Article Text

Abstract
Objectives: Government reports on violence in developing countries are almost universally based upon police data, which are typically incomplete and unreliable. Violence in Karachi was evaluated using ambulance service, not police, records.
Setting: Karachi, Pakistan.
Methodology: The study was based on a case series of persons suffering from intentional injuries and transported by Edhi, the largest emergency service in Karachi, between October 1993 and January 1996. Main outcome variables were injury and death rates.
Results: Edhi Ambulance Service transported 4091 intentionally injured persons during the 29 month period from October 1993 to January 1996. Ninety five per cent (n=3864) were males; 74% (n=2823) were 20 to 40 years of age, and 2400 (58%) died before reaching the hospital. Firearms were the most common mode of injury (n=3396, 83%). Forty six per cent (n=1828) of violent injuries occurred in four neighborhoods of Karachi—22% in Korangi (n= 884) and 8% each in Orangi (n=337), Malir Colony (n=307), and Nazimabad (n=300). On the 32 days when a political strike was called, more people were injured (mean = 10.4 v 5.0 persons, p=0.01) and killed (mean 6.6 v 3.9 persons, p<0.01) compared with days without a political strike.
Conclusion: Violence is a major public health problem in Karachi, affecting predominantly wage earners. At least some of the violence is rooted within the political system. Detailed study of the causes of violence that explains the role that political and ethnic tensions play, may suggest strategies to lessen the toll of violence.
- violence
- Pakistan
- ambulance service
- penetrating wounds
Statistics from Altmetric.com
Worldwide, violent injuries are the eighth leading cause of death.1 Violence is particularly concentrated among adolescents and young adults and has become the leading cause of potential years of life lost in most countries.2 Homicide comprises the second highest number of deaths for people between the ages of 15 and 24 years and is the leading cause of death among African American youth in the United States.3 In El Salvador, a developing country, political violence was the leading cause of death among adults in 1986; males aged 15 to 24 were the most affected, with a homicide rate of 144.4 per 100 000 population.4
In Pakistan, and throughout most of the world, violence is envisioned as a problem to be addressed through law enforcement.5 With the criminal justice system serving as society's bulwark against violence, the primary interventions have been deterrence and incapacitation, that is, to apprehend and penalize persons after they have committed a violent act.6 An alternative for understanding community violence and developing interventions is a public health model. This enables health professionals to study violence from the perspective of agent, host, and environment.5 As a first step, data describing the problem are needed. Currently such information is limited.
The 1992 Pakistan Demographic Survey, found “accidents, poisoning and violence” to be the second most common cause of death between 15 to 39 years.7 However, this national survey does not provide any figures about the number of violent deaths or injuries in Pakistan's major cities, like Karachi. Police crime statistics and crime survey data are known to be poor indicators of the level of violence in society.8–10 There has been no study comparing official crime data with other records sources in Karachi. In a comparison of police reports of road traffic accidents with ambulance service records, police records underestimated serious motor vehicle injures by 21 times and under-reported deaths by 44%.9 Due to the involvement of the state in repressive political violence in many third world countries, official data are generally considered to underestimate rates.4 There is a need for a better data source to understand violence and to characterize it by person, place, and time in Karachi and throughout Pakistan. Thus, we conducted a study to characterize violence in Karachi using records from the major ambulance service in the city.
METHODS
Edhi is a private philanthropic institution that provides, among other services, ambulances to transport ill persons. We selected Edhi's Ambulance Service, as it is the largest ambulance service in the city and covers the entire metropolitan area. Its dispatch centers, supported by 75 working ambulances and 150 drivers, are spread evenly throughout the city.
These ambulances transport the ill or injured to the nearest hospital; they do not provide any prehospital medical care. They also transport dead bodies of victims of injuries. Because the ambulance centers are spread throughout the city, they are the first to respond to most medical emergencies. Telephone hot lines receive calls 24 hours per day. After the ambulance transports an injured person to the nearest hospital, the driver radios information pertaining to the incident back to the head office and this information is handwritten in an open ended format in logbooks. The information includes the person's name, age, sex, type of injury, place where the injury occurred, type of weapon used, persons involved, a general description of the circumstances, destination, and whether the person was alive when they reached the destination. The logbooks do not distinguish persons who were dead when the ambulance arrived, from those found alive or who died on the way to the hospital.
The Edhi Ambulance Service permitted us to photocopy their logbooks and analyze data for the period from October 1993 to January 1996, with a gap of five weeks due to lost records. We translated the log entries into English and the open ended statements were coded to permit analysis. For example, a typical entry might say that a person was stabbed with a knife by his cousin in Korangi and died on his way to the hospital. We would code this as attempted homicide in the area of Korangi, by a family member, with the agent of injury being a knife and an outcome of death before reaching the hospital.
Karachi has an estimated population of 8.2 million10 accounting for approximately 10% of the total population and 30% of the urban population of Pakistan. It is a city of various ethnicities, and in some neighborhoods the majority belong to a single ethnic group. We coded place of the incident according to the area mentioned in the registers. After completion of data entry the areas were grouped together into 41 neighborhoods according to divisions assigned in maps provided by the Karachi Development Authority.
