Article Text

Abstract
Background Cohort studies play essential roles in assessing causality, appropriate interventions. The study, Post-crash Prospective Epidemiological Research Studies in IrAN Traffic Safety and Health Cohort, aims to investigate the common health consequences of road traffic injuries (RTIs) postcrash through multiple follow-ups.
Methods This protocol study was designed to analyse human, vehicle and environmental factors as exposures relating to postcrash outcomes (injury, disability, death, property damage, quality of life, etc). Population sources include registered injured people and followed up healthy people in precrash cohort experienced RTIs. It includes four first-year follow-ups, 1 month (phone-based), 3 months (in-person, video/phone call), 6 and 12 months (phone-based) after crash. Then, 24-month and 36-month follow-ups will be conducted triennially. Various questionnaires such as Post-traumatic Stress Disorder Questionnaire, Patient Health Questionnaire, WHO Disability Assessment Schedules, Cost-related Information, etc are completed. Counselling with a psychiatrist and a medical visit by a practitioner are provided accompanied by extra tools (simulator-based driving assessment, and psychophysiological tests). Through preliminary recruitment plan, 5807, 2905, 2247 and 1051 subjects have been enrolled, respectively at the baseline, first, second and third follow-ups by now. At baseline, cars and motorcycles accounted for over 30% and 25% of RTIs. At first follow-up, 27% of participants were pedestrians engaged mostly in car crashes. Around a fourth of injuries were single injuries. Car occupants were injured in 40% of collisions.
Discussion The study provides an opportunity to investigate physical-psychosocial outcomes of RTIs, predictors and patterns at follow-up phases postinjury through longitudinal assessments, to provide advocates for evidence-based safety national policy-making.
- mental health
- epidemiology
- cohort study
- longitudinal
- functional outcome
- quality of life
Data availability statement
Data are available upon reasonable request. Access to data The access to the relevant and confidential data from this study is high on the agenda after satisfying legal requirements, ethical principles and protecting personal privacy. We welcome exchange of ideas on the research, and proposals to add to the study. Those interested can contact Dr. Homayoun Sadeghi-Bazargani (PI). The applications will be reviewed upon approval by the research council and the regional ethics committee of Tabriz University of Medical Sciences. The study website is https://cohortsafety.tbzmed.ac.ir/.
This is an open access article distributed in accordance with the Creative Commons Attribution 4.0 Unported (CC BY 4.0) license, which permits others to copy, redistribute, remix, transform and build upon this work for any purpose, provided the original work is properly cited, a link to the licence is given, and indication of whether changes were made. See: https://creativecommons.org/licenses/by/4.0/.
Statistics from Altmetric.com
Introduction
Longitudinal cohort studies have traditionally permitted stronger inferences than other observational studies,1 and a time-based framework to assess causality and offer the strongest scientific evidence. They have a study population selected by their exposure status, and are mainly beneficial for examining rare exposures and simultaneously multiple outcomes.2 Such epidemiological studies pave the way for translation into appropriate intervention studies using techniques to improve causal inference.
Road traffic injuries (RTIs) account for 41.2 million years of healthy life lost3 and 90% of disability-adjusted life years in low/middle-income countries (LMICs).4 In Iran, RTIs are the second leading cause of death,5 and for 80 000 major traumas yearly.6 Over 2600 person-years of life lost are attributed to RTIs.7 Several recent short-term, narrow-focus cohort studies considered road traffic issues.8–14 However, to fill in the information gap, the research—especially population-based studies—on risk factors for road traffic crashes (RTCs), outcomes and the subsequent evidence-based policy-making to control and prevent them have high priorities. Being costly, the majority of current cohort studies have been done in developed countries, and tailored for their contexts, so did not mitigate the rising rates of mortalities and injuries in LMICs. It is mentioned that environmental factors of trauma survivors may contribute to their vulnerability, emergence and continuation of stress response syndromes.15 16 To our best knowledge, prospective cohort study with long-term follow-ups and large sample of road traffic injurers are rarely conducted especially in LMICs.
Paucity of adequate comprehensive studies of health profile of people involved in RTCs at national and subnational levels is sensible reason to inaugurate a cohort study.17 It was integrated as part of the nationwide cohort studies titled Prospective Epidemiological Research Studies in IrAN (PERSIAN, in 2014) and comprehensively seizure lifestyle and environmental exposures affecting development of non-communicable diseases.18 The PERSIAN Traffic Safety and Health Cohort (hereinafter is referred to as PTC, in 2019) includes two major parts—precrash cohort and postcrash cohort (PTC-POC).19 The former briefly studies factors associated with incidence and prevalence of RTCs and RTIs. The latter was designed to analyse the human, vehicle and environment factors as they relate to all postcrash outcomes at three levels (prehospital, hospital, follow-ups). Accordingly, the main research questions of the PTC-POC are formulated as following:
How is the occurrence and status of post-traumatic stress disorder (PTSD), quality of life, disability and depression at short-term, midterm and long-term run after road traffic crash?
What are the demographic, injury-related and crash-related predictors of PTSD, quality of life, disability and depression at short-term, midterm and long-term run after road traffic crash?
How is the virtual driving performance and safety-related behaviours of RTI victims at short-term, midterm and long-term run after road traffic crash?
We hypothesise that the demographic, injury-related, crash-related and potential predictors independently affect crash consequences as well as the driving performance and safety-related behaviours at short-term, midterm and long-term after crash.
