Article Text

Abstract
Background: Injuries resulting in admission to hospital provide an important basis for determining priorities, emerging issues, and trends in injury. There are, however, a number of important issues to be considered in estimating person based injury incidence using such data. Failure to consider these could result in significant overestimates of incidence and incorrect conclusions about trends.
Aim: To demonstrate the degree to which estimates of the incidence of person based injury requiring hospital inpatient treatment vary depending on how one operationally defines an injury, and whether or not day patients, readmissions, and injury due to medical procedures are included.
Method: The source of data for this study was New Zealand’s National Minimum Dataset. The primary analyses were of a dataset of all 1989–98 discharges from public hospital who had an external cause of injury and poisoning code assigned to them.
Results: The results show that estimates of the incidence of person based injury vary significantly depending on how one operationally defines an injury, and whether day patients, readmissions, and injury due to medical procedures are included. Moreover the effects vary significantly by pathology and over time.
Conclusions: (1) Those using New Zealand hospital discharge data for determining the incidence of injury should: (a) select cases which meet the following criteria: principal diagnosis injury only cases, patients with day stay of one day or more, and first admissions only, (b) note in their reporting that the measure is an estimate and could be as high as a 3% overestimate. (2) Other countries with similar data should investigate the merit of adopting a similar approach. (3) That the International Collaborative Effort on Injury Statistics review all diagnoses within International Classification of Diseases 9th and 10th revisions with a view to reaching consensus on an operational definition of an injury.
- hospital discharge data
- medical injuries
- injury incidence
- readmissions
- NHI, National Health Index
- NMDS, National Minimum Dataset
- NZHIS, New Zealand Health Information Service
- hospital discharge data
- medical injuries
- injury incidence
- readmissions
- NHI, National Health Index
- NMDS, National Minimum Dataset
- NZHIS, New Zealand Health Information Service
Statistics from Altmetric.com
- hospital discharge data
- medical injuries
- injury incidence
- readmissions
- NHI, National Health Index
- NMDS, National Minimum Dataset
- NZHIS, New Zealand Health Information Service
- hospital discharge data
- medical injuries
- injury incidence
- readmissions
- NHI, National Health Index
- NMDS, National Minimum Dataset
- NZHIS, New Zealand Health Information Service
As injury and its prevention receives increasing recognition worldwide as a public health problem, the demand for quality data to determine priorities, emerging issues, and trends has increased. For non-fatal injury, those events which result in inpatient hospital treatment have an important part to play in this respect since many of them are serious, both in terms of threat to life and long term disablement, and, as a consequence, incur substantial cost. New Zealand is in the fortunate position of having had published records of injury cases for all public hospital discharges since 1955 and electronic versions of the data since 1974. These data have been used extensively by the Injury Prevention Research Unit in producing research aimed at facilitating injury prevention in New Zealand.1 This experience has alerted us to a number of important issues that users of similar data should be aware of in estimating person based injury incidence. As we will show here, these issues may have a dramatic effect on estimates of incidence and conclusions about trends.
The aim of this paper is to demonstrate the degree to which estimates of the incidence of person based injury requiring hospital inpatient treatment vary depending on how one operationally defines an injury, and whether or not day patients, readmissions, and injury due to medical procedures are included.
METHODS
The source of data for this study is New Zealand’s National Minimum Dataset (NMDS) which is maintained by New Zealand Health Information Service (NZHIS). This is a single integrated collection of secondary and tertiary health data, developed in consultation with health sector representatives, required at national level for policy formulation, monitoring and evaluation of policy implementation, performance monitoring and evaluation, health status measurement, and meeting international requirements.
Information about all day patients and inpatients discharged from public hospitals is supplied directly to the NMDS by hospital based computer systems. The data collected include information on diagnoses, diagnostic and therapeutic procedures, as well as demographic information about the patient/healthcare user (for example, ethnicity, age, sex, domicile). All discharges with an injury and poisoning diagnosis have the circumstances of injury coded according to the external causes of injury and poisoning codes (E codes) and the nature of injury according to International Classification of Diseases2 or derivatives of it (for example, ICD-9-CM and ICD-9-CM-A).
