Article Text

Abstract
Objective—To estimate the average number of outpatient visits, emergency department visits, and hospitalizations for injured patients.
Methods—The Medical Expenditure Panel Survey Household Component of 1996 is a weighted sample designed to represent the United States population. For each episode of injury the average number of office visits or outpatient contacts, emergency department visits, and hospitalizations were computed. Subsequently the ratio of outpatient to inpatient contacts for each type of injury was estimated.
Results—When asked to report on their medical problems for the previous six months, the majority of respondents who recalled injuries did not report contact with emergency departments or hospitalization. The average injury is associated with only 0.2 to 0.3 emergency department visits. Sports related injuries were associated with 0.03 hospitalizations. Gun related injuries were associated with 0.12 hospitalizations. All types of injury were related with more than one episode of outpatient or office based care. The ratio of emergency department visits and outpatient visits to hospitalizations varies according to the nature of the injury.
Conclusion—Policymakers interested in the cost of injury should account for the extensive outpatient utilization of injured patients.
- injury pyramids
- injury epidemiology
- health services
Statistics from Altmetric.com
The burden of injuries in the United States has been described in terms of deaths, hospitalizations, and emergency department visits and their associated costs to individuals and to society. Approximately $260 billion is spent annually on injury and its consequences according to information provided to the Institute of Medicine for its recent report, Reducing the Burden of Injury.1 In 1995 alone, there were an estimated 62 million acute injury conditions reported to the National Health Interview Survey, 92% of which were medically attended. There were 147 891 deaths, 2.6 million hospitalizations, and more than 36.9 million emergency room visits.2 These figures illustrate an “aggregate injury pyramid”—that is, for every one injury death, there are approximately 18 injury related hospital discharges, and 250 injury related emergency department visits. Aggregate data such as these can be derived from multiple nationally representative data sources, for example, National Hospital Discharge Survey, National Hospital Ambulatory Medical Care Survey, National Health Interview Survey, and are useful in depicting the burden that injuries place on the nation's health resources. Despite the presence of these data, third party payers and firms providing health care face a dilemma in assessing the impact of injuries on the populations they serve. Although it is well known that injuries requiring hospitalization are more severe and more costly, it has been difficult to assess the extent of services required by non-hospitalized patients with injuries. The difficulty arises because the administrative data for injuries that are treated in the outpatient setting seldom include the E codes that would allow the proper classification of the mechanism of injury.3 Diagnosis codes are of some use in classifying injuries such as poisonings and burns, but for injuries such as falls and sports injuries, diagnosis codes are of limited use.
In contrast to the limited availability of outpatient E codes there are many states where all injuries requiring hospitalization are electronically recorded and classified with E codes. In these states, health planners can readily assess the burden of injury in terms of hospitalizations, but can only make rough estimates of the numbers of injured patients receiving care in outpatient settings. Projections based on the ratio of hospitalizations to ambulatory care visits could improve this estimation process and would be possible with better E coding of all medical care encounters. Until universal and uniform E coding becomes a reality, such projections may be improved by analysis of data from the 1996 Medical Expenditure Panel Survey (MEPS). In this paper, we present estimates of the ratios of emergency department and outpatient visits to hospitalizations from this national survey. With these estimates, a health planner could use available data on hospitalizations to extrapolate how many emergency department visits and outpatient visits might be occurring in the population.
Methods
DATA
The household component (HC) of the MEPS was designed and conducted by the Agency for Health Care Policy Research (AHCPR) to provide national estimates of the level of health care use for the purpose of health policy.4 The sampling frame for MEPS is drawn from respondents to the National Health Interview Survey. MEPS-HC uses an overlapping panel design in which there are five rounds of computer assisted personal interviews to collect self reports on medical utilization from households over a two year period. The preliminary release of the MEPS-HC upon which this article is based includes three rounds of data covering 76 602 medical conditions for a sample representative of all ages, genders, and ethnic backgrounds of the United States population. A single respondent in the MEPS dataset may have had zero, one, or a number of medical conditions during the three rounds. A respondent reporting a single medical condition may have reported zero, one, or a number of episodes of medical care for that medical condition. Episodes of medical care were classified and enumerated in mutually exclusive categories as hospitalizations, emergency department visits, outpatient visits, or office based visits. The latter two categories could include items such as medical consultation, radiography, physical therapy, etc. For the purposes of this paper outpatient visits and office visits are aggregated into a single category termed “outpatient visits”.