Furthermore, national extension of the cohort study is developed at postcrash level. Throughout the country, five candidate universities evaluated based on preliminary conditions such as being equipped with injury/trauma registry systems will begin data collection in 2022. They will be obligated to accomplish a limited package for at least 200 injurers annually. The current article presents the methodology and profile of PTC-POC study thoroughly.
To summarise, the main reasons for developing this epidemiological long-term prospective study at national level can be briefed as follows: The study
Determines the occurrence and status of PTSD, quality of life, disability and depression at short-term, midterm and long-term run after road traffic crash.
Determines the demographic, injury-related and crash-related predictors of PTSD, quality of life, disability and depression at short-term, midterm and long-term run after road traffic crash.
Determines the virtual driving performance and safety-related behaviours of road traffic injury victims at short-term, midterm and long-term run after road traffic crash.
Pays specific attention not only to the causality and clinical associations but also to the current conditions and procedures.
Recognises potential targets for studies on tertiary preventions of persistent adverse conditions post injury.
Advocates for evidence-based road safety policies, and evidence-based interventions to promote culture change in current national policies.
Provides scientific evidence on considerable importance of postinjury era to convince national policy makers.
Properly allocates fund and resources to RTC-related projects and data sharing.
Materials and methods
Study design
This prospective postcrash cohort study was designed to analyse factors of human, vehicle and environment as exposures relating to outcomes postinjury such as quality of life, type/severity of injury, disability, death, property damage and driving behaviours. We used the Strengthening the Reporting of Observational Studies in Epidemiology cohort reporting guidelines.20
Study setting
This study is carried out in the city of Tabriz, northwest of Iran (1 600 000 residents). Given that the city of Tabriz indicated RTCs among the 10 leading burden of diseases, it was a suitable area for conducting road traffic cohort studies.21 Together with following the PERSIAN cohort protocols, the data collection were performed in PTC-POC so as to examine the hypotheses.
Moreover, a Road Traffic Injury Research Center (hereinafter is referred to as the Centre), has a key intersectoral national role on road safety promotion as well as good capacity and experience at regional and international levels. It is equipped with a Traffic Safety and Health Clinic and a laboratory to examine physical/mental health and driving performance. There are two referral trauma centres equipped with Integrated Road Traffic Injury Registry System (IRTIRS) and provide the preliminary information.
Study participants
The population-based PTC-POC is principally drawn from two sources. One source is comprised people involved in an RTC and registered with the IRTIRS running in two referral trauma centres, from September 2019. The other source contains people who were sampled in the population-based precrash cohort and later experienced an RTC. They will be included regardless of the place of collision and hospitalisation. The study includes both genders at all age groups with any consequences. The inclusion and exclusion criteria are as follows:
Inclusion criteria
Referral hospitals:
Hospitalisation for at least 24 hours after RTCs.
Enrolment at baseline and registration with IRTIRS.
Provision of informed consent.
Population-based precrash cohort:
Experience of RTC
Provision of informed consent.
Exclusion criteria
Admission to an intensive care unit with no patient sitters
Discharge prior to registration with IRTIRS (in fewer than 24 hours)
Having no phone number for contact and follow-up.
Death at any time after crash.
To increase participation, incentives such as paying for travel costs to/from the Centre are used. A phone call is made to remind participants of upcoming follow-ups, and providing the online application of questionnaires for those with access to the internet. Regarding the pandemic of COVID-19, a facemask is given for participants. Incentives help increase participation and lessen loss at follow-ups.
Patients and public involvement
The first stage of patients or their data involvement is at the scene of RTC. They are recorded by Emergency Medical Services (EMS) and the Police. The tools are selected and used based on the research project goals, expert panel and researchers direct experiences and scientific literature, as well as the actual experience gained through establishing the IRTIRS.
Patients and public did not directly involve in the design and performance of the study. Indirectly, as they are road traffic victims and physically affected, the related tools and services are provided underlying the study objectives. Patients or their authorised representatives are asked for their informed consent prior to inclusion. Their participation is voluntary.
Through tool-based measurements, patients are asked about the transparency of the questions. Patients indicate the suitable type of visit. At the end of psychiatry visit session, patients are informed of the psychiatrist diagnosis, provided a prescription, and referred if needed. Once papers have been published, participants will be informed of the results through the study website (https://cohortsafety.tbzmed.ac.ir/) and will receive fine points of the study in a news sheet suitable for participants and non-specialist audience.
