underlying-cause-of-death due to external causes (coded to chapter XX of ICD-10) were provided by four countries participating in the International Collaborative Effort on Automating Mortality Statistics—that is, Australia, Sweden, Taiwan and the USA. All four participating countries use the same automated coding system for selection of the underlying-cause-of-death, therefore there were believed to be few coding artifacts in this international comparison.
Chapter XX is subdivided into several homogeneous blocks of three-character categories (examples are given in table 1). In each block, one category is designated for unspecified circumstances. Table 2 lists all unspecified external cause codes with titles. We excluded the codes that combine both other and unspecified events (ICD-10 codes W49, W64, W99, X19, X39, X49 and Y82), because it is impossible to distinguish between specified and unspecified circumstances using only these codes. We also calculated the proportion of unspecified falls (ICD-10 code W19) by age for each country.
Proportion of injury deaths with unspecified codes in chapter XX injury blocks of International Statistical Classification of Diseases and Related Health Problems, Tenth Revision, by country, 2001
Unspecified code in each block of three-character categories in chapter XX of the International Statistical Classification of Diseases and Related Health Problems, Tenth Revision
For those deaths with underlying cause coded as ICD-10 code X59 (exposure to unspecified factor, accident not otherwise specified) and W19 (unspecified falls), we use multiple-causes-of-death data to examine the proportion of these deaths coded with an associated ICD-10 injury code S72 (fracture to femur) or S00–S09 (injuries to the head) for decedents aged ⩾65 years.
RESULTS
Table 1 presents the proportion of injury deaths coded as unspecified. Sweden (33%) had the highest percentage of deaths reported as due to an unspecified factor (ICD-10 code X59), followed by Australia (17%), Taiwan (13%), and the USA (7%). Sweden also had the highest percentage of deaths from unspecified falls (64% of all fall deaths), followed by Australia (56%), the USA (51%) and Taiwan (49%). The proportion of unspecified falls increased with age in each country (table 3).
Proportion of unspecified fall deaths (International Statistical Classification of Diseases and Related Health Problems, Tenth Revision, ICD-10 code W19) among all falls (ICD-10 codes W00–W19) by age and country, 2001
Table 4 presents the results of analysis using multiple-causes-of-death data. Of those decedents aged ⩾65 years in whom ICD-10 code X59 was assigned, more than half had femoral fractures (ICD-10 injury code S72) in Australia, Sweden and the USA. Of those dying from unspecified falls (ICD-10 code W19) aged ⩾65 years, less than one-third had femoral fractures. In Taiwan, only 2.3% of unspecified falls involved femoral fracture and 89% (235/264) had associated head injury codes (ICD-10 code S00–S09).
Proportion of unspecified external cause and unspecified falls deaths (International Statistical Classification of Diseases and Related Health Problems, Tenth Revision, ICD-10 code X59 and W19) aged ⩾65 years with femoral fracture (ICD-10 code S72) by country, 2001
Taiwan had an unusually high percentage (99%) of unspecified circumstances for unintentional drowning, followed by Sweden (47%), the USA (35%) and Australia (13%). We also found relatively high percentages of unspecified code use for transport accidents (87%) and incidents involving fire and flames (98%) in Taiwan and other accidental threats to breathing (33%) in Sweden compared with the other three countries. Of the 33 deaths that had been coded as ICD-10 code W84 (unspecified threat to breathing) in Sweden, 24 of the deceased were aged ⩾65 years. We could not find more specific information for these deaths using multiple-cause-of-death data.
On the contrary, Australia (2%) and Sweden (3%) had relatively low percentages of use of unspecified codes for transport accidents compared with Taiwan (87%) and the USA (23%). Table 5 illustrates the number of deaths coded to the various four-character unspecified motor vehicle traffic accident codes. All the four participating countries had low percentages of intentional self-harm deaths caused by unspecified means (ICD-10 code X84). We also found some variations in the proportion of use of codes for an unspecified event of undetermined intent (ICD-10 code Y34) across countries, from 0% in Australia to 9% in Taiwan.