Since the Edhi Ambulance Service transported all emergencies, not just violent injuries, we excluded persons with all other medical causes and non-intentional injuries from the analysis. Violent injuries were defined as “injuries inflicted by another person with the intent to physically injure or kill by any means”. Data were double entered and analyzed in Epi Info.11 We evaluated the frequency of various characteristics and compared the prevalence between groups. For comparison of continuous variables not normally distributed we used the Kruskal-Wallis test.
RESULTS
From October 1993 to January 1996, 4091 persons sustained violent injuries in Karachi and were transported by the Edhi Ambulance Service. Of these, 2378 (58%) died before they reached the hospital. This represents a rate of 23 violent injuries per 100 000 persons per year, and assuming no further deaths after arrival at the hospital, a minimum estimate of 13 deaths per 100 000 persons per year. The mean age of the victims was 30 years with 74% between 20 and 40 years (fig 1). Ninety five per cent were males.

Age and sex distribution of violent injuries in Karachi, Pakistan transported by the Edhi Ambulance Service from October 1993 to January 1996 (n=40910).
The majority of the records did not contain information on the role of either the victim (89%) or the assailant (87%); however 6% (257) of the victims were described as in the process of committing a crime (for example car theft or armed robbery) and 3% (116) were policemen. Similarly, 6% (229) of the assailants were committing a crime, 3% (118) were policemen, and 1% (53) were relatives. Two per cent (91) of the injuries were self inflicted.
Firearms were the agent of injury of 3392 victims (85%), while knives, blunt objects, and bomb blasts each were each used in 3%. This extrapolates to a rate of firearm injuries of 15.9 per 100 000 population and a firearm mortality rate of 9.8 per 100 000 population.
Intentional injuries were concentrated in certain areas of the city, with 1828 (46%) injured in only four of the 41 neighborhoods. The area with the largest number of violent injuries was Korangi (n=884, 22%) followed by Orangi (8%, n=337), Malir Colony (8%, n=307), and Nazimabad (8%, n=300).
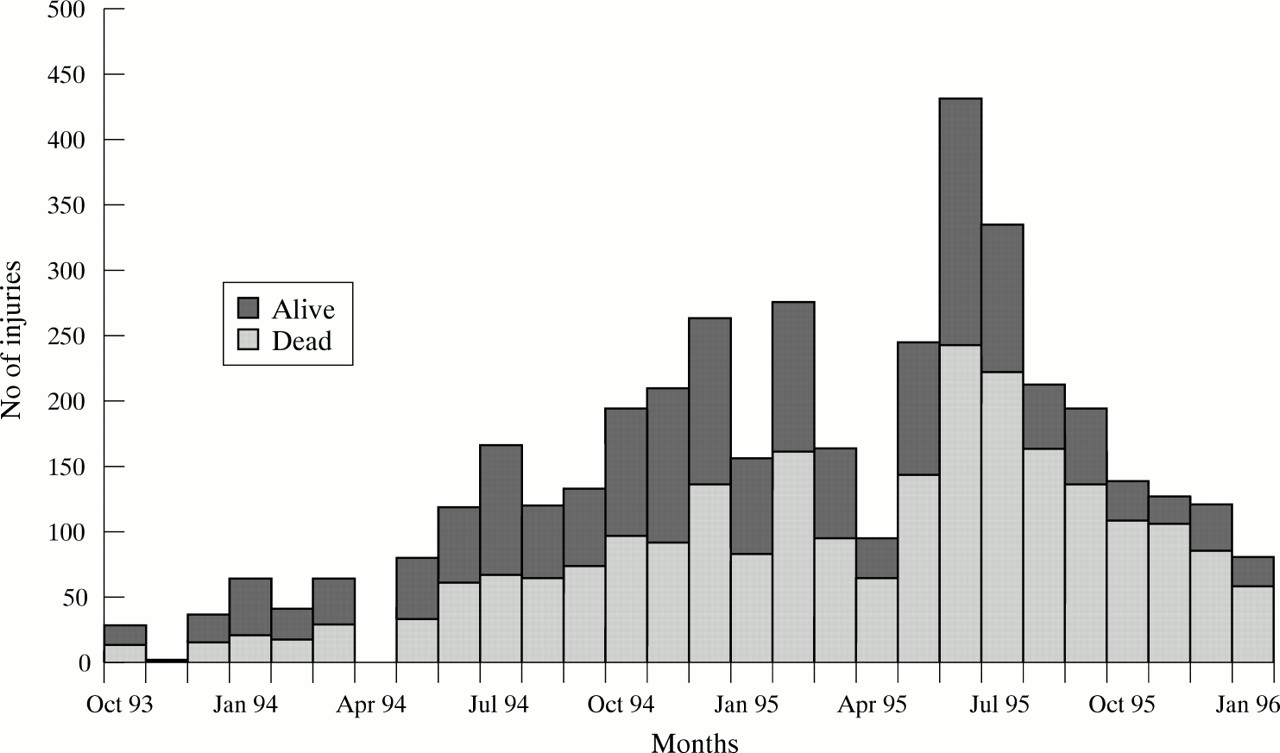
Violent injuries were more common during the daytime and early night-time. The monthly toll increased in 1995 compared with 1994, peaking in June and July 1995 (fig 2).