Study sample size
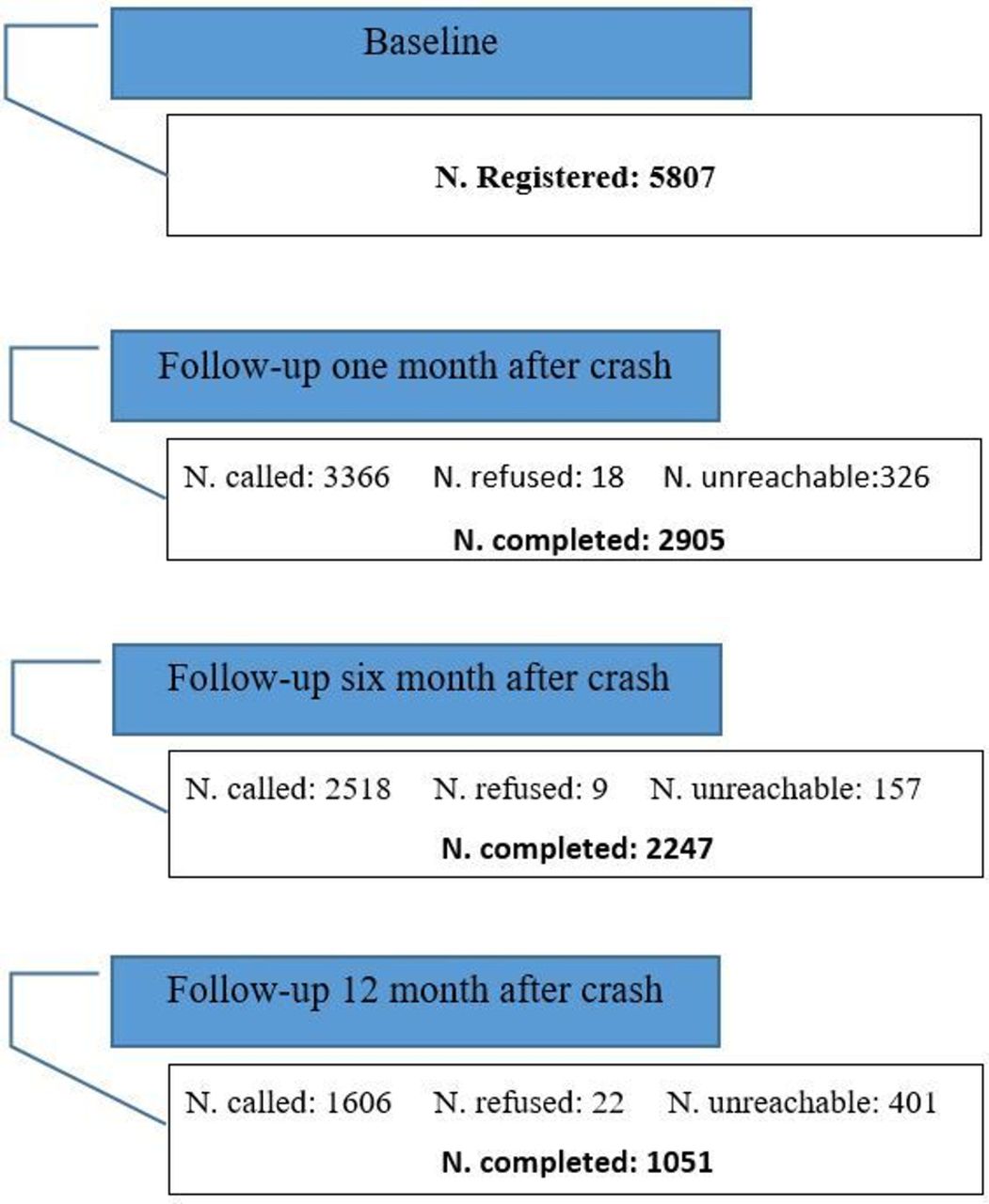
We designed the study to ensure achievement of the correct responses in the most efficient manner. Therefore, we enrol enough RTI patients to provide results with adequate power. However, we would not waste time collecting more than needed. We estimated the sample size based on a pilot data. Regarding the PTSD incidence as an outcome of interest, a sample size of 2824 RTC survivors will achieve 80% power to detect a difference (P1−P0) of 0.0225 using a two-sided exact test (alpha 0.05), and considering a 10% chance of dropout.22 23 Of three of the main outcomes of interest including PTSD, depression and disability, we estimated the highest sample size for the PTSD, so we considered it our underlying sample size. Accordingly, having high coverage rate, and gathering data of 2905 people at 1 month follow-up (F-up1) between 2019 and 2021 (figure 1), it seems realistic to reach the number of 5000 patients at F-up1 from 2019 through 2022, so we scheduled it. F-up1 will then be carried out yearly for 10 000 registered people from 2022 to 2032. The current cohort study is designed to reach a goal sample size of 15 000 at F-up1, over a 13-year period from 2019 onwards.

Flow diagram of Post-crash Traffic Safety and Health Cohort Study, Prospective Epidemiological Research Studies in IrAN, September 2019–March 2020. F-up1 stands for 1-month follow-up, F-up2 for 6-month follow-up, F-up3 for 12-month follow-up.