Number of motor vehicle traffic deaths with four-character unspecified codes by country, 2001
DISCUSSION
Obvious gaps existed between the ideal and the reality in classifying injury deaths among the four participating countries. In Sweden, about one-third of all injury deaths and in Australia, Taiwan and the USA, about one in 10 injury deaths were coded to X59. Falls and drownings were the two most common events for which sufficient specificity was often not provided. Ironically, falls and drownings are two of the code groups for which there is an increase in level of detail in ICD-10 compared with ICD-9.6 In the following sections, we propose some explanations for the relatively high prevalence of unspecified injury codes, explore the variations across countries and discuss their implications for international comparisons.
Unspecified external factors
The relatively high percentage (33%) of deaths in Sweden coded to X59 is particularly problematic when comparing data between countries. Most of these were ⩾65 years and involved femoral fractures. In the ICD-9 era, this was less a problem because these deaths could be coded to ICD-9 code E887 (fracture due to unspecified cause) which has been tabulated within the fall block (E880–E888). It was logical to assume that these deaths involved a fall even though a fall was not explicitly specified. However, there is no comparable ICD-10 code; all of these deaths were coded in ICD-10 to X59, which is not specific as to a fracture. This has been recognized as a problem and from the 2006 ICD-10 updates (implementation in the USA will be in January 2007) a fourth character subdivision has been introduced for the ICD-10 code X59. The new code is X59.0 (exposure to unspecified factor causing fracture).
Unspecified falls
Most of the people who died from falls were those aged ⩾65 years. The overall proportion of unspecified falls was 71% (447/634) in Australia, 80% (435/543) in Sweden and 77% (11 637/15 055) in the US. Our findings also revealed that the proportion of unspecified falls increased with age, with percentages in the ⩾65 age group of 69% in Australia, 67% in Sweden, 71% in Taiwan and 56% in the USA (table 3). It is sometimes difficult to get precise information about the circumstances for these falls in the elderly people.
For example, an elderly person who lives alone and falls in the home is found dead 2 days later. The certifier might find it difficult to attribute this fall to slipping (ICD-10 code W01), or a fall involving bed (ICD-10 code W06), chair (ICD-10 code W07), or other furniture (ICD-10 code W08). In the case of an elderly person who falls in a nursing home while being carried or supported by a healthcare worker (ICD-10 code W04) which at the same time, involves a wheelchair (ICD-10 code W05) and bed (ICD-10 code W06), it may also be difficult to disentangle the main cause of the fall.
Other unspecified injury codes
Despite the relatively low percentage of unspecified events of undetermined intent in each country, we still found large variation across countries. A recent American study indicated great variations across states in the number of deaths classified as undetermined intent.11 A Taiwanese study pointed out that in some cities and counties a high number of deaths classified as due to undetermined intent occured owing to small number of certifiers with biased behavior in reporting manner of death.12 However, these studies did not examine why the certifiers did not report mechanisms or means (eg, poisoning, hanging, drowning, handgun, falls, jumping and so on). Differences in reporting intent may also be due to some countries interpreting the ICD rules to mean that a death cannot be coded to undetermined intent unless a legal official or coroner conducts a full investigation of the death and is not able to make a determination regarding the intent.
For transport accidents, Australia and Sweden had a very low percentage of use of unspecified codes (ICD-10 code V89 and V99). On the contrary, Taiwan had a quite high percentage of use of these non-specific codes. Possible reasons for the variations across countries may be related to the differences in the extent of querying undertaken when death certificates are incomplete and different measures taken to collect additional information about the circumstances of deaths between the study countries.
Querying the unspecified death certificates
In Taiwan, coders routinely query unspecified deaths for decedents aged ⩽49 years. Most of the time, coders do not query unnatural deaths certified by coroners or medical examiners. In the USA, standards for querying establish that unspecified external causes should always be queried (priority level 1e in the query manual),13 but practice varies widely from state to state. Some states query in most high priority situations. Some do not query at all. The others fall somewhere in between.
In Australia, coders query for additional information if there is not sufficient detail on the death certificate to assign a specific and useful underlying cause. However, the degree to which such queries return positive results depends on factors such as the availability and goodwill of the original certifier. There are no rigid rules for the number of queries sent per year. Generally, death certificates for decedents aged >85 years are not queried.
