Article Text

Abstract
Introduction: The Barell body region by nature of injury diagnosis matrix standardizes data selection and reports, using a two dimensional array (matrix) that includes all International Classification of Diseases (ICD)-9-CM codes describing trauma.
Aim: To provide a standard format for reports from trauma registries, hospital discharge data systems, emergency department data systems, or other sources of non-fatal injury data. This tool could also be used to characterize the patterns of injury using a manageable number of clinically meaningful diagnostic categories and to serve as a standard for casemix comparison across time and place.
Concept: The matrix displays 12 nature of injury columns and 36 body region rows placing each ICD-9-CM code in the range from 800 to 995 in a unique cell location in the matrix. Each cell includes the codes associated with a given injury. The matrix rows and columns can easily be collapsed to get broader groupings or expanded if more specific sites are required. The current matrix offers three standard levels of detail through predefined collapsing of body regions from 36 rows to nine rows to five rows.
Matrix development: This paper presents stages in the development and the major concepts and properties of the matrix, using data from the Israeli national trauma registry, and from the US National Hospital Discharge Survey. The matrix introduces new ideas such as the separation of traumatic brain injury (TBI), into three types. Injuries to the eye have been separated from other facial injuries. Other head injuries such as open wounds and burns were categorized separately. Injuries to the spinal cord and spinal column were also separated as are the abdomen and pelvis. Extremities have been divided into upper and lower with a further subdivision into more specific regions. Hip fractures were separated from other lower extremity fractures.
Forthcoming developments: The matrix will be used for the development of standard methods for the analysis of multiple injuries and the creation of patient injury profiles. To meet the growing use of ICD-10 and to be applicable to a wider range of countries, the matrix will be translated to ICD-10 and eventually to ICD-10-CM.
Conclusion: The Barell injury diagnosis matrix has the potential to serve as a basic tool in epidemiological and clinical analyses of injury data.
- Barell matrix
- ICD, International Classification of Diseases
- ICE, International Collaborative Effort
- NHDS, National Hospital Discharge Survey
- TBI, traumatic brain injury
- Barell matrix
- ICD, International Classification of Diseases
- ICE, International Collaborative Effort
- NHDS, National Hospital Discharge Survey
- TBI, traumatic brain injury
Statistics from Altmetric.com
- Barell matrix
- ICD, International Classification of Diseases
- ICE, International Collaborative Effort
- NHDS, National Hospital Discharge Survey
- TBI, traumatic brain injury
- Barell matrix
- ICD, International Classification of Diseases
- ICE, International Collaborative Effort
- NHDS, National Hospital Discharge Survey
- TBI, traumatic brain injury
The Barell body region by nature of injury diagnosis matrix standardizes data selection and reports, using a two dimensional array (matrix) that includes all International Classification of Diseases (ICD)-9-CM codes describing trauma. The matrix has the potential to serve as a basic tool in the epidemiological and clinical analysis of injury diagnosis data.
The matrix was originally designed in 1996 by researchers from the Injury Prevention and Control Section of the Health Services Research Unit in the Israeli Ministry of Health and by clinical personnel from the Trauma Branch of the Israeli Defense Forces Medical Corps. Development was initiated by Barell at meetings of the International Collaborative Effort (ICE) on Injury Statistics in 1997.1–4 A parallel matrix was designed by Mackenzie and Champion.5 The matrix was finalized at the ICE meeting of 2001, after which the united version presented in this paper was completed.
This paper describes the stages in the development and the major concepts and properties of the Barell injury diagnosis matrix.
OBJECTIVES
The matrix is a tool for standardized retrieval of injury cases for epidemiological, clinical, and management oriented analyses. It could be used to:
Characterize the patterns of injury resulting from diverse circumstances using a manageable number of clinically meaningful diagnostic categories.
Serve as a standard for casemix comparison across time and place.
Simplify the process of classifying injuries using ICD-9-CM in a trauma setting.
Provide a standard format for reports from trauma registries, hospital discharge data systems, emergency department data systems, or other sources of non-fatal injury data.