Study procedures
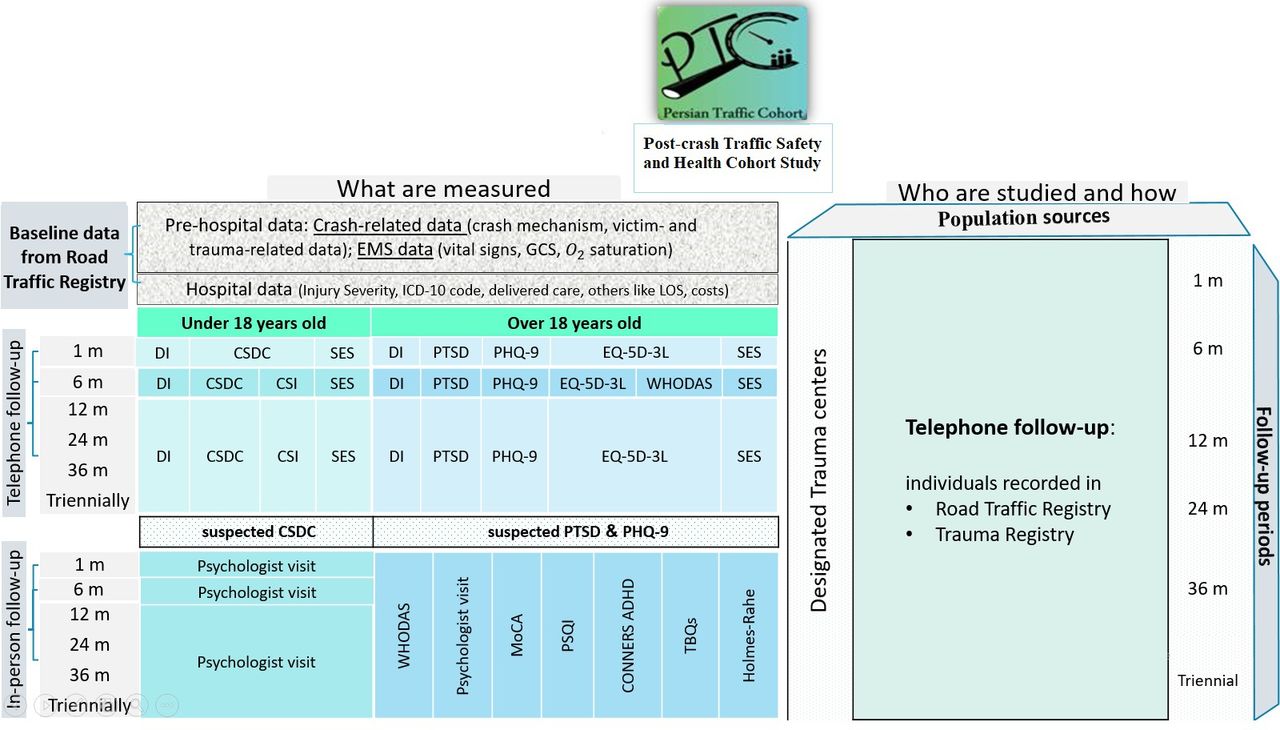
This current study is designed to help understand the occurrence and status of road traffic crashes outcomes, and their predictors as well as patients’ virtual driving performance and safe behaviours at different time spans after crash. The cohort study is based on the IRTIRS data and uses its recorded data exactly.24 The IRTIRS covers two levels of information sources including prehospital and hospital (table 1). The large amount of information at prehospital and hospital levels is recorded in separate and stable sources including the database of EMS, the Police, Hospital Information System (HIS). Moreover, a registry specific tool includes 53 open-ended and multiple-choice items in five groups, which was explained elsewhere.25 Our registry experts administer a face-to-face in-hospital questionnaire to patients. Regardless of this study, the data recording is ongoing.
Measurements at baseline and follow-ups in Post-crash Traffic Safety and Health Cohort Study, Prospective Epidemiological Research Studies in IrAN
Baseline injury data
The prehospital level and hospital level data are called baseline data. The former is about at-scene conditions. The data are routinely recorded after crash and include the Police data (crash-related data such as crash mechanism, victim-related and trauma-related data), and EMS data (vital signs, Glasgow Coma Scale (GCS), O2 saturation) (table 1, figure 2). The latter gathered via the HIS, includes codes of International Classification of Diseases version 10 (ICD-10), relative value unit, vital signs, GCS, O2 saturation, delivered care, surgical code, invasive procedures, pharmaceutical therapy, surgery, length of stay, complications and costs (table 1 and figure 2). In other words, the data and characteristics related to the injury and its severity are provided at these levels of baseline. Injury severity as an essential factor in postcrash studies should be assessed and its effect should be measured on the health-related outcomes. Our approach toward the injury severity assessment is holistic and based on two strategies:
For full coverage of all the enrolled patients, the injury severity will be assessed based on codes of ICD which is considered as surrogate for ISS assessments. This has been shown to have high prognostic value even compared with complex injury severity scales such as TRISS. Various versions of such methodology are available by now and are implemented in trauma settings such as ICISS, CMPMIT-ICD10 and IMP-ICDX.26–28 Moreover, Iran is currently planning to adapt the National Injury Severity Scale focused on ICD coding and triage data. This is done as a project supported by WHO and five provinces of Iran including East Azerbaijan are involved. After finalisation of the national system, the PERSIAN Traffic Cohort will also benefit from it.
For those enrolled participants who have had a crash in Tabriz district and were transferred to hospital by EMS ambulances, a prehospital injury severity assessment is run by EMS and its data can be linked with PTC patient data. The system is providing GAP-O2 scale including assessments on GCS (separately for eye, verbal and movement measurements), capillary O2 saturation, systolic blood pressure and age.
{kind=link}
{kind=link}
Algorithm for Post-crash Traffic Safety and Health Cohort Study, Prospective Epidemiological Research Studies in IrAN. CONNERS ADHD, CONNERS adult deficit/hyperactivity disorder; CSDC, Childe Stress Disorder Checklist; CSI-4, Child Symptom Inventory version 4; DI, demographic information; EMS, Emergency Medical Services; EQ-5D-3L, Europe Quality of Life-5 dimensions-3 levels; GCS, Glasgow Coma Scale; ICD-10, International Classification of Diseases version 10; LOS, length of stay; m, month; MoCA, Montreal Cognitive Assessment; PHQ-9, Patient Health Questionnaire-9; PSQI, Pittsburgh Sleep Quality Index; PTC-PreC, PERSIAN Traffic Cohort-Precrash; PTSD, post-traumatic stress disorder; SES, socioeconomic status; TBQs, Traffic Behaviour Questionnaires; WHODAS, WHO Disability Assessment Schedule 2.0.