In 1992 the vast majority of persons injured and requiring acute inpatient treatment were admitted to public hospitals.1 While the private sector has played an increasing part in the delivery of inpatient health services in recent years, the most recent publication of statistics from NZHIS suggests service delivery for the acute management of injury requiring inpatient treatment has remained unchanged.3 Since private hospitals do not consistently E code discharges we have confined our analyses to public hospital discharges.
Readmission status has been determined using four data elements available in the NMDS from 1989. These data elements were: a unique personal identifier (National Health Index (NHI) number), date of injury, date of admission, and date of discharge. It has been shown previously that reasonably accurate estimates of readmission status can be derived by coding all cases with the same NHI number and date of injury as a case with an earlier date of admission as readmissions.4 Nevertheless, to allow for incorrect and missing dates of injury, where two cases are identified with the same NHI number and one case has a date of admission within one day of the date of discharge of the other case, the former case was coded as a readmission.
Since these analyses are concerned with non-fatal injury all persons who were discharged dead have been excluded.
The theoretical definition of injury is problematic since there is no scientific basis for a distinction between disease and injury. Traditionally, however, the term has been used to refer to damage to the body produced by energy exchanges that have relatively sudden discernible effects. Damage due to some chronic low energy exposures (for example, carpal tunnel syndrome) are also included by some in their definition of injury.5
One commonly used operational definition of injury is all those pathologies included in the injury and poisoning chapter (XVII) of the International Classification of Diseases.2 That is the definition which was used here. However, sometimes official published statistics use the supplementary classification of external causes of injury and poisoning (E codes) to select cases.6
The introduction to the E codes chapter states that the classification is provided for the purposes of “…the classification of environmental events, circumstances and conditions as the cause of injury, poisoning and other adverse events” (p 547).2 The introduction, however, also states: “Where a code from this section is applicable, it is intended that it shall be used in addition to a code from one of the main chapters of the International Classification of Diseases, Injuries and Causes of Death, indicating the nature of the condition. Most often, the nature of the condition will be classifiable to chapter XVII, Injury, Poisoning and Violence…..”.
