Article Text

Abstract
Objective: To assess whether area-wide traffic calming schemes can reduce road crash related deaths and injuries.
Design: Systematic review and meta-analysis.
Data sources: Cochrane Injuries Group Specialised Register, Cochrane Central Register of Controlled Trials, Medline, EMBASE, Sociological Abstracts Science (and social science) citation index, National Technical Information service, Psychlit, Transport Research Information Service, International Road Research Documentation, and Transdoc, and web sites of road safety organisation were searched; experts were contacted, conference proceedings were handsearched, and relevant reference lists were checked.
Inclusion criteria: Randomised controlled trials, and controlled before/after studies of area-wide traffic calming schemes designed to discourage and slow down through traffic on residential roads.
Methods: Data were collected on road user deaths, injuries, and traffic crashes. For each study rate ratios were calculated, the ratio of event rates before and after intervention in the traffic calmed area divided by the corresponding ratio of event rates in the control area, which were pooled to give an overall estimate using a random effects model.
Findings: Sixteen controlled before/after studies met our inclusion criteria. Eight studies reported the number of road user deaths: pooled rate ratio 0.63 (95% confidence interval (CI) 0.14 to 2.59). Sixteen studies reported the number of injuries (fatal and non-fatal): pooled rate ratio 0.89 (95% CI 0.80 to 1.00). All studies were in high income countries.
Conclusion: Area-wide traffic calming in towns and cities has the potential to reduce road traffic injuries. However, further rigorous evaluations of this intervention are needed, especially in low and middle income countries.
- systematic review
- traffic calming
- road safety
Statistics from Altmetric.com
The worldwide epidemic of road traffic injuries is only just beginning. At present, over a million people die each year and some 10 million people sustain permanent disabilities in road traffic crashes. For people under 44 years, road traffic crashes are a leading cause of death and disablement, second only to HIV and AIDS.1 Many developing countries are still at comparatively low levels of motorisation and the incidence of road traffic injuries in these countries is likely to increase. It is estimated that by 2020 road traffic crashes will have moved from ninth to third in the world disease burden ranking, as measured in disability adjusted life years.2
Most of the road deaths in developing countries involve vulnerable road users such as pedestrians and cyclists. In Ethiopia, pedestrian injuries account for 84% of all road traffic fatalities compared with 32% in Britain and 15% in the USA.3 In the heavily motorised countries drivers and passengers account for the majority of road deaths but pedestrians account for a large proportion of road deaths involving children. The identification of effective strategies for the prevention of road traffic injuries is of global health importance.
In urban areas, road traffic crashes are scattered widely, and in such situations localised interventions for high risk sites are not appropriate. In high income countries area-wide traffic calming schemes, including the treatment of both main roads and residential roads, have been proposed as a strategy for reducing such scattered crashes. Traffic calming has been defined as the combination of mainly physical measures that reduce the negative effects of motor vehicle use, alter driver behaviour, and improve conditions for non-motorised street users.4 It has been estimated that area-wide traffic calming schemes can reduce the number of road traffic injuries by about 15%.5 However, this estimate was based on a review that included uncontrolled before/after studies in which the effect of traffic calming could be confounded by other factors that influence road traffic injury rates. In particular, in high income countries there is evidence that pedestrian injury rates have fallen because of a reduction in walking.6 In this case, the inclusion of uncontrolled studies could exaggerate the apparent effect of traffic calming. We conducted a systematic review of controlled studies to assess the effect of area-wide traffic calming on road user deaths, injuries (fatal and non-fatal), and numbers of road traffic crashes.
METHODS
Inclusion criteria
We included randomised controlled trials and controlled before/after studies of area-wide traffic calming schemes. Eligible schemes included those that involved a number of specific changes to the road layout, road hierarchy or road environment, for example road narrowing, road closures, creation of one way streets, changes at junctions, mini-roundabouts, road surface treatment, or speed humps. We excluded studies describing the enforcement of legal interventions, financial incentives or disincentives, and interventions investigating alteration to road signage or traffic lights alone, or studies solely describing interventions to separate different road users (cycle lanes, bus lanes, pedestrian walkways). The outcomes of interest were all road user deaths, all road user injuries (fatal and non-fatal), and the number of traffic crashes.
