Article Text

Abstract
Background and aims Bicycling may be less appealing in parts of the world where cycling is less safe. Differences between jurisdictions suggest route design is key to improving safety and increasing ridership. Previous studies faced difficulties in effectively assessing denominators for risk calculations and controlling confounding. This paper describes the advantages of the case-crossover design of the Bicyclists' Injuries and the Cycling Environment study to address these challenges to observational studies of cycling safety.
Methods Injured cyclists were recruited from the emergency departments of five hospitals in Vancouver and Toronto, Canada. In 18 months, 690 participants were successfully recruited and interviewed. Each participant was interviewed to map the route of their injury trip, identify the injury site and select two control sites at random from the same route. Infrastructural characteristics at each study site were scored by site observers who were blinded as to whether sites were crash or comparison sites. Analyses will compare infrastructural variables between case and control sites with conditional logistic regression.
Discussion This study presents a novel application of the case-crossover design to the evaluation of relationships between infrastructure and cycling safety while controlling confounders and exposure to risk. It is hoped that the value of this method and the efficiency of the recruitment process will encourage replication in other locations, to expand the range of cycling infrastructure compared and to facilitate evidence-based cycling infrastructure choices that can make cycling safer and more appealing.
- Bicycling
- crossover studies
- epidemiology
- injuries
Statistics from Altmetric.com
Bicycling is an underused mode of transportation in Canada and the USA, comprising only approximately 1–2% of urban trips, in comparison to 10–28% of urban trips in European countries such as Austria, Germany, Switzerland, Sweden, Denmark and The Netherlands.1 In surveys, participants emphasise safety concerns that deter them from cycling.2–6
Concerns about safety are well founded. Data from North America and Europe indicate that cyclists are three to 70 times more likely to be injured per trip or per kilometre travelled than car occupants.1 7 There are also clear differences between continents: mortality data from Canada and the USA suggest North American cyclists are two to six times more likely to be killed than cyclists in Denmark and The Netherlands;1 8 and US data suggest American cyclists are eight times more likely to have serious injuries than cyclists in Germany, and 30 times more likely to have serious injuries than cyclists in The Netherlands.1 While these comparisons are cause for concern, the case can be made that there is potential for cycling safety in North America to be improved.
Improving safety is desirable in itself but also has the potential to increase bicycle ridership.5 Increased ridership can in turn improve safety through the ‘safety in numbers’ effect: more bicycles on the roads are a reminder to drivers to watch for potential conflicts with cyclists; and as more people use bicycles for at least some trips, there is a greater chance that drivers will also be cyclists and be more aware of their obligations towards these fellow road users.9–12 Modifications to the built environment—in particular road-related infrastructure—are a key component for improved safety. There are classic public health advantages13 to this approach: changes to road infrastructure affect the entire population; safer infrastructure does not require active choice for protection to be engaged (unlike helmets or bicycling skills courses); and the benefits of infrastructure are long-lasting after implementation.
Given that the built environment is a logical target for intervention, rigorous empirical analyses of infrastructural influences on safety or risk are needed. We have previously conducted a comprehensive review14 of studies of cycling infrastructure and risk of injury published in the peer-reviewed literature. These peer-reviewed studies suggested that purpose-built bicycle facilities (such as on-road marked bike lanes,15–17 bicycle routes,15 bicycle paths,15 18 and separated cycle tracks at roundabouts19–21 reduce the risk of cycling injury (see Reynolds et al14 for detailed definitions of transportation infrastructure). However, we also concluded that the previous research examining infrastructure safety has encountered several challenges. One is a lack of consistent definitions of infrastructure, which would more easily allow comparisons between studies. It is also difficult to ensure that infrastructure is not categorised such that types with different risks are grouped together (eg, sidewalks and off-street paths), particularly when risks are not yet fully understood. Among the other complexities of observational research on the infrastructural determinants of cycling safety and injury are two important methodological issues that are particularly evident to population health researchers: adequately measuring exposure to risk and controlling for potential confounders. In designing the Bicyclists' Injuries and the Cycling Environment (BICE) study, we paid particular attention to these issues.