Cohort follow-ups
Based on the baseline data, our cohort study begins with follow-ups scheduled to be carried out at 1 month (phone-based), 3, 6 and 12 months (in-person/online video call/phone call) after crash. Then, 24-month and 36-month follow-ups will be steered and continued triennially (table 1). The questionnaires of phone interview are completed by two highly qualified questioners and recorded in IRTIRS. Follow-ups will continue until respondents refuse to participate, can no longer be contacted or pass away. Currently, the first-year follow-ups (1 month, 3 months, 6 months, 12 months), by phone/online video calls are conducted. Our in-person follow-ups are restricted once in a while due to the pandemic COVID-19.
The volume of information related to the follow-ups is stored in a strong, reliable and stable information system, considering pseudonymisation. The information could be linked to the aforementioned databases through an identifier such as national code, for the purpose of various studies or access to information of individuals in other areas. A couple of staff are engaged in data entry, data quality control, and data extraction through this system.
Phone survey
Follow-ups are planned to include all age groups, both gender and all outcomes. Participants registered at baseline are called and followed up to fill partially different sets of questionnaires provided for two age groups:≤18 years (children) and >18 years (adults). A responsible person such as a parent/legal guardian fills out the questionnaires for little children and patients with cognitive disorders. Then, the information received at each stage of follow-ups is entered into the system separately for each follow-up phase (1 month, 6 months, 12 months postinjury). Due to some limitations in some facilities and budget, only the first-year follow-ups are ongoing. The main parameters at F-up1 include acute consequences, at F-up2 include function, quality of life and psychological consequences and at F-up3 consist of long-lasting consequences,19 with appropriate tools (table 1). The selected tools are mostly screening the same parameters at both age categories. At this stage, the mental and physical health consequences of interest for adults encompass quality of life (by Europe Quality of Life-5 dimensions-3 levels), PTSD (by PTSD Screen for DSM-5 (PTSD-5)), depression (by Patient Health Questionnaire-9 (PHQ-9)) and function/disability (by WHO Disability Assessment Schedule 2.0 (WHODAS 2.0)) (table 2) as well as different costs, using questionnaires at short-term, mid-term and long-term postinjury. We use the age-related screening tools, if exist (figure 2).
Conditions of interest in the Post-crash Traffic Safety and Health Cohort Study, Prospective Epidemiological Research Studies in IrAN
The collected data are quality controlled before and after recording in the system. The content is quality controlled by random check and statistical methods such as partial least squares (PLS), convergent and concurrent content validity. Moreover, the quality of communication is checked by the measurement of participants’ satisfaction. Subsequently, we weekly estimate the screening scores of two tools, PTSD and PHQ-9, for all 18+ patients, after phone-based follow-ups. The scores are used to prepare a list of patients demanding a psychiatric visit. Due to some financial constraints and limitations in facilities, only adults are invited to the next stage of study.
In-person survey
In-person follow-ups happen at 3 months after crash for participants at F-up1, and averagely 2 weeks later for participants at F-up2 and F-up3. Main parameters such as patients’ function (by WHODAS 2.0, we obtained WHO’s official allowance to specifically use in this cohort study), recent life stress (by Holmes-Rahe Stress Inventory), cognitive impairments (by Montreal Cognitive Assessment), adult deficit/hyperactivity disorder (by CONNERS’ Screening Scale), sleep quality (by Pittsburgh Sleep Quality Index), traffic behaviours (by Pedestrian Behavior Questionnaire/Manchester Driving Behavior Questionnaire/Motorcycle Riding Behavior Questionnaire), virtual driving assessment on a driving simulator, and psychophysiological characteristics, along with health examination by a specialist are scheduled for in-person visits (figure 2, table 1). As our psychiatry protocol, based on screening scores, patients with psychiatric disorders are examined by a psychiatrist/psychiatry resident through a Structured Clinical Interview for DSM Disorders (SCID) in terms of several disorders (major depressive disorder, anxiety disorder, adaptive disorder, PTSD, alcohol and drug use, personality disorder, mood disorder, schizophrenia or psychosis disorder, and eating disorders). Up to now, only patients aged above 18 years have been invited to in-person visits at the study site. This plan was adopted due to some limitations in facilities and human resources. If they give consent, based on an appointment, they are offered counselling with a trusted psychiatrist/psychiatry resident, and a medical visit by a trusted practitioner provided in office visits. To increase participation, those having trouble with in-person visits due to COVID-19-related conditions, migration, refusal to or inability to come to the Centre, are offered to have psychiatric interviews via online video/phone call (for those without access to the internet). At a later call, the interviewees via online/phone calls are phoned to fill the 36-item WHODAS 2.0.