Identification of studies
We searched the following electronic databases; Cochrane Injuries Group Specialized Register, Cochrane Central Register of Controlled Trials, Medline, EMBASE, Sociological Abstracts Science (and Social Science) Citation Index, National Technical Information Service, Psychlit, Transport Research Information Service, International Road Research Documentation, and TRANSDOC (the last three combined in the TRANSPORT database). One reviewer examined titles, abstracts, and keywords of citations, as given on electronic databases, for eligibility. Where possible the full text of all of potentially relevant citations was obtained. We also searched the web sites of road safety organisations, contacted experts, hand searched conference proceedings, and checked reference lists of relevant papers. There were no language restrictions. Further details of the search strategy can be seen in box 1.
Box 1: Strategy for identification of studies
Search strategy for electronic databases; searches run in 2000
-
Terms describing the intervention, outcomes, and study methodology were combined.
-
A: the intervention—area traffic control* or TRAFFIC RESTRAINT* or traffic calming or traffic engineering or road design or road layout or roundabout* or humps or bumps or traffic distribution or traffic redistribution or traffic flow or crosswalk* or speed cushion* or chicane* or road narrowing or refuges or road hierarchy or traffic hierarchy or four way* stop* or access only or sheltered parking or left turn lane* or wooner* or junction layout or road layout or lateral clearance.
-
B: the outcome—accident* or injur* or fatalit* or death or safety.
-
C: the study methodology—evaluation or assess* or stud* or evaluation or assess* or (controlled near2 stud*) or comparison or comparative or intervention near2 stud* or controls.
Web sites searched; searches conducted in 2001
-
AAA Foundation for Traffic Safety (USA): www.aaafoundation.org
-
ARRB, Australian Road Research Board: www.arrb.org.au
-
Australian Transport Safety Bureau: www.atsb.gov.au
-
CROW, Information and Technology Centres for Transport and Infrastructure (Netherlands): www.crow.nl
-
Danish Council for Road Safety Research: www.trm.dk/eng/veje/rft
-
Danish Transport Research Institute: www.dtf.dk
-
DVR, Deutscher Verkenrssichereitsrat Road Safety Institute (Germany): www.dvr.de/
-
FINNRA, Finnish National Road administration: www.tieh.fi
-
INRETS, Institut National de Recherche sur les Transports et leur Sécurité (France): www.inrets.fr
-
ITE, Institute of Transportation Engineers (USA): www.ite.org
-
LET, Laboratoire d’economie des transports (France): www.lsh-lyon.cnrs.fr
-
NHTSA, National Highway Traffic Safety Administration (USA): www.nhtsa.dot.gov
-
Swedish National Roads Administration: www.vv.se/for_lang/english/
-
SWOV, Institute for Road Safety Research (Netherlands): www.swov.nl
-
TOI, Institute of Transport Economics (Norway): www.toi.no
-
TC, Transport Canada: www.tc.gov
-
TRB, Transportation Research Board: www.nas.edu/trb/
-
TRL, Transport Research Laboratory (UK): www.trl.co.uk
-
US Department of Transport, Federal Highway Administration (USA): www.fhwa.dot.gov
-
VTI, Swedish National Road and Transport Research Institute: www.vti.se
-
VTT, Finland www.vtt.fi/indexe.htm
Conference proceedings handsearched
-
Australian Road Research Board (ARRB). Proceedings of the 12th ARRB conference; Hobart, Tasmania 27–31 August 1984.
-
Australian Road Research Board (ARRB). Proceedings of the 15th ARRB conference; Darwin 26–31 August 1990.
-
Institution of Professional Engineers New Zealand (IPENZ). Annual conference, Christchurch February 1992 volumes 1 and 2.