Denominator problems in observational studies of bicycling infrastructure
In some before–after studies of infrastructural interventions, such as the conversion of intersections into roundabouts,22 getting accurate denominators to calculate injury rates (instead of simple injury counts) has been a challenge, especially when the traffic volume varies with time (eg, time of day, by season, etc.) or even as a result of the intervention itself.22 Simply adjusting for city-wide averages of bicycle volumes23 does not necessarily provide the fine scale differences in denominators required for comparing infrastructure designs. Previous intervention studies have attempted to address the denominator issue by adjusting for average bicycle and motor vehicle volumes in the target area,24 or comparing both injury counts and observed traffic volumes in unchanged intersections,20–22 25 but these may be difficult to assess accurately and precisely. In studies in which injured cyclists are compared with non-injured cyclists, issues of comparability on exposure to risk (eg, time spent cycling) arise. Several previous studies have attempted to adjust their risk analyses with a measure of distances travelled on various infrastructure,7 15 17 26 while others have focused on riding time to control for exposure to risk.18
Confounding
In studies comparing injured cyclists with non-injured cyclists, differences in personal factors that influence one's choice of cycling infrastructure and one's risk of injury are potential confounders. Some of the individual differences are likely to be accounted for by consideration of common confounders such as age7 17 18 27–29 or sex,7 16 19 20 or even helmet use.28 30 31 However, other factors may be as yet unidentified confounders that are difficult to measure.
Addressing exposure to risk and confounding with the case-crossover study design
To ensure comparability on exposure to risk and to account for unmeasured confounders we designed a case-crossover study, in which participants serve as their own controls.32 The design can be used to compare the environmental characteristics at the point in time and space when an injury event occurred with the characteristics at a point in time and space when no injury occurred (eg, earlier on the same trip). The case-crossover approach is particularly useful for evaluating risk factor behaviours or exposures that vary through time and their association with distinct acute events.32–34 We designed a case-crossover study to compare characteristics of the transportation infrastructure at the location of a cycling injury event with the infrastructure at a randomly selected point on the same route of travel where no injury occurred. An overview of the design and its advantages is provided in figure 1. A logistical advantage of the case-crossover study is that, as external control subjects are not required, recruitment can be much more efficient.

Overview of the design of the Bicyclists' Injuries and the Cycling Environment (BICE) study.
Methods
Study locations and study population
Vancouver and Toronto are two of the largest urban centres in Canada, with populations of approximately 2.2 million and 5.4 million, respectively. They have different weather patterns, transportation infrastructures and proportions of the population who cycle at least once per week (12% in Vancouver vs 6% in Toronto).35 Together, these urban areas incorporate a wide variety of cycling infrastructure including on-road cycling lanes, shared road lanes, traffic-calmed roads, off-road paths for cyclists only and mixed use paths. The study population consisted of adult cyclists (aged 19 years and older) who resided and cycled in Vancouver or Toronto.
Participant recruitment
Adults injured while riding a bicycle who attended the emergency department of one of five study hospitals (St Paul's and Vancouver General hospitals in Vancouver and St Michael's, Toronto General and Toronto Western hospitals in Toronto) were prospectively recruited as cases. We excluded cases who were:
Fatally injured, because there were few during the study period (two in total) and route reconstruction was impossible without interviewing the injured cyclist.
Younger than 19 years old at the time of the injury incident.
Unable to communicate with research staff either because of their injuries or language barriers.
Injured during a trip in which they were trick riding, racing, or mountain biking, because the BICE study focused on urban utilitarian cycling for which urban cycling networks are designed.
Riding with more than one cyclist on the bicycle (although users of trailers were included).
Living or injured outside of Toronto or Vancouver.
On-site research staff reviewed emergency department charts to identify injured cyclists who attended for treatment, and our study coordinators contacted each potential participant in their respective cities, screened them for eligibility, requested participation and arranged interviews. Participants were interviewed as soon as possible after the injury incident to maximise recall. Our protocol was reviewed and approved by the research ethics boards at each of the five hospitals, as well as the University of British Columbia and the University of Toronto.
Interviews: injury and control site selection
Our trained study interviewers used a structured questionnaire to conduct interviews lasting approximately 30 min. The primary purpose of the interview was to identify and map the route of the participant on the injury trip, including any trip continuation after the event. We used detailed maps (including streets and off-street paths) on which each participant identified their route and injury site. Each route was used to generate two comparison sites (figure 1) where no injury occurred. To do this, two random proportions between 0 and 1 were selected and applied to the total route distance to select two points. The second of these points was matched to the intersection/non-intersection status of the injury site by moving the site for observation to the nearest intersection or non-intersection point as required. Random selection of the two control sites meant that the probability of selection of a specific infrastructure type was proportional to the relative length of the infrastructure on the injury trip, ie, exposure to the infrastructure. The interviewers asked about the circumstances of the injury event and about transient characteristics of the sites on the injury trip: cyclist's direction of travel compared with traffic; whether the cyclist was with companions; street surface conditions; light conditions and estimated speed.