CONCEPT
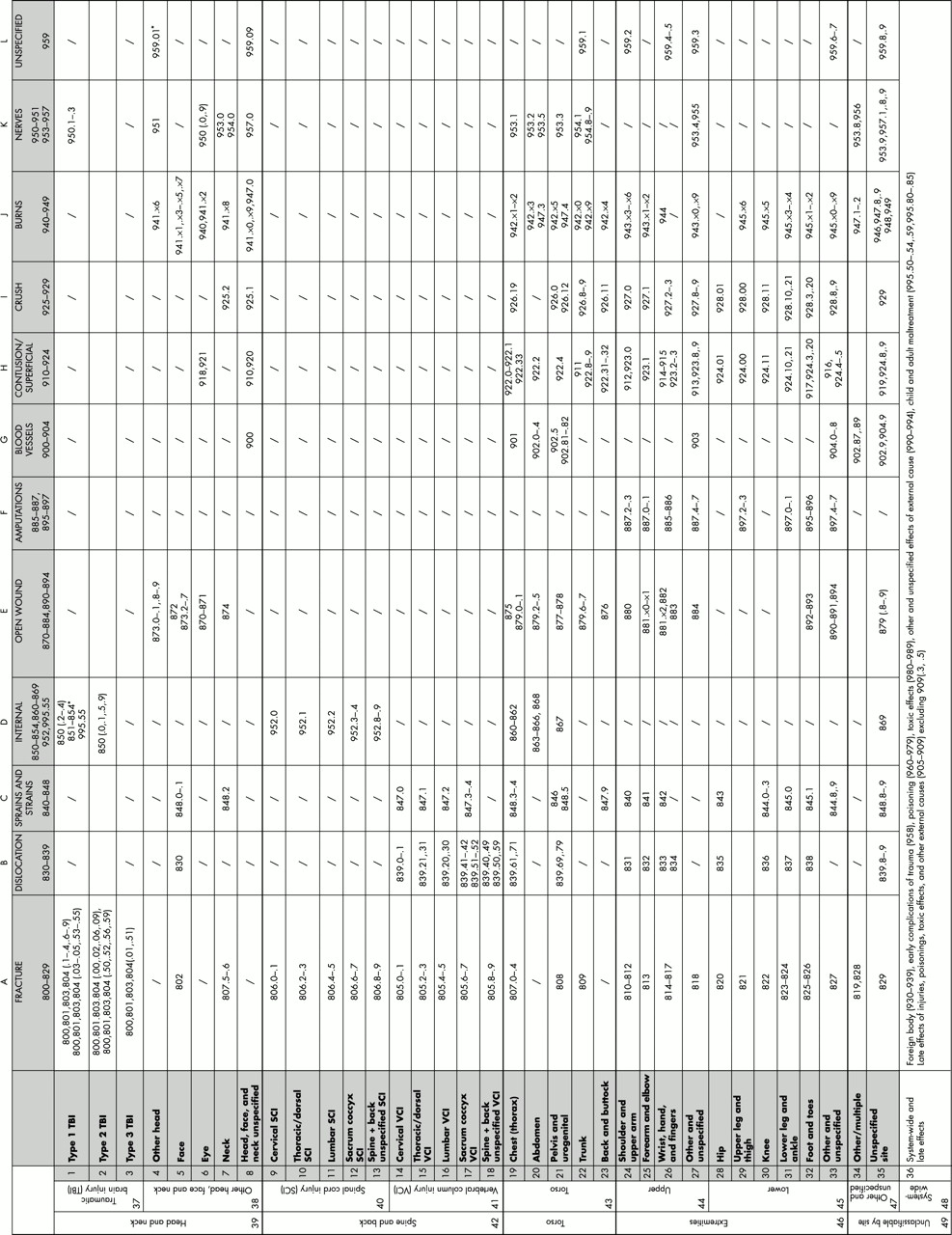
Most traumatic injuries can be described using 12 systematically classified injury natures. These are fractures, dislocations, sprains and strains, internal injuries, open wounds, amputations, injuries to blood vessels, contusions and superficial injuries, crush, burn, and nerve injuries. When these “nature of injury types” affect different body regions they form the various injuries detailed serially in the ICD-9-CM codes.6 The matrix depicts the nature of injury in the columns and body region in the rows. The placement of ICD-9-CM codes in their “appropriate” cells gives substance to the matrix. The matrix rows and columns can easily be collapsed to get broader groupings or expanded if more specific sites are required. The current matrix offers three standard levels of detail through predefined collapsing of body regions from 36 rows to nine rows to five rows (fig 1).

{kind=link}
The Barell injury diagnosis matrix; classification by body region and nature of injury (based on five digit ICD-9-CM codes). *Note from CDC: 959.01 (added to ICD-9-CM in 1997) is not intended to be assigned to TBI cases; however, in the USA it has been assigned incorrectly to a substantial proportion of cases previously coded 854. For purposes of classification, head injuries are labeled as type 1 TBI if there is recorded evidence of an intracranial injury or a moderate or a prolonged loss of consciousness, shaken infant syndrome, or injuries to the optic nerve pathways. Type 2 TBI includes injuries with no recorded evidence of intracranial injury, and loss of consciousness of less than one hour, or loss of consciousness of unknown duration, or unspecified level of consciousness. Type 3 TBI includes patients with no evidence of intracranial injury and no loss of consciousness.
