Article Text

Abstract
Retrospective data extraction from two complementary mortality datasets determined the descriptive epidemiology and population rates in unintentional drowning deaths at surf beaches (n = 129). The annual average crude surf beach drowning rate was 0.28 per 100 000 population for males and 2.36 per 100 000 population for international tourists. The study generated hypotheses for risk assessment to assist intervention: adult males, international tourists, people with cardiovascular conditions, and exposure to rip currents.
Statistics from Altmetric.com
Many countries have ocean beaches with surf activity. At surf beaches, the highest incidence of drowning occurs in adolescent and adult males, possibly because of more frequent and/or risk-intense exposure to surf bathing.1 Three sources of environmental hazard have been identified at surf beaches: breaker height and type; variations in water depth; currents.2 Person-related factors that influence risk include swimming outside lifeguard-patrolled areas, at unpatrolled beaches, or during non-patrol periods.3
Drowning studies have included beach as a location variable.4–7 Other studies have also reported risk and protective factor prevalence among drownings at surf beaches including alcohol and resuscitation.89 Developing effective countermeasures requires further understanding the relationship of situation-related and person-related factors to drowning risk on surf beaches.
The study primarily aimed to describe the epidemiology of surf beach drowning including the prevalence of potential risk factors. A parallel aim was to examine the strengths and limitations of two complementary mortality datasets available for the Australian population, one containing coroner data and the other maintained by a national lifesaving organization.
METHOD
Data collection
The National Coroners Information System (NCIS) provides an in-depth descriptive investigation of surf beach drowning by web-based retrieval of death records reported to Australian coroners. The Incident Report Database (IRD) provides drowning information from the year 2000, reported by volunteer and professional lifesavers or sourced from media.
Case inclusion criteria for drowning deaths (extracted from both datasets) were:
occurred 1 July 2001–30 June 2005 immediately or after the incident;
occurred at an Australian coastal location exposed to ocean-derived waves (excludes large bays and harbors protected from ocean swell);
victim was engaged in recreational water activity accessed directly (excludes attempting rescue or access by watercraft);
circumstances indicated unintentional drowning and this was not definitively ruled out by medical records or other evidence.
Data were accessed in January 2006. Drowning deaths (n = 1286) were identified in the NCIS from the mechanism code supplemented with a text search for “drown” (and derivatives). Drowning at built locations was excluded by inspection of the object field (eg, bathtub). A location check excluded drowning in natural non-coastal water bodies. The remaining records were reviewed for inclusion by applying criteria 1–4 to case documentation.
IRD cases were identified from reports of specified surf beach drowning. After a cross-check with NCIS cases, all additional records meeting the inclusion criteria were added to the study dataset. Cases were identified in both databases by matching the date of incident or victim’s name.
Annual crude death rates were calculated manually from resident population data, adjusted proportionally by year for the average number of days of travel by short-term (<1 year) international inbound and outbound travelers.10–12 Annual age-specific rates relied on resident population data only (age data not available for short-term travel). The annual international tourist rate was based on adjusted short-term international inbound travel by average number of days of travel.
Outcome measures and analysis
Complementary data were extracted from the NCIS and IRD using the case inclusion criteria. The mutually exclusive methods of record collection allowed a comparison of completeness for each database.
Eleven available variables were considered germane to the study aims after literature review and expert consultation. The variables (sex, age group, health condition, implication of drugs or alcohol, proximity of residential address to coastline, swimming ability, surf activity, proximity of others in water, rip (seaward moving) current implicated, cardiopulmonary resuscitation (CPR), and swimming in a patrolled (supervised) zone) were ascertained from case documents or recorded data. Results are reported as annual rates per 100 000 population, case frequency, and percentage.