The following descriptive information was also collected, although the case-crossover design controlled for these within-trip and within-person characteristics: the time of day; weather conditions; the type of bike; the use of bike lights; reflectors on the bike or clothing; the conspicuity of the clothing worn; the use of a helmet; characteristics of the cyclist: age; sex; education; household income; cycling experience; cycling training; cycling frequency; use of drugs or alcohol in the preceding 6 h and sleep in the previous 24 h.
Site observations
The local study coordinators assigned GPS coordinates to the injury site and the identified control sites after each interview. Data about cycling infrastructure at each of the three sites were collected during site observations by trained study personnel. The site observers were blinded to site status (ie, injury site or control site). The observer was provided with GPS coordinates and the site description from the interview to locate each site. Observers were provided with a target range for the time of day to conduct observation (to match this to the time of day when the injury occurred). We used a structured observation form to record: type of route (eg, street or off-road path); intersection type; presence of car parking; presence of junctions; slope of the surface; type of road surface; road surface quality; cyclist traffic volume; motor vehicle traffic volume; motor vehicle traffic speed; available street lighting and land use.
Recruitment progress
A total of 2335 injured cyclists were identified at the five study hospitals from 1 June 2008 to 30 November 2009. Approximately 39% of these were found to be ineligible (primarily because they resided or were injured outside the city), and 25% were not contactable within 10 phone calls or 3 months of the injury date. Of those eligible and contacted, 18% refused; the most common reason for refusing was lack of time, although a few also reported being too injured, legal issues related to the injury and being embarrassed about the injury circumstances. The final study sample of 690 participants exceeded our planned sample of 600, and was recruited in 18 months, 6 months ahead of schedule. The participants were 59% male, and the mean birth year was 1971, suggesting that this injured sample was similar to participants in a recent survey of current and potential cyclists in Vancouver.6 The mean length of the injury trips was 5.4 km, but this was variable (SD 7.2 km). The participants were mainly regular cyclists, with 72% reporting cycling four or more times per week in summer, and 46% reporting cycling at least once per month even in winter months.
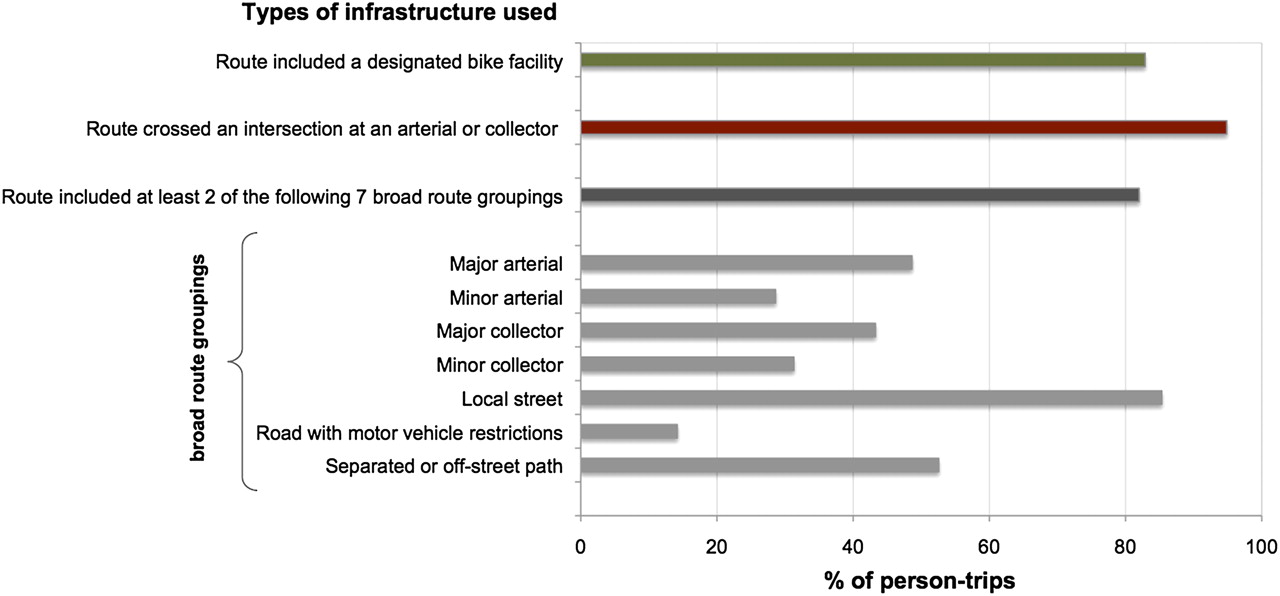
A concern with the case-crossover design is overmatching, which occurs when there is insufficient variance in exposure (ie, transportation infrastructure) between the injury and control sites, because the comparisons occur within trips and individuals—not between individuals. We might be concerned that the points on any single trip route would be too similar to each other (eg, a trip only along arterial roads) to allow meaningful comparisons. However, in a preliminary analysis of 409 of the routes in Vancouver, we found 339 of the trips used a designated bicycle facility for at least part of their trip, all but 21 trips crossed an arterial or collector road, and 82% of the trips used at least two of seven broad route categories, suggesting that overmatching will not be a problem for our analyses (figure 2).
