Article Text

Abstract
Objective: To outline an approach and agenda for research to prevent injuries to children and adolescents.
Methods: Injuries to children and adolescents 18 years and younger in low, middle, and high income countries were investigated.
Results: A new paradigm for considering injury control research is presented. Research studies are suggested for the areas of etiologic research, intervention research, and outcomes research.
Conclusions: Injuries are an important cause of death and disability adjusted life years lost worldwide. Translation of existing research and rigorous randomized trials are needed to reduce the global burden of trauma.
- etiologic research
- injury control
Statistics from Altmetric.com
Injuries are a global problem in all countries and continents of the world. An estimated 5 million people died from injuries in 2000.1 These injury deaths occurred in high, middle, and low income countries. In high income countries, road traffic injuries, self inflicted injuries, and interpersonal violence are the three leading causes of death among all causes for individuals aged 15–44 years.2 However, even among low and middle income countries, injuries in this age group are exceeded only by HIV infection and AIDS as the leading causes of death.
The burden of injuries is perhaps more apparent when examining the disability adjusted years of life lost (DALYS) due to injuries (table 1). Injuries account for 182 555 000 DALYS, reflecting both the frequency of injuries and the fact that injuries occur more commonly to children and young adults. Worldwide, injuries account for 12% of the global burden of disease.
Deaths and disability adjusted life years (DALYs) lost due to injuries, 2000
The challenge we face is to convince the Bill and Melinda Gates Foundation, The United States Aid to International Development Agency, The Wellcome Trust, and governments around the world of the importance of injuries. These organizations are trying to make a difference in global health, and are doing so by attacking major infectious diseases around the world: malaria, polio, measles, diarrhea, respiratory infection, and HIV. The tools available for addressing these problems are largely available and inexpensive: immunizations, clean water, oral dehydration solution, and condoms. One of the problems for injury control is that we have not done as good a job as we need in developing effective, inexpensive interventions. If a group of injury experts were in a room with Bill Gates, what could they propose to him to prevent injuries to children in low income countries which would give as much return on the dollar invested as immunizing children against measles, polio, or tetanus? I believe that the panel of injury experts would have a difficult time knowing what to say. This is a problem which we must address and correct.
In 2000, 74 000 children under the age of 15 died from war related injuries, accounting for more than half of the intentional injury deaths in this age group.1 The number of injury deaths to children that have been prevented through research and prevention programs in all likelihood pales in comparison to the number lost annually due to war.
CHALLENGES
There are many challenges we face which must, in some way, be dealt with if we are to develop and implement injury prevention programs on a wide scale. The health care systems in many high income countries such as the United States and the United Kingdom, are not working well for anyone, but especially for the poor. The availability of basic health care is a greater problem in low and middle income countries. The downturn in the world economy has exacerbated the problems of the health care system. Other public health problems, such as HIV infection, have long taken priority and new ones, such as bioterrorism, are shifting resources away from injury prevention and control. These problems cannot be ignored and force us, as injury control advocates, to use our resources wisely.