DEVELOPMENT OF THE MATRIX STRUCTURE
The matrix columns follow the sequence of ICD-9-CM codes. Column A includes ICD-9-CM codes 800 to 829, column B contains codes 830 to 839, column C codes 840 to 848, and so on. The columns have not changed much through the development process. The few changes that did occur include separation of amputations from open wounds (codes 885–887 and 895–897) and collapsing contusions and superficial injuries to form one column for ICD-9-CM codes 910 to 924. Amputations were separated from open wounds as they were recognized as an important source of disability receiving increasing attention.
The rows, however, are the product of a long iterative process involving much thought and intent. The most significant changes include:
Traumatic brain injury* (TBI) was initially defined based on the definition of the Centers for Disease Control and Prevention7 but later separated into three types of TBI. Type 1 TBI was defined where there was recorded evidence of an intracranial injury or a moderate or a prolonged loss of consciousness, shaken infant syndrome, or injuries to the optic nerve pathways. Type 2 TBI included injuries with no recorded evidence of intracranial injury, and a loss of consciousness of less than one hour, or loss of consciousness of unknown duration, or unspecified level of consciousness. Type 3 TBI included patients with no evidence of intracranial injury, and no loss of consciousness. The differences between these three classes using Israeli trauma registry data are described in example 1 below and shown in table 1.
Injuries to the eye are separated from other facial injuries.
Other head injuries, such as open wounds and burns, are categorized separately.
Injuries to the spinal cord and spinal column are separated as it was presumed that spinal cord injuries would be more severe and would involve a different type of disability and rehabilitation. Furthermore, the cross tabulation of detailed body regions for spinal cord and spinal column injuries showed differences as detailed in example 2 below (see table 2).
The abdomen and pelvis are defined separately.
Extremities are divided into upper and lower, with a further subdivision of each into more specific regions. Hip fractures are separated from other lower extremity fractures as they usually affect different populations from other injuries as presented in example 3 below.
Some conditions could not be associated with a specific body region. These included injuries that could occur at one of two or more sites, injuries to multiple sites, or injuries that are systemic.
Earlier versions of the matrix placed codes referring to one of two or more sites where injury was most likely to occur (priority codes). In the final matrix it was decided to create rows of “other” or “unspecified” by body region (at the general matrix level), for example, other and unspecified head and neck. These rows provided a suitable place for most of the priority codes.
Codes describing multiple injuries or indistinctly defined injuries, not in the same body region, were placed in separate rows named “other and multiple specified” sites or unspecified.
Systemic injuries appear in the last row named “system-wide conditions”. These include: foreign bodies entering through orifice, early complications of trauma, late effects of injuries, poisoning and toxic effects of substances, and other and unspecified effects of external causes. This last separation enables easy use of the matrix for analysis of trauma registry data which excludes cases with non-traumatic injuries based on the recommendations of the American College of Surgeons,8 in which diagnostic injury codes between 800 and 959.9 only are included.
ICD-9-CM codes for adverse effects (995.0–.4, .6–.7, .86–.89) and complications of surgical and medical care (996–999) are not included in the matrix. This is consistent with the omission of comparable external cause of injury codes (E codes) from the injury mortality matrix developed by Centers for Disease Control and Prevention.9
Patient characteristics for casualties with TBI by TBI types
Body region of spine and back injuries by spinal cord and vertebral column; values are number (%)
In all, the matrix displays 12 nature of injury columns and 36 body region rows placing each ICD-9-CM code in the range from 800 to 995 in a unique cell location. Each cell includes the codes associated with a given injury. Initially, the matrix was developed on five digit ICD-9-CM codes which are in use in the Israeli trauma registry and in the US National Hospital Discharge Survey (NHDS). Modifications have been made and a four digit version of the matrix is now available upon request from authors. This four digit matrix will be useful for analysis of multiple cause-of-death data (using codes from ICD-9) or in places where the fifth digit from ICD-9-CM is not recorded.
APPLICATIONS
Data presented in this paper are from the Israeli national trauma registry, and from the US NHDS. Included in the trauma registry are all casualty admissions to hospital, emergency department deaths, and transfers to another acute care hospital at eight of 23 trauma centers in Israel. As these centers include all level I centers in the country, it is assumed that they cover over 70% of the severe trauma in Israel. Data presented includes records from 1 January 1997 to 31 December 1999, a total of 47 692 patients.