-
Institution of Professional Engineers New Zealand (IPENZ). Proceedings of the technical session of the group at the annual conference of IPENZ; Auckland 8–12 February 1982.
-
Institute of Transportation Engineers (ITE). Proceedings of the 45th to 71st ITE annual meeting, 1975–2001.
-
Institute of Transportation Engineers (ITE). Transportation and traffic theory 9th international symposium; Netherlands 1984.
-
Institute of Transportation Engineers (ITE). Residential street design and traffic control 1989.
-
Israel Institute of Technology. International conference on pedestrian safety; Haifa 20–23 December 1976.
-
Landor Publishing Ltd. The third national traffic calming conference; London 18 October 1996.
-
Organisation for Economic Co-operation and Development (OECD). Proceedings of the symposium on techniques of improving urban conditions by restraint of road traffic; 25–27 October 1971.
-
PTRC Transport, Highways and Planning Summer 13th–18th Annual Meetings, 1985–90.
-
Swedish Road and Traffic Research Institute. Proceedings of the conference on strategic highway research program and traffic safety on two continents; Gothenburg, Sweden 18–20 September 1991.
-
Swedish Road and Traffic Research Institute. Proceedings of the conference on strategic highway research program and traffic safety on two continents; Gothenburg, Sweden 27–29 September 1989.
-
Swedish Road and Traffic Research Institute. Proceedings of the conference on road safety and traffic environment in Europe; Gothenburg, Sweden 26–28 September 1990.
-
The Technion Israel Institute of Technology. The second international conference on new ways for improved road safety and quality of life; Tel-Aviv Hilton Hotel, Israel 7–10 October 1991.
-
Transportation Research Institute. International conference on new ways and means for improved safety; Tel Aviv, Israel 20–23 February 1989.
-
Transport Research Laboratory. Safety 91 Papers on vehicle safety, traffic safety and road user safety research; TRL Laboratory, Berks 1–2 May 1991.
Data extraction and analysis
One reviewer decided whether studies met the inclusion criteria, and this was checked by a second reviewer. Using a data collection form two reviewers independently extracted data on road user deaths, injuries (fatal and non-fatal), traffic crashes, characteristics of the intervention and control area, and types of measures implemented. To assess study quality we collected information on how the intervention and control areas were matched, duration of the before and after periods, and, because of the potential for contamination, we also noted the proximity of the intervention and control areas.
For each study we calculated a rate ratio: the ratio of event rates before and after intervention in the traffic calmed area divided by the corresponding ratio of event rates in the control area. This gives the reduction in the incident rate in the intervention area compared to that in the control area. For example, a rate ratio of 0.8 corresponds to a 20% reduction in events compared with that predicted from the rates in the control area. For the calculation of 95% confidence intervals, standard errors of the logarithms of the rate ratios were constructed assuming that the number of events in each area in each period followed a Poisson distribution,7 provided there was at least one event in each period. For studies with no events in one or more periods exact confidence intervals were calculated where the rate ratio was defined. Rate ratios were combined on a logarithmic scale using a random effects meta-analysis model. The assumption of random effects means that the effect estimates and confidence intervals allow for variation in study specific rate ratios over and above that due to variability within studies.8 In this meta-analysis such additional variability reflects both underlying heterogeneity in rate ratios across studies and any variability arising through overdispersion9 if the assumption that events follow Poisson distributions is violated.
For studies with no events in one or more periods 1/2 was added to all counts in the pooled analysis. In the analysis of road user deaths, where the majority of studies had no events in at least one period, no test of heterogeneity was carried out, and a pooled estimate of the rate ratio was obtained from the column totals. Analyses were carried out in Stata version 7.0 (Stata corporation, College Station, Texas 77845, USA).