Our study has two major parts after hospital level, postcrash, namely, follow-ups and psychiatrist/practitioner visits. The former one, is not often affected by the epidemic because it is conducted through phone calls, except for the time of our interviewers’ sick leave. In that case, their work was done by others. The latter one, is conducted in two types as face-to-face psychiatrist/practitioner visits, begun since 20 October 2020. It has largely been affected and temporarily been restricted once in a while due to the Epidemic COVID-19. So that only six people were visited in October and November, in 2020. Next, in 2021, at the time of reduction in incidence and prevalence of COVID-19 cases in East Azerbaijan province, we could invite patients and 17 people visited a psychiatrist/practitioner at the study site. In 2022, five patients have been visited in person, so far. The other type, online/on-phone visit, is performed and provided for patients unable to attend the study site for any reasons. During the epidemic, we could continue the online/on-phone visits much more regularly, except for some weeks in which the activity of such research centres was not allowed according to health protocols on the COVID-19. Up to now, overall 226 patients have been visited via online video/phone calls.
Data analysis
This cohort study considers selection biases such as loss to follow-up bias, length of hospital stay bias, and information biases such as bias in interviewing, bias from surrogate interviews to control and manage them. A variety of variables (with quantitative or categorical scales) are available. We select appropriate types of analysis to control for confounding, to examine subgroups, interactions and regarding missing data. Although statistical methods may vary according to every specific objective developed for each original research based on this cohort, the general statistical methods include measures of central tendency, dispersion tendency, distribution, graphs, correlation and classical regression methods.
In a cohort study, loss to follow-up, missing data and lower statistical power are main concerns to be taken into account using the following methods.
Longitudinal data analysis
As there are repeated measurements in this cohort study, we will use the methods of longitudinal data analysis. The data will be assessed based on data characteristics such as the correlation detail, number of measurements and imbalance of measurements. Accordingly, different methods will be included such as linear mixed effect models, generalised estimating equations (GEE) and covariance modelling in order to handle multiple challenges of longitudinal data. GEE is good for both categorical and continuous data and handle missing data without explicit imputation needed. Irregularly timed data is allowed. Without irregularly timed data, GEE seems more plausible, too, but we have to decide after collecting the data. In GEE, modelling the association between outcomes and covariates, we will use identity link function, logit link function and log link function for continuous, binary and count outcomes, respectively. The estimation method of maximum likelihood and the exchangeable working correlation structures are preferred.
Survival analysis
We may consider time to the event analysis methods including occurrence, reoccurrence and disappearance events.
Structural equation modelling
Having many data from various items and including in analysis, instead of using subscales or total scales, the powerful, multivariate technique of structural equation modelling (SEM) is proper to examine multivariate causal structural relationships of observed and latent variables.
PLS and orthogonal PLS
These supervised modelling techniques as popular methods for multivariate statistical analysis, manage large numbers of correlated variables, offer higher study power, moderate ability in managing missing values, are less prone to threats from multicollinearity and missing values, and predict outcome-related variables from possible predictors. These methods can be applied either for data reduction purposes or non-causality complex association investigations.
Missing data analysis methods
Although some of the above mentioned methods take care of missing data, they are not exact for missing data. We may need specific missing data analysis methods such as inverse probability methods, based on data characteristics, for instance, having wider data set and higher number of fields compared with records. In SEM, full information maximum likelihood would be preferred, otherwise, multiple imputation will be considered depending on the pattern of missingness in our data (monotone, arbitrary) and the form of the imputed variable, as well as the missing data mechanisms (missing at random, missing completely at random).
The analyses will be done using STATA (StataCorp), SIMCA P14 statistical software package (UMETRICS, Umea, Sweden), SAS software V.9.1 (SAS Institute) or other packages in case of necessity.
Preliminary results
Participation
Since September 2019, 5807 registered people have been recruited at baseline. At baseline, the coverage rate is higher than 90%, as participants are at the hospital. Recruitment is ongoing. To date, at F-up1, 3366 people have been contacted. Of them, 2905 respondents (male: 79%; participation rate 58.5%) were successfully tracked. At F-up2 and F-up3, 2247 and 1051 participants were recruited, respectively. Some participants refused to contribute and some were not reachable for any reason (figure 1).
Linking the registered deaths with the forensic medicine database produced 163 deaths that occurred within a month after crash (October 2019–October 2021). Since the registered deaths may be for a variety of reasons, the death report was created based on the forensic medicine database by age and sex (table 3).
Road traffic injury death report over 30 days after crash, 2019–2021
Compared with those who refused or were not reachable, participants at F-up1 were mostly older men (mean age (SD): 41 (15)), married, educated. Participants and non-participants did not differ in terms of job (χ2 (5)=9.2966; p=0.098).
Baseline measurements
The majority of 5807 people registered at baseline had a diploma. Passenger cars account for over 30% of RTCs, while motorcycles account for over 25% of RTCs (table 4). Motorcyclists who injured their pelvis (Coef: 0.29 (95% CI 0.16 to 0.42), p=0.001) and knee (Coef: 0.26 (95% CI 0.10 to 0.42), p=0.001) experienced a lower quality of life.
Demographic and some specific characteristics at baseline and 1-month follow-up (2019–2021)
Passenger cars were involved in about half of RTCs. At baseline, drivers made up almost 50% of victims, followed by passengers/pillion passengers in more than 25% of events. Pedestrians comprised 26% of victims in RTCs. Considering crash mechanism, the most common type was vehicle–vehicle at 43%, followed by vehicle–pedestrian at a rate of about 14% of all collisions at baseline (table 4).
One-month follow-up measurements
Of phone-based F-up1 participants to date, 79% are men (mean age: 39.6 (18–93 years), SD: 16). Around 81% of participants were 54 years old or younger. The largest group was children (38.2%), followed by 25–34 years of age (26%).