Data are also presented from the US NHDS for 1998 and 1999. NHDS data are for discharges from non-federal short stay general hospitals. Because repeat hospitalizations for the same injury cannot be separated in this dataset, the outcome measure is a hospital discharge and not a person.10 For 1998–99, there were a total of 3.6 million discharges with a principal diagnosis of injury.11 To analyze the Israeli data, a SAS computer program was written which reads all assigned diagnoses (up to 10 ICD-9-CM codes) in the medical record and updates the counts in the matrix cells. When using multiple diagnoses, persons with a specific type of injury are counted, even if they have other injuries as well. This point is a central concept in the matrix application for data analysis, and will be described in detail in a separate paper.
To analyze the United States data, a SAS computer program was written to read a single diagnosis (the first listed or principal diagnosis). The SAS statements can be found on: http://www.cdc.gov/nchs/about/otheract/ice/barellsas.htm.
An injury of interest may be defined by a cell, a combination of cells, a row (for example. casualties with eye injuries), a column (casualties with a fracture regardless of site), or any combination thereof. The matrix can be used to identify common patterns of injuries in different circumstances, such as head-on motor vehicle crashes, falls from height, etc.
Additionally, the matrix can be used for reporting injury statistics, as is done in the US with hospital discharge data or from trauma registry data as done in Israel.
RESULTS
Figure 1 presents the final matrix reduced to fit into the pages of this journal. A PDF format of the full scale matrix can be found on the internet12 or by mail from the authors. The results presented below demonstrate how several of the decisions were made during the matrix building process:
1. Rationale for the separation of TBI types
Table 1 presents several characteristics of Israeli patients with TBI. The table shows the differences between three mutually exclusive groups—those with ICD-9 codes indicating type 1 TBI, those with codes indicative of type 2 TBI, and those with codes suggesting type 3 TBI. Thirty per cent of type 1 TBI had a life threatening injury (injury severity score 25+) compared with 1.3% in type 2 TBI and 1.2% in type 3 TBI. Type 1 TBI patients have higher inpatient death rates (13.3% v 0.3% in type 2 v 0.2% in type 3), and longer intensive care unit stays (four days, two days, and one day, respectively). Ages were also found to be different between the groups, the median age being 25 years in type 1 TBI, 10 years in type 2, and 3 years in type 3. Preliminary results are presented in detail in separate papers.13,14
2. Variability in body region injured by spinal cord injuries and vertebral column injuries
Table 2 presents US data cross tabulating injury region (cervical, thoracic/dorsal, lumbar, sacrum-coccyx, and other) by type of back injury (spinal cord or spinal column). Spinal cord injuries are most often cervical (54%) while vertebral column injuries were usually (47%) lumbar, further justifying the distinction. The matrix, therefore, makes the differentiation between cervical, thoracic, and lumbosacral injuries both to the spinal cord and to the vertebra.
3. Separation of hip fractures from other lower extremity fractures
Table 3 presents various characteristics of patients with hip fractures and those with other lower extremity fractures. The results show that 95% of hip fractures are caused by falls compared with only 50% in other lower extremity fractures. Hip fracture patients are predominantly female (69%) compared with 37% with other fractures. They are also older (79 v 34 years) and stayed in hospital longer (9 v 5 days). Therefore, a decision was made to keep these patients separated by the matrix so they could easily be excluded from studies concerned with more general trauma.
Characteristics of patients with hip fractures and other lower extremity fractures
Diagnoses frequency
Based on the matrix presented in fig 1, table 4 presents the frequencies and per cent distributions of diagnoses recorded in the Israeli national trauma registry during the three year study period, as well as the distributions from the US NHDS for 1998–99. To simplify the presentation, only the first listed diagnosis is used in this figure, and it presents data at the least detailed standard row level. As one would expect, distributions seen from the Israeli trauma registry data are different from the distributions seen in the NHDS data, primarily because the populations served differ in terms of injury severity.
Frequency and per cent distributions of first listed diagnosis by matrix cells (most general level)
The matrix is useful for highlighting differences. For example, it shows that the Israeli trauma registry have more than twice the proportion of head and neck injuries compared with discharges in the NHDS (36% v 17%) and head and neck injuries are more likely to be internal organ injuries in the Israeli trauma registry than in the NHDS (58% v 42%).