{kind=link}
{kind=link}
Types of infrastructure used in the Bicyclists' Injuries and the Cycling Environment (BICE) study, based on preliminary analyses of 409 of 690 injury trips (all within Vancouver).
Planned analyses
The initial analyses will focus on tabulating descriptive statistics about the cycling environments of the non-injury sites (to provide an understanding of the use of various types of cycling infrastructure in the study regions) and of the injury sites (to document the injury environments). To our knowledge, characterisations of cycling environments at the level of detail offered by this study are not available in the literature.
Inferential analyses will examine associations between the physical cycling environment and the binary dependent variable (1=injury ‘event’ or 0=no event) using conditional logistic regression appropriate to the matched design. The central analysis will compare the odds of injury by the type of route travelled, where the route type will include the availability of bicycling infrastructure and any separation from motor vehicle traffic (see table 1 for the proposed levels for the route type variable). Secondary analyses will compare the odds of injury for different intersection designs (eg, roundabouts vs two-way stops) including factors such as speed and volume of motor vehicle traffic, width of road and lanes, presence of car parking and streetcar tracks.
Infrastructural variables to be analysed in the Bicyclists' Injuries and the Cycling Environment (BICE) study
Discussion
The case-crossover design described here will allow a unique investigation of the influences of the built environment on cycling injury that controls for individual differences in exposure to risk and potentially confounding personal and trip characteristics. Our recruitment results indicate that the method generated a large sample size in a short period of time, and that a broad variety of infrastructure can be compared despite the restriction to within-trip comparisons inherent in the design. We hope the feasibility demonstrated here encourages future studies employing a similar design in additional cities to allow the evaluation of even wider ranges of cycling infrastructure. Systematically investigating the influences of the built environment on injury risk will allow urban planners and transportation engineers to make informed design choices to make cycling safer and more appealing.
Acknowledgments
The authors would like to acknowledge the work of the many community and hospital collaborators and the staff of the BICE study (a full list is available here: http://www.cher.ubc.ca/cyclingincities/injury.html).
References
Footnotes
Funding The study was funded by the Heart and Stroke Foundation of Canada and the Canadian Institutes of Health Research (Institute of Musculoskeletal Health and Arthritis and Institute of Nutrition, Metabolism and Diabetes). CCOR recognises funding from the Natural Sciences and Engineering Research Council of Canada, and MW and MAH acknowledge funding from the Michael Smith Foundation for Health Research. MAH recognises funding from the Public Health Agency of Canada. MAH, MC and MW received additional funding from the Canadian Institutes of Health Research. The opinions expressed herein are those of the authors and not necessarily those of the funding agencies. Early drafts of this research protocol benefitted from comments and suggestions from participants in the 2005–6 Bridge Program Grant Development Course at the University of British Columbia and from anonymous reviewers affiliated with the funding agencies.
Competing interests None.
Ethics approval This study received ethis approval from ethics boards at the University of British Columbia, University of Toronto, St Paul's Hospital, Vancouver General Hospital, St Michael's Hospital and Toronto University Health Network.
Provenance and peer review Not commissioned; externally peer reviewed.