Passenger cars were the most common type of used vehicles (35%), next motorcycles (25%). Pedestrians comprised 27% of participants. Most pedestrians (51%) had crashes with one or more passenger cars. The majority of victims were drivers (table 4).
At 1 month after crash, about 40% (CI 0.37 to 0.41) of patients had PTSD at mild (28.6%) or severe (11.6%) levels. In terms of patients’ health, 50.6% (CI 0.47 to 0.51) had no symptoms of depression, but 35.9% of patients were screened with mild/moderate depression, and 13.5% of patients reported severe depression (total score of 15 or above). Regarding ICD-10 codes in chapter XIX, single injuries accounted for 27% of injuries. For chapter XX, car occupants’ injuries occurred in about 40% of collisions. When addressing ICD-10 codes of V0-V7, motorcycle riders and pedestrians were each injured in almost 25% of collisions (table 5).
ICD-10 codes for participants at F-up1 (n=2905; 2019–2021)
In-person psychiatrist/practitioner visit
From October 2020 to January 2022, out of 28, 18 male patients (65%) and 10 female patients were visited in person. We had 21 patients above 30 years old (75%). At 1-month, 6-month and 12-month follow-ups, 10, 7 and 11 patients, respectively, were visited at study site.
Discussion
Methods
This protocol paper provides a profile and methodology of the postcrash cohort study comprehensively. We investigate participants experienced RTCs in terms of PTSD, depressive symptoms, health-related quality of life, socioeconomic status (SES) and function. Formers are examined at three phone surveys and the latter at a 6-month phone survey. We planned to continue follow-ups for 13 years. We carry on four short-span follow-ups through the first year at specified schedules. The phone surveys are at 1, 6 and 12 months after crash. The in-person/online surveys are accomplished 3, 6 and 12 months after crash. Then, two annual and three triennial follow-ups will be completed for survivors. The design was approved after actual experiences published in a study,19 researchers direct experiences and scientific literature. The essential consequences and their measurement tools are discussed later.
Necessity for inclusion of consequences and time in the study
After RTCs, many serious and long-lasting consequences including physical, psychological and social outcomes are often revealed among survivors. PTSD often follows a traumatic event. is associated with functional impairment and poor quality of life, causes major distress or interfere with work or home life.29 The prevalence of probable PTSD among RTC survivors was high (15.4%–26.7%).30 31 RTCs impaired patients’ quality of life and daily functioning.32 33 Mental status of RTC survivors are less examined than their physical injuries34. To prevent psychosocial problems postinjury from becoming chronic, this study follow-ups survivors to screen those with PTSD and depressive symptoms, and identify functional outcomes and SES.
Research specifies time since collision is a significant determinant of PTSD, acute stress symptoms in 6–8 months after trauma,34 and physical disability over time postinjury.35 Based on evidence and a 12-expert panel, the initial time frames were introduced as explained elsewhere.19 F-up1 considers major health outcomes and fatalities occurring at 1-month postcrash. F-up2 reflects the period of retrieval/adaptation to a postcrash health condition.36 The long-term assessment at F-up3 reveals health-related quality of life and SES.
Reasons for selected tools in the study
To provide specific reasons for using some particular tools in screening, the study used Primary Care PTSD-5 because it presents excellent diagnostic accuracy and was broadly acceptable to patients.37 Checking for psychometric parameters of the ultra-brief version tool of PHQ-2, we discovered lack of validity and reliability in phone surveys,19 despite being reliable in in-person survey. Thus depression screening is demonstrated by PHQ-9 which indicated high sensitivity and specificity for diagnosis of major depression and internal reliability (0.89) in a primary care population.38
Health-related quality of life is deliberated using EQ-5D-3L and WHODAS 2.0. The former covers disability-related domains, applicable for different age groups and injury populations, and recommended by a study.37 The latter was designated in ICD-10 and globally applied in function assessment.39 40
The importance of continuity and consistency, the key features of a cohort study, is also considered in the selection of tools. In the long run, the plans should continue. We have only considered children specific screening tools in the current setting, with the available facilities. After the expansion of laboratory equipment and special examinations, in our future plan, children will also be visited by a child psychiatrist/paediatrician.
It is notable that outcomes, mental and physical, of RTCs become more apparent in early months after crash so there is more need to participate at F-up1 by the injured people. However, in the current health system, hospitals provide principally physical health services, and mental health received too little attention. According to the discoveries of the present longitudinal cohort study, major improvements would be defined in the type and way of providing the services for the injured.
Preliminary findings
On the basis of the cross-sectional findings, for baseline (n=5807) and 1-month follow-up data (n=2905), motorcyclists suffered a lower quality of life after crashes in rainy weather and injuries in pelvis and knee. It is consistent with the results of similar studies.41 42 It may be referred to the severity of injury occurred in rainy weather.
The study indicated dominance of male and adult patients, role of driver, passenger cars and motorcycles as used vehicles, passenger cars and heavy vehicles as counterpart vehicles. The crash mechanism indicated vehicle–vehicle and vehicle–pedestrian collisions and rolling over in descending order.43 The majority of the patients suffered from single injuries of head trauma; abdomen, lower back, lumbar spine and pelvis; and knee and lower leg.44
The data presented on the nature and severity of injuries sustained can assist with planning to deal with the postcrash consequences as well as conducting tertiary prevention particularly psychological outcomes.