DISCUSSION
The Barell injury diagnostic matrix described in this paper is a framework that can serve as a practical tool for standardizing injury diagnosis data. ICD-9-CM codes are arranged by the nature of injury, meaning that any attempt to gather all injuries to a certain body region involves collating codes across sections within the chapter headings. By using the matrix, this selection is predefined and standard, enabling comparisons across time or place. The major concept behind the matrix's construction was that most injuries can be accounted for by a list of 12 injury natures. Organizing these by body regions produces a useful tool.
The construction of the matrix was an iterative process that took five years, from the initial presentation of the idea, to the final approval at the ICE on injury statistics. One of the more difficult decisions had to do with the definition of TBI. Because the Centers for Disease Control and Prevention already had a TBI surveillance definition in place,7 discussions took place over many months. Currently, the matrix does not partition or tabulate TBIs by severity (that is, mild v severe). This is one of the issues that will be considered in future refinements of the matrix.
Key points
-
The Barell body region and nature of injury diagnosis matrix standardizes data selection and reports, using a two dimensional array (matrix) which includes all ICD-9-CM codes describing trauma.
-
The matrix can be used to characterize the patterns of injury using a manageable number of clinically meaningful diagnostic categories and to serve as a standard for casemix comparison across time and place.
-
The matrix introduces some new ideas such as the separation of traumatic brain injury into three groups.
-
The matrix has the potential to serve as a basic tool in the epidemiological clinical analysis of multiple injury diagnosis data.
-
This paper presents stages in the development and the major concepts and properties of the matrix, using data from the Israeli national trauma registry, and from the US National Hospital Discharge Survey.
Another area of discussion and debate has been the placement of injuries to nerve roots. Are nerve roots central nervous system injuries or not? Consistent with early epidemiologic studies of TBI in the US, the Centers for Disease Control and Prevention do not currently include them in their central nervous system definition.7 In the end, injury to brachial plexus (953.4) was included in upper extremities, and injuries to the optic chiasm pathway and visual cortex (codes 950.1–.3) were included in TBI as a nerve injury and not in the eye row.
In regard to spinal cord and certain TBIs, we debated whether to place these in the nerves column or as internal injuries. For example, spinal cord injuries were initially categorized partly in fractures and partly with nerve injuries. In the last matrix update, the ICD codes for spinal cord “nerve” injuries (code 952) were included with internal organ injuries. The reason for the move was that the column for nerve injuries included some, but not all spinal cord injuries (spinal cord injuries with fractures are classified under fractures). Moving them to internal injuries is more consistent with the placement of brain injuries. Thus, the nerve column now includes all nerve injuries except for spinal cord injuries. The latter can be identified through the matrix rows.
The matrix has been built using five digit ICD9-CM codes. This is most important for burn injuries where the fifth digit gives the location of the burn and also for certain head injuries where the fifth digit details the duration of loss of consciousness. Any data system which lacks this level of detail may miss essential information.
FORTHCOMING DEVELOPMENTS
ICD-10 reverses the classification system, and body region becomes the major category, subdivided by type of injury.15 However, the problem of collating codes remains—this time to identify all fractures, all relevant codes must be collated from the S and T sections, which are organized primarily by body region. With the growing use of ICD-10 and in order to be applicable to a wider range of countries, some of which use ICD-10 already, we need to translate this matrix to ICD-10.
The matrix can be used for analyzing both single diagnoses (as with the NHDS) and multiple diagnoses (as with the Israeli trauma registry data). When used with multiple diagnoses it serves as the basis for the development of standard methods for the analysis of multiple injuries and to create patient profiles. The present lack of tools suitable for the analysis of multiple injuries set limits on our ability to correctly analyze injury in populations. Choosing the first listed or principal diagnosis can result in loss of information, as some patients with a specific injury will be excluded if another injury was chosen as their major diagnosis. Most important is the possibility of distorting information on the true physical condition of the casualty, because multiple injuries are often associated with greater severity. This analysis of multiple injuries is seen as a central issue in the matrix concept and will be at the core of the next phase of development.
Acknowledgments
We would like to thank the trauma surgeons and staff from the eight hospitals in the Israeli Trauma Registry. Special thanks to members of the International Collaborative Effort (ICE) on Injury Statistics whose inputs were invaluable to the development of the matrix.
Vita Barell who was the heart and soul of the development of this matrix died last May, leaving us to complete her mission. Vita was a special person, dearly missed for her charm and wisdom. This matrix is named after her.
Footnotes
↵* Injury to the head that is documented in a medical record, with one or more of the following conditions attributed to head injury: observed or self reported decreased level of consciousness, amnesia, skull fracture, objective neurological or neuropsychological abnormality, or diagnosed intracranial lesion.7
-
↵* Vita Barell died in May 2001.
Linked Articles
- Original Article