RESULTS
The searches identified 12 986 published and unpublished reports which were screened for eligibility. We obtained the full text of 586 reports and of these 12 reports, describing 16 controlled before/after studies, met our inclusion criteria (see table 1).10–21 We found no randomised controlled trials. Seven studies were done in Germany,10–12,16 six in the UK,13,17–21 two in Australia,14 and one in the Netherlands15; all were done in the 1970s and 1980s. In most studies attempts had been made to match the intervention and control sites. However, in three differences in the land use characteristics or type of district are reported,14,15 and in one the control area was much larger than the intervention area.15 Outcome data was collected from police or local authority records in all studies.
Table of included studies
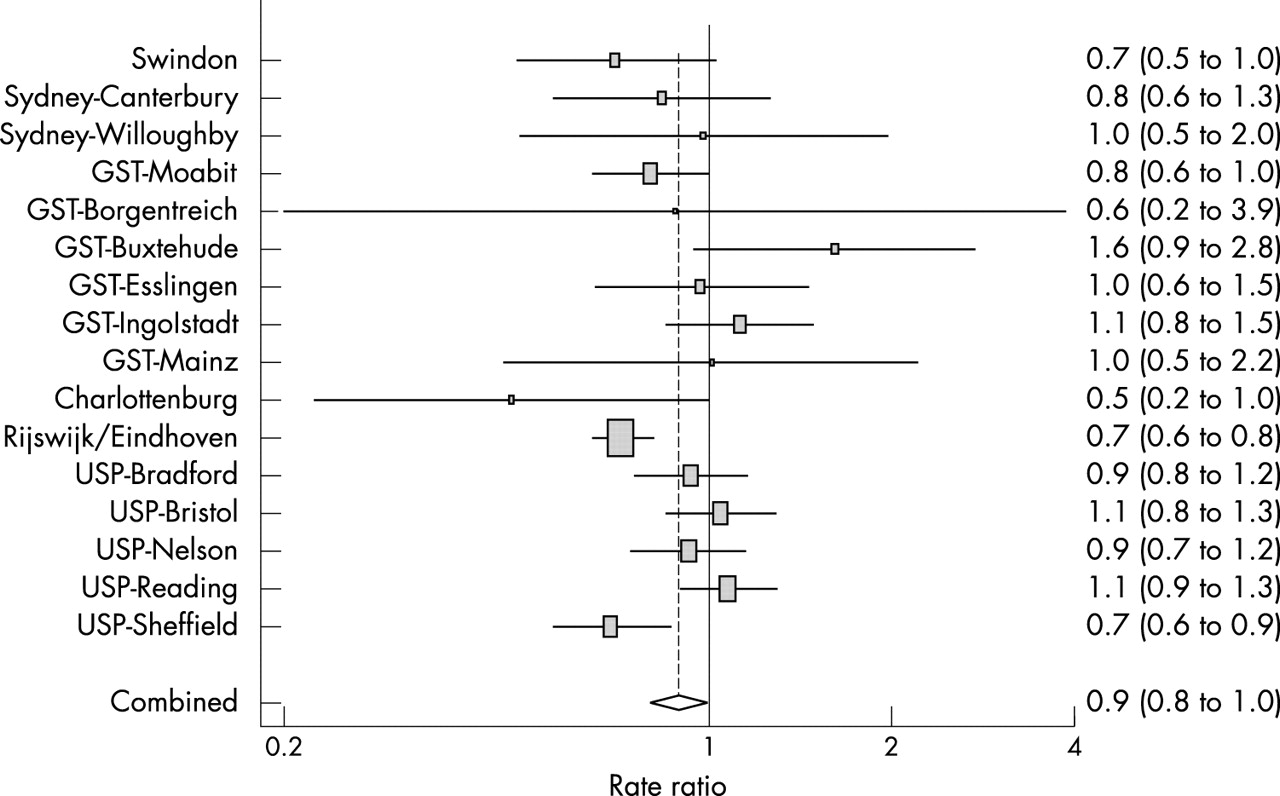
Eight studies reported the number of road user deaths.10,14 The pooled rate ratio was 0.63 (95% confidence interval (CI) 0.14 to 2.59). This result should be interpreted with caution since many of the studies include at least one period in which no road user deaths were observed. Sixteen studies reported the number of road traffic injuries (fatal and non-fatal).10–21 The pooled rate ratio was 0.89 (95% CI 0.80 to 1.00) (fig 1), with statistically significant heterogeneity between the studies (p = 0.05). Nine studies reported the total number of road traffic crashes.10,19,20 The pooled rate ratio was 0.95 (95% CI 0.81 to 1.11) (fig 2), again with statistically significant heterogeneity between the studies (p = 0.001). Thirteen trials reported the number of pedestrian crashes.10,14,17–21 The pooled rate ratio was 1.00 (95% CI 0.84 to 1.18) There was no significant heterogeneity (p = 0.21).