In New Zealand the latter provision is applied and, as a consequence, there are more cases with external cause code than have a principal diagnosis of injury. Other countries we have identified who adopt a similar practice are Australia (J Harrison, personal communication), Canada (E Mackenzie, personal communication), England and Wales (C Sweeting, personal communication), and the USA (H Weiss, personal communication). We thus commence our analyses by examining the effect of selecting cases solely on E codes.
Annual population estimates, were obtained from Statistics New Zealand for the purposes of calculating rates. Where noted, rates have been age adjusted using the direct method.
RESULTS
Case selection based on external cause rather than diagnosis
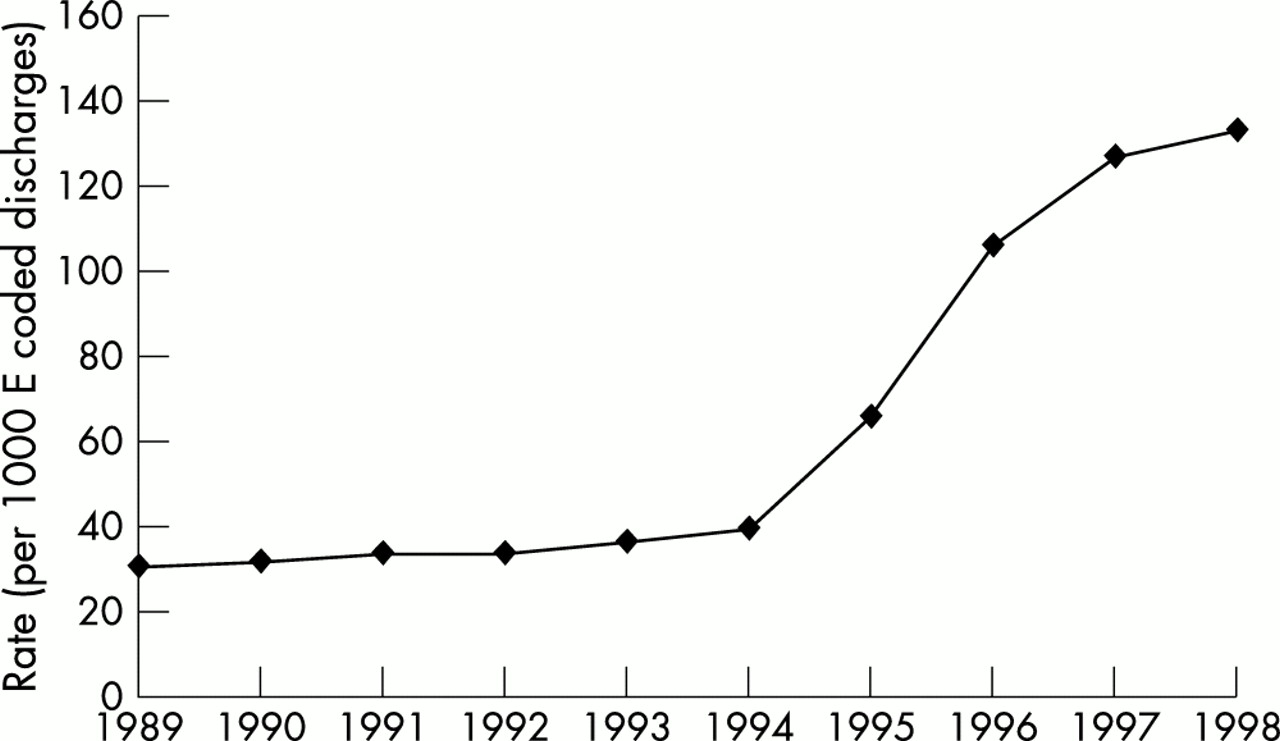
The distribution of E coded New Zealand discharges by principal diagnosis is given in table 1. The table shows that non-injury principal diagnoses account for 36% (n=38 434) of all E coded discharges. Of these, 41% (n=15 735) did not have an injury diagnosis as a secondary or subsequent diagnosis. The vast majority (80%) of the 15 735 cases had E codes identifying iatrogenic factors as the cause (for example, adverse effects of drugs). Figure 1 shows the utilisation rate of E codes for non-injury cases increased substantially after 1994.
All discharges with external cause code: principal diagnosis distribution, 1998

Trend in rate (age adjusted) of non-injury discharges with an E code, 1989–98.
Principal diagnosis only as the basis for case selection of injury cases
Several countries, including New Zealand, make provision for the recording of multiple diagnoses. Thus there would be discharges which have a disease as a principal diagnosis but other diagnoses as injury (for example, heart attack, fracture of the lower limb). It could be argued that injury cases should be selected on the basis of any diagnostic field having an injury code. This approach is problematic for at least two reasons. First, in many cases where the injury diagnosis appears in the second or subsequent diagnosis fields it would be difficult to determine if the person would have been “admitted” to hospital if they had only the injury. Secondly, as countries place increasing emphasis on the costs of health delivery and the recovery of those costs, the utilisation of multiple diagnostic codes is likely to increase over time. This is well illustrated in the New Zealand context.
Figure 2 shows that up until 1994 if one selected injury cases on the basis that they had a injury diagnosis recorded in any diagnostic field it would have minimal impact on the estimate of incidence of injury. Thereafter, however, the increasing use of the second and subsequent diagnostic fields would have a significant and unstable effect on the incidence estimate.

Trends in rates (age adjusted) of injury discharges by diagnostic order, 1989–98.
Given the foregoing the remainder of the results below are only for those cases where the principal diagnosis was an injury.