In Sweden, coders routinely query injury deaths without stated external causes for deaths of people aged ⩽80 years. Coders also query deaths where the description of the external event does not allow the coder to assign a specific three-character code. The exception is hip fractures in the elderly people. Because many of these accidents take place at the patient’s home and the physicians seldom know the exact circumstances, the coders seldom query hip fractures and code them to ICD-10 code X59.0.
Gathering more information
One of the reasons for the relatively low percentage of unspecified external cause codes in Australia is that the coders can use the National Coroners Information System (NCIS) to obtain further information about an external cause death. The NCIS is a national internet-based data storage and retrieval system for Australian coroner’s cases. Information about every death reported to an Australian coroner since July 2000 is stored within the system, which includes information such as toxicology results, police reports, autopsy results and so on and the final coronial finding relating to the manner and cause of death. Coders in the causes of death unit at the Australian Bureau of Statistics can access this information to obtain details to enable use of a more specified code.14
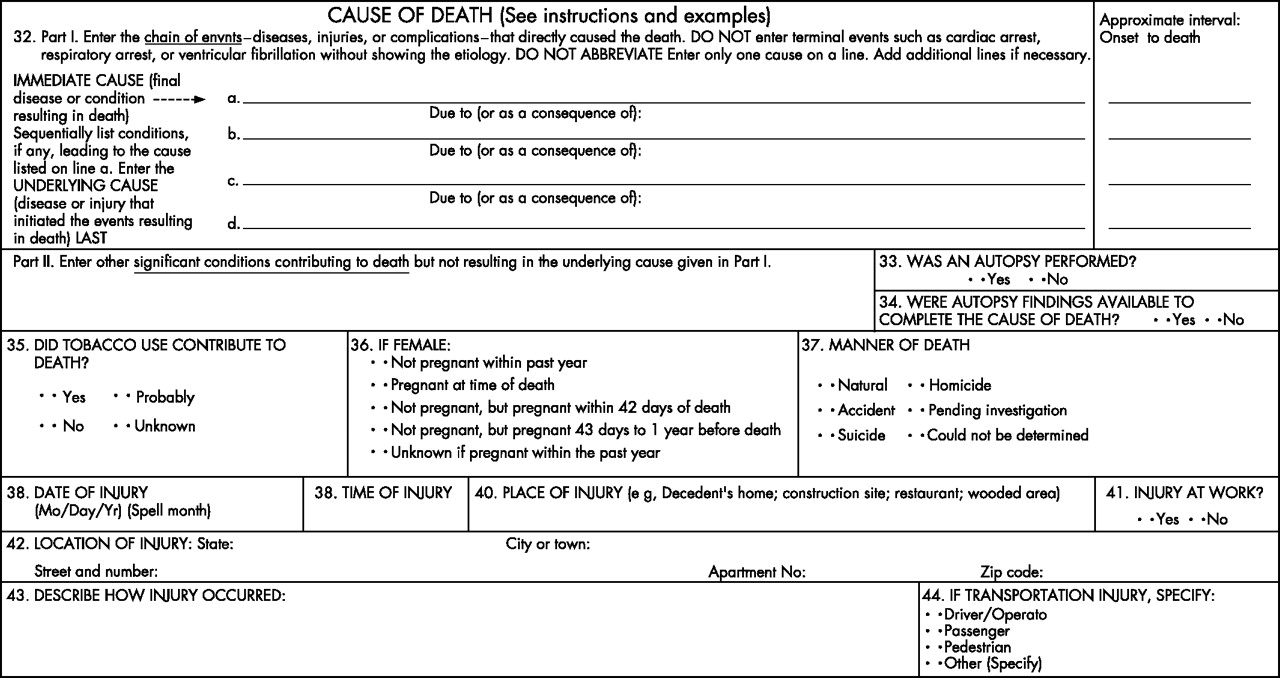
To get more information about the circumstances of injury, some items have been added to the USA standard certificate of death over the years (fig 1). Date of injury, time of injury, place of injury, whether injury occurred at work, location of injury and a description of how the injury occurred have been in place since at least 1949. Most recently, an item detailing the road user type for transportation injuries was added in 2003. These items provide coders with useful information for more specific external cause coding.