There were a total of 6320 medical conditions recorded as injuries in the data. The operational definition of injury is based on a subject who received medical care for a condition giving a positive response to the question, “Was the condition due to an accident or injury?”. The MEPS dataset does not record information on health events for which no medical attention was sought. The nature of each injury was recorded by the interviewers as verbatim text which was subsequently coded to fully specified 1996 International Classification of Diseases, 9th revision, CM codes by professional coders. Subjects were asked a series of specific questions to determine whether the injury was related to a gun, a motor vehicle, a poison, a fire or burn, a sports injury, or a fall. For each medical condition the source of care and number of contacts was recorded.
Because the National Health Interview Survey over samples African Americans and Hispanics, sampling weights were produced by AHCPR in order to adjust estimates based on probability of sample inclusion. The weights were designed to reflect a United States civilian non-institutionalized population numbering 265 million. Additional documentation on MEPS-HC is available.4
ANALYSIS
The “SVYMEANs” program from STATA 6.0 was used. We separately analysed emergency department visits and outpatient or office based visits, because the former are thought to be of special interest for cost control. For each injury condition the average number of hospitalizations, emergency department visits, and outpatient or office based events was estimated using the available sample weights, primary sampling unit markers, and strata markers. Confidence intervals were based on estimates of variance that were also adjusted for the weighted survey design.
In order to estimate the ratio of outpatient visits to hospital visits we divided the population average number of outpatient visits per injury condition by the population average number of hospital visits per injury condition. There is no simple way to exactly compute the standard error of a ratio formed by dividing two estimated means. To retain an indication of the precision in the computed ratios confidence intervals for these ratios were formed using the “Box method”.5 In the box method the lower (upper) bound for the ratio is computed as the lower (upper) bound of a 68.4% confidence interval of the numerator divided by the upper (lower) bound of a similar interval of the denominator.
Results