Day patients
Patients whose stay in hospital was less than a day have been described by NZHIS as day patients. Table 2 shows the distribution of E coded discharges by day patients and inpatients (that is, day stay >0) for 1998. Overall day patients accounted for 18% of the discharges. The effect of excluding day patients varies according to the E code grouping. At one extreme, submersion/suffocation/foreign bodies (E960–E969), 39% of discharges were day patients, and at the other extreme the comparable figure for “air space and transport accidents” (E840–E848) was 4%. Figure 3 shows that the number of day patients per 1000 injury discharges increased steadily from 1989 through to 1993. Thereafter the rates have been relatively stable at about 169 cases per 1000 injury discharges.
Distributon of E code group by day patients and inpatients for discharges with principal diagnosis of injury, 1998

Trends in rates (age adjusted) of injury discharges with various attributes, 1989–98.
Readmissions
Given that people can be admitted to hospital for the treatment of injury in both the acute and rehabilitative phases, it is important to be able to differentiate the two. Failure to do so could produce a substantial error in the estimate of person based injury incidence if the dataset being examined has individuals in it who have a series of readmissions for ongoing treatment and or rehabilitation (for example, skin grafts after thermal injury).
Table 3 shows the distribution of E code by readmission status for 1998. Overall 9% of all discharges E coded were readmissions. The largest contributor (45%) to this effect was “surgical and medical procedures as the cause of abnormal reaction of patients or later complication, without mention of misadventure at the time of procedure” (E878-E879). Late effects of accidental injury (E929) had the highest percentage (51%) of readmissions. Figure 3 shows the readmission rate had declined substantially since 1993.
Distributon of E code group by readmission status for discharges with principal diagnosis of injury, 1998
Injury due to medical procedures
Injury due to: “misadventures to patients during surgical and medical care” (E870–E876), “surgical and medical procedures as the cause of abnormal reaction of patients or later complication, without mention of misadventure at the time of procedure” (E878–E879), and “drugs, medicaments and biological substances causing adverse effects in therapeutic use” (E930–E949), traditionally have not been considered the domain of injury prevention.7 Combined (n=11 899) these E code groupings account for 18% of all patients with a principal diagnosis of injury (table 2). Clearly the inclusion or exclusion of these events has significant implications for the estimate of the incidence of injury. Moreover, as fig 3 shows, the rate of these cases have been increasing over time.
An examination of the injury diagnoses for these three groups reveals that 93% have a diagnosis in the grouping: 996–999: “complications of surgical and medical care not elsewhere classified”.
Combined effects
So far we have considered day patients, readmissions, and injuries due to medical procedures independently of one another. Table 4 shows the combined effect of selecting first admissions only and excluding day cases and injuries due to medical procedures (fully restrictive). Overall the estimate of the incidence of injury for 1998 is 37% less than it would be if case selection was based solely on whether a discharge had a principal diagnosis of injury. Table 4 also shows that the extent of the reduction varies dramatically by the external cause being considered.
Distributon of E code group with and without the fully restrictive selection procedure* for discharges with principal diagnosis of injury, 1998
Figure 4 shows the trends in rates using unrestricted and restricted criteria.