Conclusion
This protocol provides an opportunity to study physical, psychological and social outcomes postinjury in terms of patterns at each phase, longitudinal assessment and clarification of predictors based on data from repeated follow-ups. A broad variety of subjects enables comprehensive analyses of health trajectories and determinants over life course. The PTC-POC follows the quality control principles considered in the PERSIAN.18 The POC quality control system provides a robust avenue for complete and precise data collection, data entry and generation of databases. Therefore, the designed and planned protocol appears appropriate and performs successfully in conducting a long-term cohort. However, depending on the improvement of facilities or infrastructure, the extension of this cohort study at the national level in other well-equipped universities is part of the plan. In this regard, some of the measurements can also be extended.
Limitations
Due to the limitations in some facilities, and budget constraints, it is not possible to include children in in-person survey. Precision in measuring and visiting a large number of people simultaneously is considerably important, which requires great care. Given the high prevalence of road traffic accidents in Iran, it is expected that the postcrash cohort study will rarely continue too long. However, implementation of such cohort plans may take a long time in countries with low prevalence and low incidence.
As in other parts of life, the COVID-19 pandemic has created immense troubles to running this research effectively, because we deal with injured population who are at risk from exposure to COVID-19.45 The process of implementation in invitation, participation and following related protocols has become more difficult. It seems possible that the authenticity of results would be compromised by the epidemic. Therefore, we are going to examine the agreement between the results obtained from face-to-face psychiatrist/practitioner visits and visits via online/on-phone calls, in patients with two types of visits, in-person and online/on-phone. Also, some tools that have been completed at acceptable intervals in both in-person visits, and online or by telephone will also be explored to discover the agreement of their scores.
Moreover, extrapolating the results of this study to a high-income country should be cautious, considering the supporting infrastructures and overall life style of residents of these countries.
What is already known on the subject
Very few prospective cohort studies have been done on road traffic issues and mainly assessed one or limited dimensions postinjury, limited times of follow-ups and types of data collection, which reached to conclusions tailored for contexts of developed countries with respect to the study population, culture, environment and domestic policies.
What this study adds
The current prospective postcrash cohort study as the first of its kind in the Eastern Mediterranean Region and an all-inclusive study assesses the occurrence and status of health profile elements, along with psychiatric and medical visits, psychophysiological characteristics, virtual driving performance and safety-related behaviours, and the potential predictors of health profile elements are inspected to boast and promote evidence-based consequences on tertiary preventions postinjury.
The study has been conducted at different follow-up phases, and time periods (more than 10 years) postcrash to assess through time status and changes, based on data recorded in Integrated Road Traffic Injury Registry System fed with data from Hospital Information System, Emergency Medical Services and the Police, along with the prospective cohort follow-up data as the core.
How this study might affect research, practice or policy
The study will indicate not only the causality and clinical associations to the status quo and procedures, but also recognise potential targets for studies on tertiary preventions of persistent adverse conditions postinjury and will properly allocate fund and resources to road traffic crash/injury-related projects as well as data sharing.
The study will advocate for evidence-based safety national policymaking, evidence-based interventions to promote culture change in current national policymaking, provide scientific evidence on considerable importance of postinjury era to convince national policy makers.
Data availability statement
Data are available upon reasonable request. Access to data The access to the relevant and confidential data from this study is high on the agenda after satisfying legal requirements, ethical principles and protecting personal privacy. We welcome exchange of ideas on the research, and proposals to add to the study. Those interested can contact Dr. Homayoun Sadeghi-Bazargani (PI). The applications will be reviewed upon approval by the research council and the regional ethics committee of Tabriz University of Medical Sciences. The study website is https://cohortsafety.tbzmed.ac.ir/.
Ethics statements
Patient consent for publication
Ethics approval
This study involves human participants and the Regional Ethics Committee of Tabriz University of Medical Sciences approved the current study (reference number: IR.TBZMED.REC.1398.543) on 19 August 2019. The Research Councils of Road Traffic Injury Research Center, and Tabriz University of Medical Sciences, have reviewed and approved the study design and protocol. Participants gave informed consent to participate in the study before taking part.
Acknowledgments
Authors would like to give special thanks to staff of Integrated Road Traffic injury Registry System assisted with data collection.
References
Footnotes
HS-B and NS are joint first authors.
HS-B and NS contributed equally.
Correction notice The first instance has of RTCs has been updated with the expansion 'road traffic crashes' for clarity. Also, this article has been corrected since it was first published. The open access licence has been updated to CC BY.
Contributors HS-B, MHS and HP were involved in conception and design of the study. HS-B, MHS, HP, SAB-H and MF worked on the validation of project. HS-B, MR and FP involved in software and data curation. HS-B oversaw the execution, supervised the project and acquired funding. IM, SA, ARS-K and AA provided resources. HS-B and NS administered the project, processed the register data, performed the analysis and wrote original article. SAB-H, VS, MG, FP, IM, SA, ARS-K, AA, SA and MF revised the manuscript critically for important intellectual content. All authors worked on interpreting the results and gave final approval of the version to be published.
Funding It is also certified that the prospective project receives financial support of Tabriz University of Medical Sciences, Iranian Ministry of Health and Medical Education (grant number 63795).
Competing interests None declared.
Patient and public involvement Patients and/or the public were not involved in the design, or conduct, or reporting, or dissemination plans of this research.
Provenance and peer review Not commissioned; externally peer reviewed.