MODEL OF INJURY RESEARCH
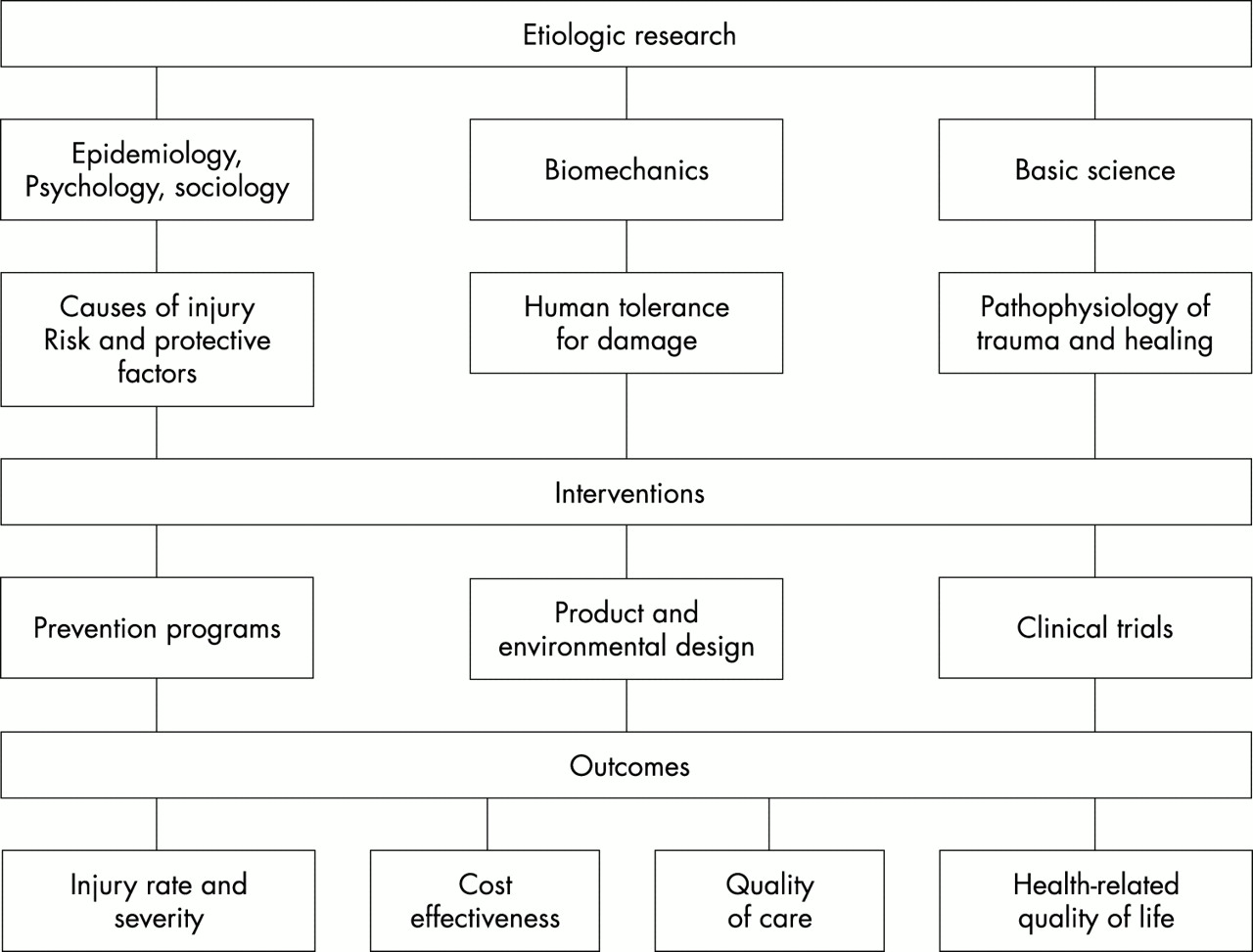
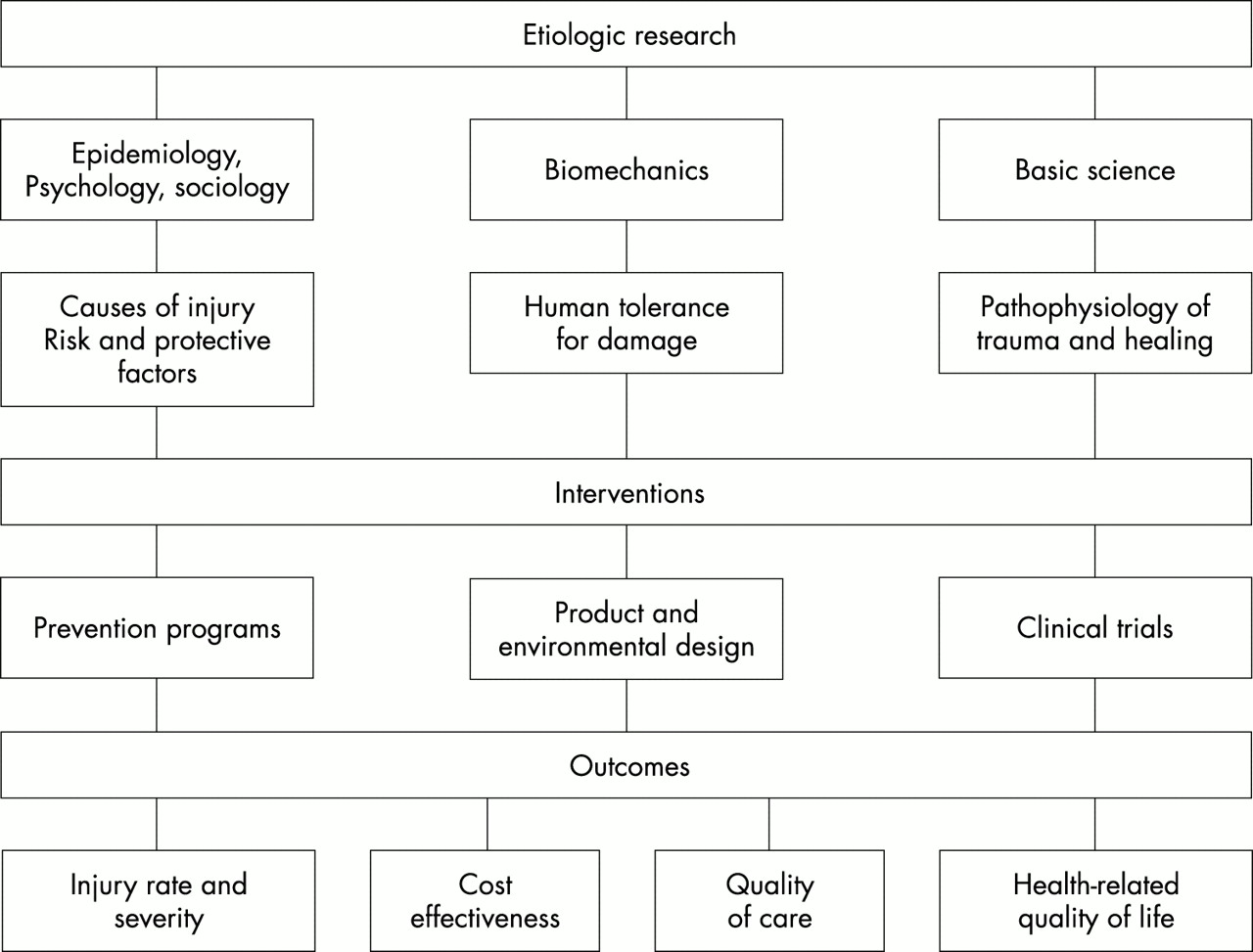
William Haddon 30 years ago proposed his now classic matrix of ways to intervene to decrease morbidity and mortality form injuries.3 This has served the field well and was instrumental in forcing us to view a crash as a separate event from the injuries which result in a crash. I would like to challenge the reader to think about injury research and injury control in a somewhat different paradigm (fig 1).
{kind=link}
Model of injury research.
An important type of research is etiologic: trying to understand the underlying causes of injury to the individual. We can use epidemiology, psychology, sociology, and other sciences to understand the risk and protective factors for injury events. Biomechanics helps us understand the process of energy transfer that Haddon stressed—energy transfer which results in damage to the organism.3 It has guided the development of safe cars and effective helmets and has the potential to be applied to many other injury problems. Basic science research is critical if we are to modulate the body’s response to injury, and lessen the burden from multiple organ failure, shock, and brain injury that are the usual causes of death in trauma patients who make it to the hospital.