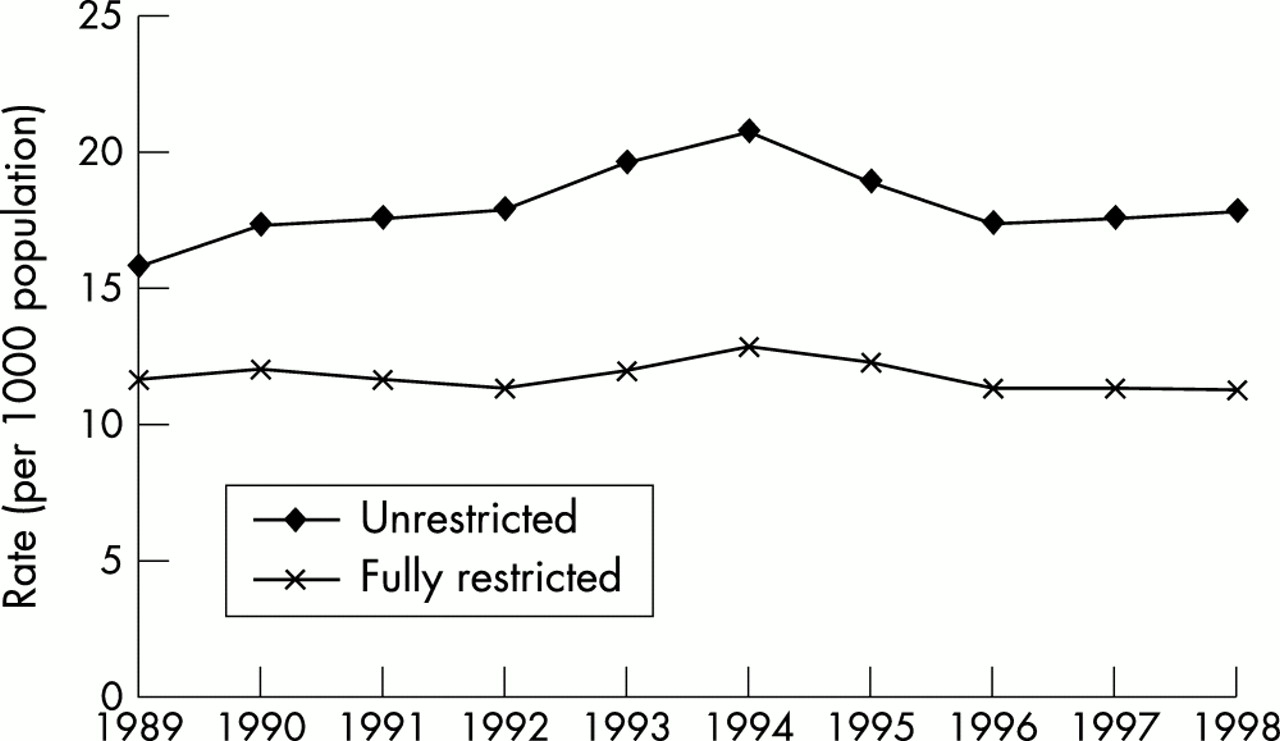
Trends in rates (age adjusted) of injury discharges with and without full restrictions, 1989–98.
Incidence, prevalence, and discharges
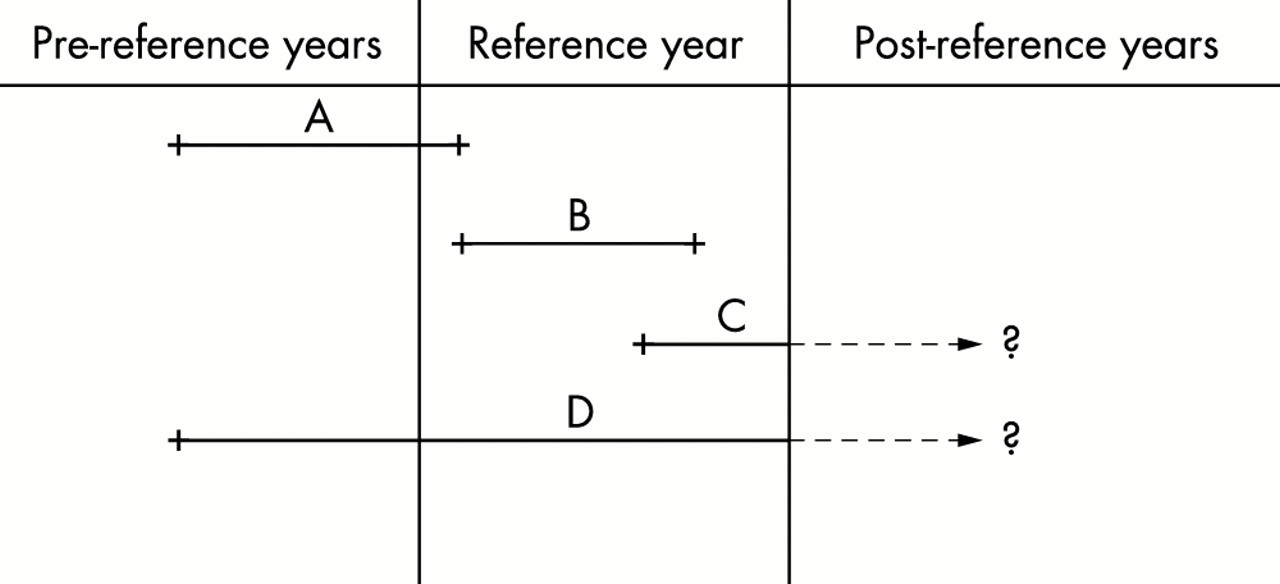
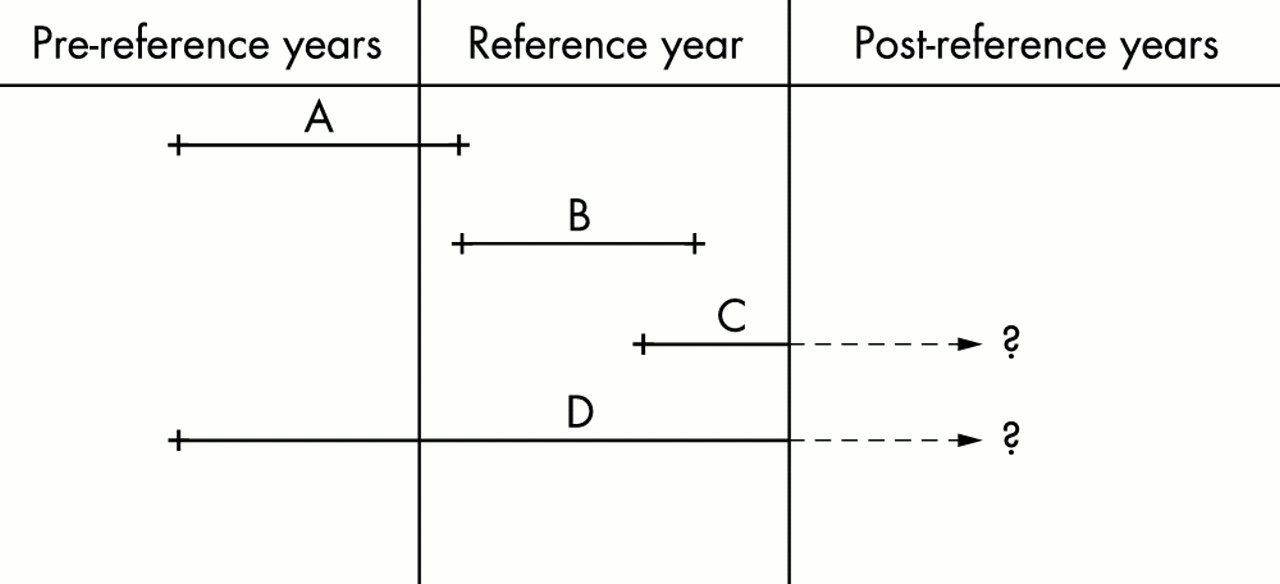
The total number of discharges each year, after excluding readmissions, is not a measure of incidence, that is new cases of injury for that year. As illustrated in fig 5 the total discharges (A+B) in a reference year will exclude new cases of injury which were admitted in the reference year but were not discharged in that year (C). These cases can only be “detected” once they are discharged. Similarly, the total discharges in the reference year includes cases admitted before the reference year but discharged in the reference year (A).
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Alternative admission and discharge date scenarios.
It should also be noted that the total number of discharges each year (A+B) is not a measure of prevalence, that is old and new cases, since as has been demonstrated it does not include all new cases in the reference year, but also because it does not include those existing cases where the victim was admitted before the reference year and discharged after the reference year (D).
The effects of these various scenarios are illustrated in table 5. Using discharges (A+B) to estimate incidence (B+C) consistently results in an overestimate of between 0.1%–3.1%.