RESULTS
Subject identification and database completeness
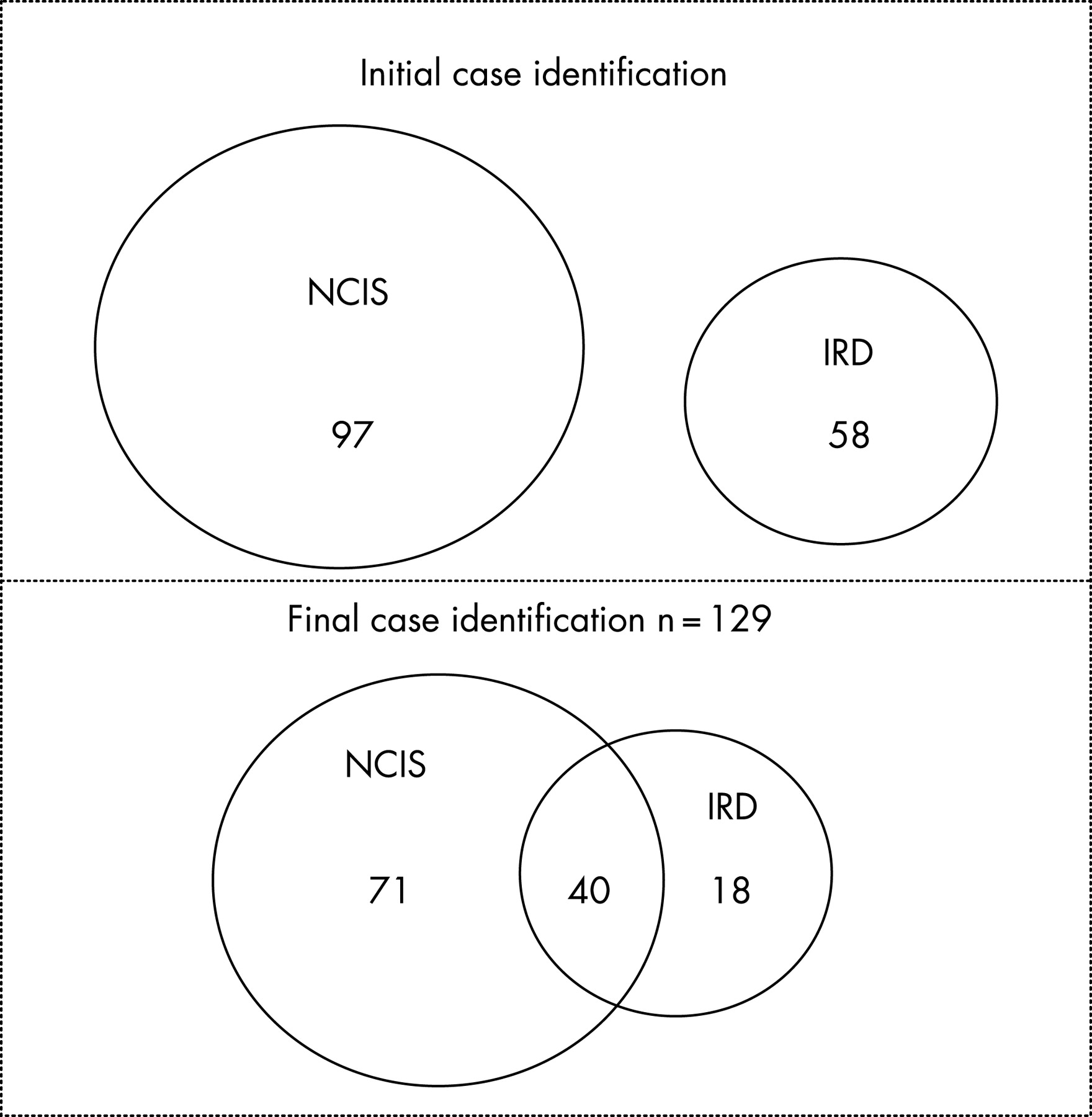
The case search criteria applied initially to each database identified 97 NCIS and 58 IRD cases. A subsequent comparison of cases identified 14 additional (misclassified) NCIS cases but no additional IRD cases. The final total was 111 NCIS cases and 58 IRD cases with 40 common to both databases (fig 1). IRD cases (18) not found in the NCIS probably remained open at the time of the data search (cases are updated and completed when closed by the coroner), and cases not found in the IRD (71) probably occurred without lifesaver knowledge or media reporting. Of the total dataset of 129 cases (annual average rate 0.16/100 000 population), 86% were identified in the NCIS and 45% in the IRD.

{kind=link}
Candidate risk factors
Data completeness varied among selected variables (eg, missing age and sex in one case, missing swimming ability in 116 cases). Overall, 110 males (85% with an annual average rate of 0.28/100 000 population) and 18 females (14% with an annual average rate of 0.04/100 000 population) drowned at Australian surf beaches over the 4-year period. Age ranged from 13 to 86 years, with drowning most common in the 20–29-year age group (n = 31) followed by the 50–59-year age group (n = 23). The majority of drowning deaths comprised males in all age groupings. The highest crude age group drowning rate (table 1; this can be found at http://ip.bmj.com/supplemental) was for 60–69 years (0.29/100 000 population).
Table 2 lists person-related factors. An underlying medical condition was reported for 39 (30%) cases. Of these, 34 (87%) were cardiovascular conditions, including acute myocardial infarction and ruptured aorta, preceding the drowning. In a further six cases, a head or spinal injury was suffered before drowning. The use of alcohol or drugs was identified as a contributing factor for seven deaths (toxicology reports), and reported in police or lifesaver reports for four more cases (no NCIS toxicology available for verification). Most of the decedents were Australians resident within 10 km of the coastline. Almost 25% were international tourists (annual rate of 2.36 surf beach drownings/100 000 population for international inbound tourists, corrected for average number of days of travel in Australia). Where swimming ability was recorded, 12 of 13 victims had been able to swim.