The information from this etiologic research, whether it be from epidemiology, biomechanics, or the bench, must be used to guide interventions. These interventions must be evidence based. Interventions at this level can consist of primary prevention programs, product and environment design changes, or clinical trials. When we were able to show that bike helmets decreased the risk of head injury by 85%,4 we were able to develop programs to promote their use.5 Once we have accurate biomechanical data on the tolerance of the body in car crashes, we can design restraint systems for children to prevent them being injured. Part of the problem right now is that we do not have that basic biomechanical data for children in car crashes. Only recently have appropriate sized dummies been developed and begun to be tested in crashes. Once we understand the mechanisms behind wound healing in burns, we can intervene to prevent hypertrophic scarring.6 If we can understand the pathophysiology of head injuries, we can conduct trials of neuroprotective agents to lessen the impact of traumatic brain injury.7
The ultimate goal of these interventions is to have an impact on outcome from trauma, in terms of lower rates of injury, decreased severity of injury, lower mortality, and improvements in functional outcome after trauma among those who survive. Given the limited resources available, interventions must be not only effective but cost effective compared to other strategies.
I will briefly review what I consider to be some of the research and intervention needs in each of these three areas. There are many other topics and areas which could be selected; I am able to comment on only a few given the space available.
ETIOLOGIC RESEARCH
I believe there is little need for descriptive epidemiology. There have now been thousands of reports on the epidemiology of injuries to people of different ages, and in different parts of the world. What is striking is the similarities of injury patterns in different locales rather than the differences. This is true among less industrialized countries as well as among countries in North America and Western Europe. There are likely to be few advances made with the implementation and publication of more descriptive epidemiologic studies of injuries.
We need to move beyond descriptive studies if we are to use etiologic research to guide intervention efforts. One of the biggest challenges is to look at the interactions between the individual child, his or her family, the neighborhood and community in which they live, and the culture of their racial, ethnic, and societal groups. Work by Sampson and colleagues in the Project on Human Development in Chicago Neighborhoods demonstrates how important this interaction is in the etiology of youth violence.8 The social cohesion of the neighborhood and the sense of collective efficacy had a major impact on the rate of violence in the community. Collective efficacy accounted for more than 75% of the variation between neighborhoods in the levels of violence. These types of neighborhood and community variables have never been examined for their correlation with other intentional injuries such as suicide or child abuse, nor have they been examined for unintentional injuries.
The chance to do this will hopefully come with the National Children’s Study, a study of 100 000 children followed from in utero to adulthood currently being planned by the National Institute of Child Health and Human Development. This will be a high quality, national longitudinal study of children, their families, and their environment in which the environment will be defined broadly (chemical, physical, behavioral, social, cultural). It will examine the effect of the interaction on the environment and genetic expression on the risk of various diseases, including injuries, and be a resource for future studies.
In the next few years, we will begin to see the fruits of the Human Genome project. We need to understand what this can tell us about injuries and how to prevent them. Clearly it will give us a better understanding of what the host brings to the traditional epidemiologic paradigm of agent-host-environment. For example, we have long known that individuals who are two standard deviations above the norm for risk taking behavior have lower resting heart rates than individuals with less risk taking.9 Can we understand the biologic mechanisms behind this in such a way that will allow us to intervene with these risk takers to reduce their level of injury?
We also know that about 5% of males in the population account for 50–70% of the crime.10 How does the environment interact with genetics to produce antisocial and violent perpetrators?
The single greatest cause of injuries in children and adolescents is motor vehicle crashes. Since children constitute a minority of those injured in crashes, vehicles are not designed with them in mind. Only recently in the United States, for example, has the National Highway Traffic Safety Administration mandated that crash protection of passengers be tested with child dummies. There is a need for further biomechanical studies to understand the mechanism of injury to children in crashes in order to guide the development of effective restraint systems. An even larger problem is the lack of good biofidelity measures for the available child dummies or computer simulation models.