{kind=link}
{kind=link}
Number of violent injuries in Karachi, Pakistan transported by the Edhi Ambulance Service from October 1993 to January 1996 (n=40910).
During the 26 month period of analysis there were a total of 38 days of political strikes. During these strike days 316 people were violently injured. More people were injured and killed by violence on political strike days (mean 11.7 v 5.9 and 5.1 v 2.9, p=0.01, respectively) compared with days without a strike. Injuries inflicted by firearms were more common on political strike days compared with non-strike days (mean 9.5 v 4.1).
DISCUSSION
As in so much of the world, violence is a major public health problem in Karachi. Violent injuries in Karachi affect mainly young adult males who are generally the principal wage earners of the family. Conservative estimates of the rates of violent injuries (23 per 100 000) and deaths (13 per 100 000) in Karachi were high compared with other Islamic countries like Egypt where the rate of homicide was 1.6 per 100 000.12
On the one hand, Karachi rates were more comparable to the rates of homicides in urban United States in the 1980s (13.7 per 100 000).13,14 However, the 1998 rates of homicides in New York City are less than half the Karachi rates (5.0 per 100 000).15 On the other hand the homicide rate in Karachi is less than cities like Sao Paulo, Brazil (28 to 40 deaths per 100 000)16 or Cali, Columbia where homicide rates are as high as 100 deaths per 100 000.17
Violence occurred in certain areas of Karachi disproportionately. These areas were not in close proximity to each other and were neither unusually poor nor wealthy communities. The ambulance service was not concentrated in these areas; neither were the population in these areas large enough to explain the greater number of homicides. For example, the 1998 census of Karachi showed that Korangi, which accounted for 22% of all homicides, contained 6% of the total city population, while Malir accounted for 8% of homicides and contained only 4.5% of the population. In contrast, the other two areas with high numbers of homicides, Nazimabad and Orangi, each with 8%, had an equal percentage of population (15.5%). One common characteristic among these four areas is that they were all were strongholds of Karachi's major opposition party.
Citywide political and non-political strikes are common in Karachi. There was a significant difference between these two types of strikes. The non-political strikes were strikes organized by labor unions—for example, the transportation union against the government for increasing fuel prices. Political strikes against the ruling government were broader. To ensure the success of their strike, political parties used threats, physical damage to property, kidnapping, or physical harassment to try to bring a halt to normal daily activities. Police tried to make the strike unsuccessful and this often led to armed conflicts. The concentration of the greatest number of violent episodes in neighborhoods that are strongholds of the opposition party, and the increase in violence on strike days, suggests that much violence in Karachi may be politically motivated.
Limitations
There are some important limitations in this study. The Edhi Ambulance Service does not transport all victims of violence in the city, and therefore the rate of violence is likely to be underestimated. Furthermore there is no guarantee that the violence victims transported by this ambulance service are representative of all victims of violence in Karachi. However, ambulance service data would be expected to be substantially more representative than the current alternative, police data, which in other settings of political violence, have been found to be biased.
A second limitation is that the status of the patient as dead or alive was measured too soon to accurately establish the mortality rate. However, even these consistently conservative estimates highlight the substantial health burden of violence in Karachi.
Another limitation is that ambulance workers were able to collect detailed information on the role of victims and assailants in fewer than 15% of cases. These responses are unlikely to be representative of all violent injury victims.
IMPLICATIONS FOR PREVENTION
Efforts to curb violence in Karachi have focused on deterrence and incapacitation. With each new government antiterrorist laws are passed giving extra powers to police. Enormous amounts of resources both in the form of manpower and money are spent to curb violence. This study presents violence as a public health issue and suggests that at least some of the violence may result from political or ethnic conflict. A more detailed study of the causes of violence that explicates the role of political, ethnic, and other tensions, may identify other opportunities where interventions could decrease the burden of violence.
Key messages
-
Altogether 58% of those violently injured die before they reach hospital.
-
The most common weapon used was a firearm.
-
On days of political strikes people were more likely to get injured (mean 10.4 v 5.0 persons, p=0.01) and killed (mean 6.6 v 3.9 persons, p<0.01) compared with days without a political strike.
-
Violent injuries were concentrated in areas of single ethnic and political affiliation.
-
Violence is a major public health problem in Karachi, Pakistan. A more careful study of the causes of violence that explains the part that political and ethnic tensions play, may suggest alternative opportunities where interventions could lessen the toll of violence.
Acknowledgments
The research was supported by the Aga Khan University, Community Health Sciences Department.