Statistically, the average injury (if there is such a thing) is unlikely to result in contact with a hospital. Overall only four hospitalizations are required for every 100 injury conditions. Only 23 emergency department visits are required for every 100 injury conditions. Office based and outpatient care accounts for most of the treatment of injury with 254 visits required for every 100 injured patients. As stated above, not all of these outpatient visits are routine medical consultations. As more MEPS data are released a finer picture of outpatient injury care will emerge.
Table 1 displays the estimates of utilization for each specific type of injury. Sports related injuries are least likely to result in hospitalization. Gun injuries and poisonings were most likely to result in hospitalization. Episodes of care that were managed completely by telephone were not recorded in the data. Overall, there were only 0.2 to 0.3 emergency department visits for every injury condition. Each type of injury condition averaged more than one outpatient visit, with vehicle related injuries requiring an average of 3.86 visits.
Numbers of injuries and number of provider contacts/injury condition reported in 1996 MEPS-HC
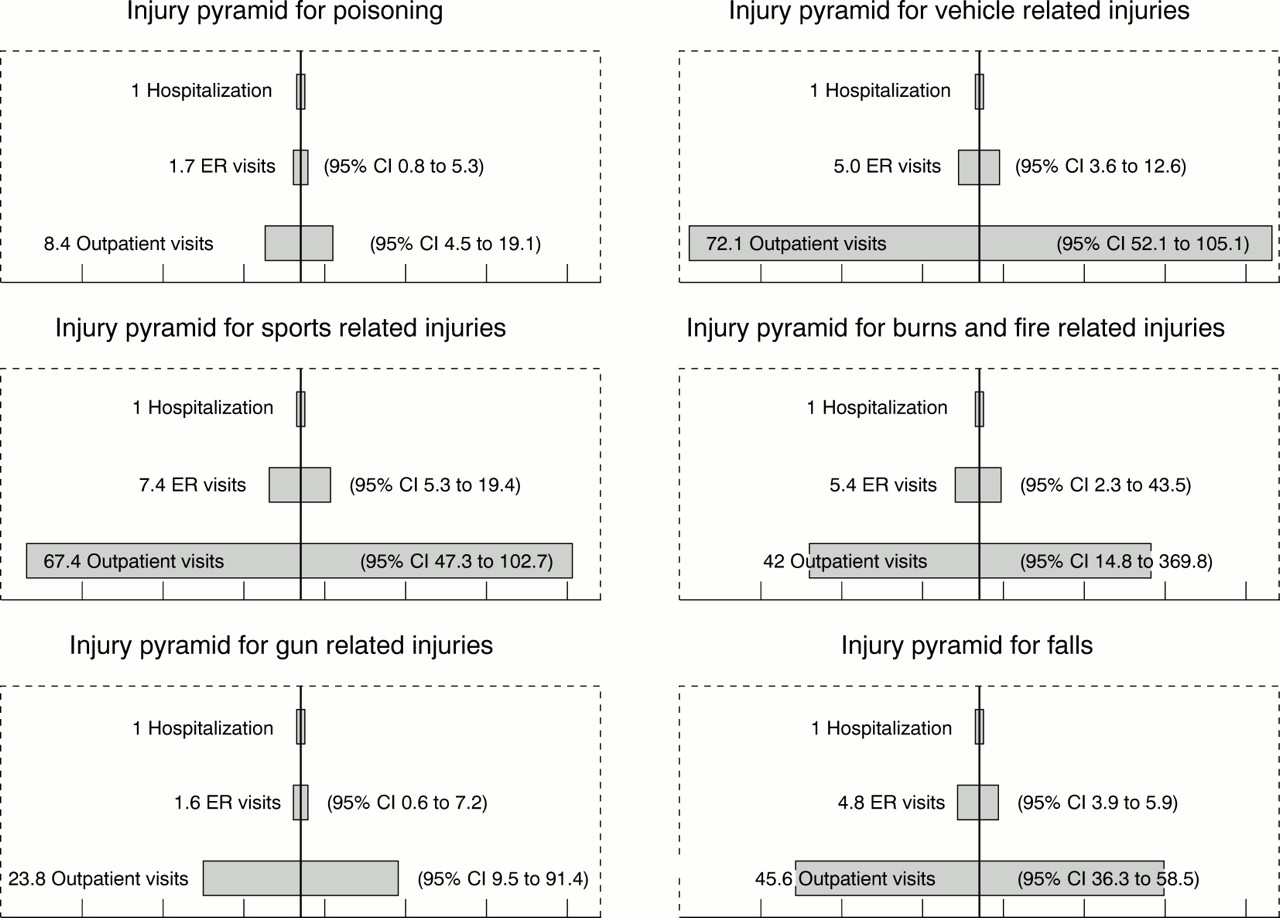
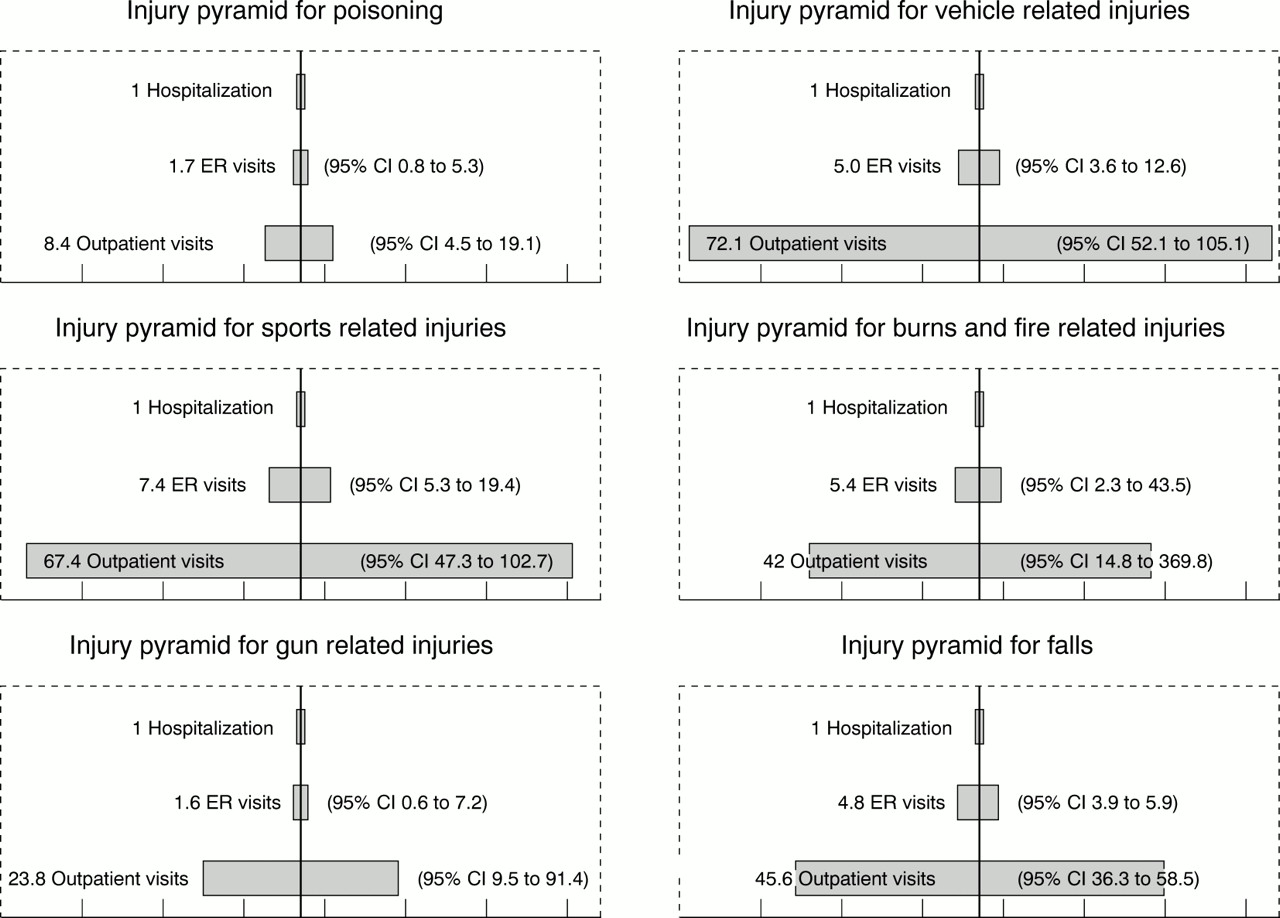
Figure 1 displays the ratios of outpatient care to inpatient care for each type of injury. The figure indicates that in a population every hospitalization is associated with several more episodes of outpatient care. A single hospitalization for a vehicle or sports related injury in a population may be accompanied by close to 70 outpatient visits.
{kind=link}
Injury pyramids for various injury types in the US population based on 1996 MEPS data. Confidence intervals (CI) in parentheses are based on box method (ER = emergency room).
Discussion
The results of this analysis, disaggregated by injury type, can be compared to data aggregated over all injury types based on the National Hospital Ambulatory Medical Care Survey (NHAMCS). A preliminary analysis of NHAMCS data for 1992 only indicated that for every inpatient injury visit there were 13 emergency department visits and 24 ambulatory care visits.6 A subsequent analysis of NHAMCS data from 1992–95 showed that 6.3% of all injuries seen in emergency departments resulted in hospitalization.7 The MEPS data suggest that for specific injuries the proportion admitted can be much higher than the aggregate data show. Furthermore the MEPS data show a far higher number of outpatient visits per hospitalization for most of the injuries considered. It should be noted that because the classification of medical events as injuries relied on the subject's self report, the results here may be skewed by recall bias. Subjects may more readily recall the circumstances for more recent and more serious events.