Biomechanics can be used to better understand other injury problems. For example, Bertocci and colleagues have used computer modeling to understand the forces involved in children falling down stairs,11 information that can be used to differentiate abusive from unintentional injuries as well as design safer stairs. Investigators at the University of Pennsylvania have developed a retractable handlebar to decrees the risk of abdominal injuries in children falling from bicycles.12 Examining bicycle helmets after crashes revealed a large number of impacts to the front rim of the helmet, which, combined with the substantial number of riders with injuries to the forehead, suggests that some helmets, because of poor fit or wearing style, expose the forehead to injury.13 In addition, the data indicated that for a small proportion of injuries, the energy to the helmet may have exceeded design limits. These data can be used to design better helmets. Colleagues at the Harborview Injury Prevention and Research Center are studying the biomechanics of falls to understand the role of shoewear in falls among the elderly. The biomechanics of other injuries should be similarly explored.
Our basic scientists are now molecular biologists and there has been an explosion of such basic research over the past few decades. While we all approach our jobs with the idea that all injuries are preventable, we realize that this is still a distant hope. The most common cause of death and serious disability from trauma is brain injury, accounting for some 80% of trauma deaths to children and adolescents. We currently can do absolutely nothing to treat the primary brain injury; all our intensive care units, emergency departments, and surgeons are focused on preventing secondary brain injury. Our ability to treat this primary injury totally depends on our basic science colleagues’ understanding of what happens at the cellular and molecular level, and deriving new treatments for these injured brains.
Another injury with devastating consequences is burns. Our treatment for these is primitive in the extreme: cutting off good skin from one area of the body and using it to replace burned skin in another area. Surely, we can and must do better in figuring out how to develop truly artificial skin, and how to prevent disfiguring scarring in burn victims. There is tremendous variability in response to injury. For example, fetuses do not scar.6 What is the basis for this and can we turn on the fetal wound healing gene to prevent scarring after burns?
INTERVENTION RESEARCH
How can we translate what has been learned from injury epidemiology, psychology, biomechanics, and molecular biology into effective interventions to prevent injuries or improve the outcomes from trauma? At the US Agency for Health Care Research and Quality, a great deal of emphasis has been placed on translating research into practice: applying what we already know works through prior research to large populations. This is a major emphasis of funders in the US and I expect it is everywhere. The funders want to know how many injuries and deaths have been prevented for what they consider a tremendous investment. At least one-third of deaths and many more non-fatal injuries can likely be prevented with what we know works.14 One of the biggest needs for the field is to determine how to get people to use effective prevention strategies and not engage in risk taking behavior; this requires a great deal more investigation.
There are many examples of interventions known to be effective that should be implemented on a wider scale. Raising the legal age to 21 to purchase alcohol has been associated with significant declines in traffic crashes.15 Many countries around the world have legal purchase ages substantially below age 21. Seat belts are the single most effective strategy to prevent injury in a crash, but use rates show tremendous variation in different countries.16 Primary seat belt laws and motorcycle helmet laws have been associated with substantial reductions in traffic deaths, but many states in the US and many low and middle income countries have not adopted such legislation. Gun availability has been associated with dramatic increases in the risk of suicide,17 but most efforts to restrict access to guns have been unsuccessful.
Based on what is learned from etiologic research, there is a need to conduct rigorous intervention trials. The standard for these trials is a randomized controlled design. These are not easy to conduct and are expensive; nevertheless, many interventions are amenable to be tested with a randomized design. These include community randomized trials for which appropriate methodologies have been developed.18
Some interventions already exist but have not been evaluated, or a randomized controlled trial cannot be done. We need to use the most sophisticated tools we have at our disposable to conduct observational studies to evaluate the effectiveness of these interventions. These include cohort studies to examine the long term impact of interventions, case-control studies to investigate injuries which might be more uncommon, and ecological studies to evaluate the impact of legislation and statewide or country wide programs.
There is also the need to translate biomechanics and engineering studies into interventions and test the real world effectiveness of product and environmental modifications on injury incidence and severity. For example: How do front and side impact airbags affect children in a crash? Will depowered airbags decrease the risk of airbag related injuries? Are booster seats effective in decreasing the injury of children in car crashes? Which devices are most effective for traffic calming and decreasing the risk of pedestrian injuries? How effective are knee and ankle braces in decreasing the risk of injury to high school athletes? Do trigger locks and other methods of safe storage of handguns decrease the risk of Chad and adolescent gun injuries? Can they also decrease the risk of suicide by elderly men?