{kind=link}
Items 38–44 on the US standard certificate of death are designed to get more specific information on circumstances of injury (this represents the most recent revision of the standard certificate of death implemented in 2003).
In Sweden, six extra items have been added to the death certificate for gathering more specific information related to the external cause of death: (1) the means of establishment of the causes of death—that is, clinical autopsy, examination before death, external inspection of the body, forensic autopsy and forensic external inspection; (2) whether there was an operation within the four weeks prior to death; (3) if the deceased had any kind of addiction and the specific type of drug/drugs: alcohol, medicine, narcotics, other; (4) in the case of injury deaths, the reason or cause and if any, the intent; (5) a short description of how the external cause arose; and (6) where the incident occurred: at home, school or other public place, sports arena, road, industry, other/not known.
Some studies suggest that another possible route for collection of additional details is through record linkage of death certificate data with other data such as hospital discharge data15–17 or police traffic accidents data18,19 to get more information on circumstances. However, each of these studies reports issues relating to the under-reporting of injury-related deaths in the current mortality statistics system, which is beyond the scope of this study, such as legal and ethical concerns relating to the ability to link disparate datasets.
Implications for international comparisons
Comparability of injury mortality data between countries may be affected by differences in the specificity of codes assigned. For example, if certifiers in country A are more likely to mention falls for deaths in elderly people with fractures, these deaths would be coded in the ICD-10 block W00–W19. On the contrary, if certifiers in country B are less likely to explicitly mention falls in the same situations, these deaths would be assigned to ICD-10 code X59. The international comparability of mortality rates due to falls will be influenced by these differences in certification behaviors. The high percentage of unspecified injuries in Taiwanese data also seriously compromises detailed international comparisons of mortality from transport injuries, drownings and deaths associated with fire and flames.
Although coder error might lead to a potential bias in our results, we believe that this bias is unlikely to happen, because previous studies have reported that coder error is least likely to happen due to external causes.20,21
Key points
-
If the certifier does not report sufficiently detailed information for an injury death, an unspecified external cause of death will be coded, which provides little useful information for injury prevention.
-
In this study, Sweden (33%) had the highest proportion of use of unspecified code (International Statistical Classification of Diseases and Related Health Problems, Tenth Revision, ICD-10 code X59), followed by Australia (17%), Taiwan (13%) and the USA (7%).
-
Most of the deceased with ICD-10 code X59 were those aged ⩾65.
-
The percentage of unspecified codes within specific groups of external causes was relatively high for deaths due to falls and unintentional drowning.
-
Researchers should be cautious when making international comparisons and efforts are needed to educate certifiers to report sufficient information for specific coding.
More effort is needed to educate certifiers to report sufficient information for coders to classify injury deaths more specifically. Currently, there are no explicit instructions on the international form of medical certificate of cause of death recommended by the World Health Organization to prompt the certifier for information related to the external cause. Certifiers may not be aware of the importance of complete documentation of such causal information, particularly for deaths in elderly people where other comorbidities are also likely to have contributed to or been associated with death. To improve the quality of statistical data relating to the external cause of injuries leading to or associated with death, certifiers need to be made aware of the importance of documenting all information pertaining to the cause of the injury. This awareness raising may happen through either through education or the query action processes. Creating a system like the NCIS in Australia is another alternative to improve the usefulness of external cause mortality data for injury prevention.
In conclusion, a large gap exists between the “ideal” and the “reality” in reporting injury deaths, especially deaths from falls and drowning. In addition, these gaps vary from country to country and have important implications for the comparability of injury mortality data between countries and for injury prevention initiatives. Therefore, researchers should be cautious when making international comparisons of such data.
Acknowledgments
We appreciate the assistance of Mr Pei-Yuen Hsu in the analysis of the data. This study was supported by a grant from The National Science Council (NSC-95-2314-B-006-093).
REFERENCES
Footnotes
-
Competing interests: None declared.