Number of road traffic injuries (fatal and non-fatal).

{kind=link}
{kind=link}
Number of road traffic crashes.
DISCUSSION
This systematic review of controlled before/after studies shows that area-wide traffic calming has the potential to prevent road traffic injuries. Although the effect of traffic calming on road user deaths is in the same direction as for injuries (fatal and non-fatal), because the number of road user deaths in the included studies is low the estimated rate ratio is imprecise. Indeed, the imprecision in the rate ratio may be understated by the confidence interval because the way that the confidence interval was calculated ignores the likely heterogeneity between studies. Although we found no reliable evidence that traffic calming reduces the number of road traffic crashes, because traffic calming may reduce vehicle speeds,22 this is not inconsistent with a reduction in the occurrence of injury. Our estimates of the effectiveness of traffic calming provide a basis for future cost effectiveness analyses that would be important in informing decisions about resource allocation.
Several methodological issues may have a bearing on the validity of these results. Publication and other selection biases are a potential threat to validity in all systematic reviews, but this is a particular problem in road safety where a large proportion of the available research is published in the grey literature. In this review only two of the included studies were published in journals. There are also problems identifying published controlled studies in the road safety databases.23 Search strategies for identifying controlled studies in medical databases can achieve high sensitivity because terms describing the study methodology are included among the indexing (descriptor) terms. Road safety databases, however, have a very limited range of indexing terms describing the study methodology. Despite our considerable efforts to identity all eligible studies, published and unpublished, irrespective of language of publication, we cannot exclude the possibility that some studies were missed resulting in reduced precision and the potential for bias.
Key points
-
Injuries as a result of road traffic crashes are a global problem and are likely to increase.
-
A previous meta-analysis, including uncontrolled before after studies, found area-wide traffic calming can reduce road traffic injuries by about 15%.
-
This systematic review, of 16 controlled before after studies, found an 11% reduction in road traffic injuries (fatal and non-fatal).
-
Traffic calming has the potential to prevent road traffic injuries but further rigorous evaluations, particularly in low and middle income countries, is required.
Although we found no randomised controlled trials of traffic calming schemes, the inclusion of studies with well matched intervention and control areas, with adequate before and after periods, may avoid the problem of confounding by changes in the background rate of injury. All but one15 of the included studies had attempted to match the intervention and control areas and all had collected at least two years before and two years after data, with a number collecting up to five years before or after data.
Because there was significant heterogeneity between the studies reporting the number of road traffic injuries and crashes, these results should be interpreted with caution. The observed heterogeneity may be due to differences in study design, in the types of traffic calming schemes involved, or in the way outcomes were defined and data collected.
The included studies were all conducted in the 1970s and 1980s, and, apart from two Australian studies, were all done in Europe. As a result it may make it more difficult to generalise from this systematic review and make inferences about the effectiveness of present day area-wide traffic calming schemes. In addition road traffic crashes are a major cause of death and injury in low and middle income countries where most of the casualties are pedestrians, cyclists, and riders of motorised two wheelers. Although traffic calming appears to be a promising intervention for preventing road traffic injuries because none of the included studies were conducted in low and middle income countries further rigorous evaluation is required in these settings.
Acknowledgments
We thank the Medical Research Council for funding to undertake this review.