There is a need for large clinical trials to improve the acute care and rehabilitation of injured patients. Many of these may need to be multicenter studies. One important area is the treatment and rehabilitation of brain injuries. For example, a recent systematic review of rehabilitation of traumatic brain injury found only one small, retrospective, observational study from a single rehabilitation facility to support an association between the acute institution of formalized, multidisciplinary, physiatrist driven traumatic brain injury rehabilitation and decreased length of stay (acute hospital and acute rehabilitation) and short term physiologic (noncognitive) patient outcomes.19 Randomized trials of the timing and intensity of early and acute rehabilitation are necessary.
Other areas such as emergency medical services care should be examined with an eye to challenging existing practices that have not been adequately tested. For example, Gausche and her colleagues in California evaluated the impact of intubation of pediatric patients by paramedics in the field.20 These results indicate that the addition of out-of-hospital endotracheal intubation to the paramedic scope of practice that already includes bag-valve-mask ventilation did not improve survival or neurological outcome of pediatric patients treated in an urban emergency medical services system. Delay of fluid resuscitation until definitive care was available was found to improve outcome of patients with penetrating torso trauma.21 Other such studies are needed.
OUTCOMES RESEARCH
There is surprisingly little outcomes research in the injury field. For example, a recent systematic review of the literature found that, of the thousands of articles published on burns, only 10 reporting on a total of 909 patients included data on return to work, probably the most important component of functional recovery in adults.22 There are remarkably few studies, with the important exception of some landmark studies on traumatic brain injury,23 that have examined the long term functional outcome of children and adolescents after injury. There is little information on whether care in trauma centers does result in better functional outcome in adults than care in non-trauma centers, or for which types of injuries care in trauma centers has the most impact.
Studies in adults indicate that one of the most important factors affecting health related quality of life after injury is the presence of post-traumatic stress disorder symptoms. The effect of post-traumatic stress disorder on outcome is at least as great as the severity of the underlying injury.24 We are only now beginning to appreciate this in children and adolescents. Intervention trials are needed to determine how best to minimize the impact of post-traumatic stress disorder on long term recovery. We know little about the impact of adult injuries on children and adolescents in the family nor on the impact of childhood injuries on parents.
There has also been relatively little work on the cost-effectiveness of interventions and the costs of not doing them. Funders increasingly want evidence that interventions are cost effective. As competition for the health care dollar continues, if not increases, we will need to make a better case for why there should be an investment in injury prevention and control. It is also critical when speaking with legislators. For example, demonstrating to legislators that the cost for the care of unhelmeted injured motorcyclists was mostly borne by the taxpayers resulted in implementation of a helmet law in Washington state, where other strategies based solely on preventing disability failed.25
AN APPROACH
In the inaugural conference for Injury Prevention, Barry Pless, the editor, discussed the difference between multidisciplinary research and interdisciplinary research. In the former, the injury problem is addressed by multiple disciplines, each contributing different areas of expertise. This is not bad and certainly has been successful. But in interdisciplinary research, different disciplines work together, each contributing their own ideas of how to develop new innovations to address injuries. We need much more of the latter.
We also need to conduct our work with a minimum of hubris. In some instances, there are many other people who have something to contribute, and perhaps more, to addressing the problem of injuries. For example, criminologists and sociologists have worked on the problem of violence for a long time. It is academic hubris at its worse to say to them, “Move over. You haven’t been able to solve this problem, but public health can”. We might get a lot farther with less hubris and more interdisciplinary collaboration.
Finally, we need perseverance. There have been large changes in public attitudes and practices, for example, around drunk driving and tobacco use. However, these changes have occurred over decades, not months or years. The injury problem is large but it is also conquerable if we persist in our efforts.