From a population perspective, hospitalization for injury is the tip of an iceberg. Hospitalization is the most visible to policymakers because administrative data on it are richer. But, by knowing something about the magnitude of outpatient care that may be associated with an episode of hospitalization for injury a more complete picture may emerge.
Given the wider availability of E coded inpatient claims, the costs of hospitalization for E code specific injuries are easier to estimate from administrative data, but are incomplete. Until there is more widespread E coding of outpatient and emergency department claims the full cost of specific injuries to the United States medical system will remain difficult to estimate. The results of this analysis could potentially be combined with estimates of the average cost of an outpatient visit or emergency department visit to assess the full magnitude of costs for injury.
Key points
-
The ratio of office visits to outpatient and inpatient hospital visits is different for different types of injuries.
-
The majority of medical consultations for injury occur in outpatient settings and not in emergency departments and hospitals.
-
Although outpatient consultations are relatively inexpensive, their large volume means that they contribute significantly to the costs of injury.
Implications for prevention
In the United States most episodes of injury that require care are treated in the office or outpatient setting. The average number of emergency department visits for most injuries ranges between 0.2 and 0.3. The average number of hospitalizations for an injury ranges from 0.03 to 0.18. For every hospitalization for injury in 1996, as many as seven emergency department visits and 70 outpatient visits occur. Policymakers interested in the cost of injury should account for the extensive outpatient utilization of injured patients. For example with hospital claims data indicating that a population experienced 100 hospital discharges associated with E codes for falls, a planner might use these results to infer that the population experienced roughly 480 emergency department visits and roughly 4560 outpatient visits related to falls. While the costs of 100 hospitalizations would be quite high, the additional costs of the outpatient care might be a sufficient additional incentive to take steps to control the risks of falling in the population using measures that are known to be cost effective.8 Such an estimate of the outpatient costs would be limited to the extent that there are regional and age related differences in treatment style that would cause a subpopulation to experience a different intensity of treatment from the nationally representative estimates presented here.
Acknowledgments
The authors wish to thank the Maternal and Child Health Consortium and the Johns Hopkins Center for Injury Research and Policy for supporting this research.