Distribution of cases by injury and discharge year for fully restricted cases discharged, 1989–98
DISCUSSION
The results show that estimates of incidence of injury requiring hospital inpatient treatment in New Zealand will be substantially inflated if they are based solely on whether a patient has an E code or not. While almost all injury cases had an E code, having a E code did not necessarily mean the patient had an injury.
In our analyses we used the operational definition of an injury as those pathologies included in the injury and poisoning chapter (XVII) of the International Classification of Diseases. Our analysis of diagnoses for those injuries due to medical procedures raises questions about this traditional approach. Ninety three per cent of the relevant E codes had pathologies in the diagnostic range: “complications of surgical and medical care not elsewhere classified” (996–999). Reference to fourth digit classifications for these codes suggests that the majority are not injury as has been theoretically defined.5 A further 3% were 995: “certain adverse effects not elsewhere classified”. Smith and others have argued that conditions in the range 995–999 should be excluded from the definition of injury for most studies because they have different aetiology and means of prevention.8 In our view, neither is sufficient grounds for exclusion. Rather the decision should be based on whether they meet the theoretical definition of injury. Many would appear not to. Typical of these is 996.0: “mechanical complication of cardiac device, implant and graft”. There are, however, some notable exceptions, for example: 997.0: “central nervous complications (for example, anoxia brain damage during or resulting from a procedure)”, 998.2: “accidental puncture or laceration during a procedure”, 998.4: “foreign body accidentally left during a procedure”.
It has also been pointed out that the converse situation exists within the International Classification of Diseases, 9th revision, namely that there are conditions which fall outside the 800–999 range which some would classify as injury.7 These include musculoskeletal conditions related to the knee and back (717, 718, 724) and certain conditions of the eye (366.2).
We only examined cases that had a principal diagnosis of injury in the range 800–999. As we have shown in fig 2 this is critical for interpreting trends in injury. This result serves to illustrate how susceptible trends in injury may be to changes in health services management practice. Ideally when examining trends in injury the choice of indicator should be minimally susceptible to such effects. One approach would be to select only those injury cases which meet an anatomical severity threshold.9
The principal diagnosis field is meant to be used to code the primary reason the patient was admitted for treatment. How well this was done for the series we examined is not known. Moreover there would be cases where it would be difficult to make such a decision—for example, a patient who had a cardiac arrest and a major injury.
The results for day patients and readmissions further underscore the importance of considering the biases in estimates of incidence which occur when they are not excluded. The size of the effects for various case selection criteria serve as a significant warning for others producing country specific estimates and undertaking international comparisons of the incidence of injury requiring hospital inpatient treatment.
Our examination of date of injury and date of discharge serves as warning that users of similar data from other countries should not assume the number of cases admitted in a reference year which are not discharged in that year is offset by the number of cases discharged in the reference year which were admitted prior to the reference year. As we have shown for New Zealand the effect is to consistently overestimate incidence, although the effect is relatively small.
We recommend that:
Those using New Zealand hospital discharge data for determining the incidence of injury should: (a) select cases which meet the following criteria: principal diagnosis injury only cases, patients with day stay of one day or more, and first admissions only, (b) note in their reporting that the measure is an estimate and could be as high as a 3% overestimate.
Other countries with similar data should investigate the merit of adopting a similar approach.
That the International Collaborative Effort on Injury Statistics review all diagnoses within International Classification of Diseases 9th and 10th revisions with view to reaching consensus on an operational definition of an injury.
Finally, it should be noted that our recommendations are concerned with measuring the incidence of injury. There will be other circumstances when one may well select cases differently. For example, including readmissions with first admissions would be appropriate in determining the total burden of hospital treatment. Similarly, examining car crashes which are due to disease (for example, fatal heart attack) may provide useful insight into new opportunities for prevention.
Acknowledgments
The Injury Prevention Research Unit is funded by the Health Research Council (HRC) of New Zealand and the Accident Compensation Corporation (ACC). Views and/or conclusions in this article are those of the authors and do not necessarily reflect those of HRC or ACC. The authors wish to thank Dorothy Begg, Lois Fingerhut, Hank Weiss, and James Harrison for their helpful comments on earlier versions of this paper.