Table 3 lists situation-related factors. Most drowning victims were engaged in swimming/wading activities and were near others in the water. In 28 (22%) cases, police or lifesavers reported the victim being swept seawards in rip currents. CPR was attempted for 83 (64%) cases. One drowning was recorded within a patrolled (supervised) zone.
DISCUSSION
A descriptive epidemiological investigation of drowning deaths in swimmers and surfers on a surf beach in Australia is reported. The prevalence of selected factors provides direction for further investigation and, given the limitations of the dataset, areas for potential improvement in mortality data collection.
A higher crude drowning rate for adult males at surf beaches accords with previous drowning studies of populations in natural unsupervised aquatic locations.13 However, investigation is required to determine whether the male over-representation is explained by exposure or other risk factors.
The association of cardiovascular conditions or events with 26% of drownings in this population-based study warrants further investigation. It is recognized that cardiovascular disease limits the ability to increase cardiac output during vigorous exercise, resulting in a higher risk of an acute cardiovascular medical condition.14 Although cardiovascular conditions reported here were predominantly specified as a contributing cause of death, pathology reports (where available) did not routinely state whether the drowning resulted from an associated acute event. Case–control studies accounting for exposure to vigorous exercise are required to confirm whether acute events related to pre-existing cardiovascular conditions are a risk factor for surf beach drowning.
Key points
This descriptive epidemiological investigation of possible factors associated with surf beach drownings will assist with the design of analytical studies of risk factors including exposure.
The study generated candidate risk factors for investigating surf beach drownings including adult males, international tourists, people with cardiovascular conditions, and exposure to rip currents.
The study demonstrates the ability of the National Coroners Information System to provide detailed and timely information on deaths from injury and the benefits of complementary datasets in injury epidemiology.
In this sample, 65% of drowning victims had resided within 50 km of the coastline; international tourists comprised 25% of cases. Given that 85% of Australians live within 50 km of the coastline and over 60% of international tourists go to a beach, these patterns presumably reflect levels of surf experience and frequency of water exposure.1015–17 The findings also show that flotation devices used in surfing activities (eg, surfboards), swimming aids (eg, flippers used for snorkeling/diving), and swimming near others did not prevent drowning in the cases reported here. The study did not provide a controlled test of the effectiveness of CPR, as time of immersion was not routinely recorded in either database.
The study was limited by incomplete or missing data. For example, drugs and alcohol were implicated in relatively few (8%) drownings, yet a previous study using a comparable geographic sample found that 25% of recreational drownings were associated with alcohol use.4 Given this, and the absence of toxicology reports for some cases in the present study, the association of alcohol with recreational surf beach drowning is probably under-reported. Information was also lacking on the role of swimming ability in surf beach drowning (not recorded in 90% of cases). To facilitate the investigation of the role played by swimming competence in surf drowning, these data should be routinely collected in mortality records.18 Similarly, although rip currents were reported in 22% of surf beach drownings, collection of this variable in mortality records is not routine. The association of rip current with surf beach drowning may therefore be more common than reported.
Although the study dataset is limited, the method shows the capacity of the NCIS to provide timely and detailed injury-related mortality data. Although the data were retrieved just 6 months after the study period, 86% of known cases were identified. Use of the IRD dataset, together with laborious text searches of the NCIS, was essential to identifying misclassified or open cases. However, the NCIS is a relatively new research tool and is subject to improvement through ongoing review. The IRD provides a useful comparative and additional source of information for this injury problem, but the method of data collection precludes inclusion of surf beach drownings unknown to lifesavers or unreported in the media.
IMPLICATIONS FOR INJURY PREVENTION RESEARCH
New knowledge from this study on possible risk and protective factors associated with surf beach drowning provides hypotheses for future analytical epidemiological studies. At present, beach and water exposure data are not available for surf beaches in Australia. Specific measures of exposure to surf beaches are required to inform relative risk data to assist the development of targeted injury prevention strategies.
Acknowledgments
We thank the following: Peter Agnew, Surf Life Saving Australia, for access to the IRD; Chris Rigg, Tourism Research Australia, for supplementary visitor data; Amanda Hinkley, Marde Hoy, and Andrew Short for assistance with case identification from the NCIS; Carolyn Staines and anonymous reviewers for insightful comments on manuscript drafts.
Supplementary materials
web only table 14/1/62
Files in this Data Supplement:
Footnotes
Competing interests: None.
Ethics approval: Ethical approval was granted by Monash University Standing Committee on Ethics in Research Involving Humans, project Nos 2004/572EA, 2005/760EA, and M0004-2.