Article Text

Abstract
Children are the most frequent victims of dog bites presenting to hospital emergency departments (ED), but there are gaps in understanding of the circumstances of such bites. The objective of this study was to characterise the behavioural circumstances of dog bites by interviewing children ≤17 years (or parent proxies for children ≤6 years) presenting with dog bite injuries to The Children's Hospital of Philadelphia about the bite incident, its setting and associated interactions. Of 203 children enrolled, 51% were <7 years old and 55% were male. 72% of children knew the biting dog. Most bites to younger children occurred during positive interactions, initiated by the child, with stationary, familiar dogs, indoors. Most older bitten children had been active (eg, outdoors), unfamiliar with the dog and not interacting. Whereas face bites predominated (70%) in the younger group (<7 years), bites to extremities predominated (72%) in the older group. Recognition of the two distinctive behavioural and circumstantial subgroups of dog bites that emerged can lead to more effective prevention strategies.
- Bites
- dog bites
- behaviour
- child
- adolescent
- aggression
Statistics from Altmetric.com
Introduction
The public health significance of dog bites is especially relevant for children, who are bitten at a rate more than double that of adults.1 Extant studies have focused on demographic information about the victims and the biting dogs, but presented inconsistent information regarding the behaviours, circumstances, and provocation associated with biting.2–5 In a study of dogs that bit children and were referred to a veterinary behaviour referral centre, the most common stimuli associated with biting familiar children were resource-guarding, and petting, hugging, or other ‘benign’ interactions, while bites to unfamiliar children were most commonly associated with presumptive territorial defence.6 However, that study was limited to a population of dogs presenting to a veterinary referral practice; it focused on the dogs rather than on the victims, and relied on indirect behavioural data (ie, extracted from the veterinary medical record).
Our objective in the current study was to conduct interviews of dog bite victims in a large urban children's hospital to analyse the behavioural aspects of child-directed dog bites as soon as possible after the bite occurred, with a survey instrument similar to that used by veterinary behaviour specialists and geared specifically to obtain information about behavioural circumstances of dog bites. To our knowledge this would be the first such use of a veterinary behavioural assessment of the bite circumstances involved in cases presenting to an emergency department, and would contribute to the literature a unique perspective on the circumstances involved. We thereby hoped to identify risks currently unrecognised in conventionally reported epidemiological studies.
Patients and methods
Subjects
Data for a cross-sectional analysis were collected by prospectively enrolling a consecutive cohort of children ≤17 years presenting for dog bite injuries to the emergency department (ED) of the Level 1 trauma centre at the Children's Hospital of Philadelphia during December 2006 to February 2009. The Children's Hospital of Philadelphia serves Philadelphia county, with a population of 363 615 persons ≤17 years old, and the surrounding area.7 Screening and recruitment occurred between 07:00 and midnight, when research assistants were available. Children and families were enrolled using assent/informed consent and were interviewed prior to discharge. Those admitted to the hospital were interviewed by a research team member or research assistant during their hospital stay. Children 7–17 years old were interviewed directly, with help from parents/guardians as needed. For children 0–6 years old, the parent or guardian was interviewed as a proxy. The study was approved by the Institutional Review Board of the Children's Hospital of Pennsylvania.
Questionnaires/survey instruments
A research team member administered a structured questionnaire and recorded responses on paper. For child and proxy versions alike, additional questions regarding the dog's background were administered when the presenting families owned or lived with the dog. Historical questions were based on a questionnaire used in a clinical veterinary setting, and included training, historical aggression, and historical response to loud noises and separation from the owner.6 Injury severity scores (ISS) were calculated from the medical chart (outpatients) or hospital trauma registry (inpatients).8
Familiarity
To determine the degree of familiarity between the child and dog, subjects were asked whether the dog and child knew each other well (defined as having spent time together at least once per week, for at least the preceding three months), whether the dog lived in the child's household, and whether the subject considered the dog his or her ‘own’. Only those responding affirmatively to the latter question continued with the supplementary questions.
Location
Bites were grouped by location into either indoors or outdoors. In either case, it was determined whether the dog and/or child lived in that location or—in the case of outdoor bites—nearby.
Child–dog interaction and activity
Interaction was identified in several ways. First, subjects were asked an open-ended question about the bite incident. Second, subjects were asked whether the child and dog were doing something together, and specifically whether petting/touching. Finally, subjects were given a list of potential interactions—that is, petting/reaching to pet, hugging, kissing, approaching, restraining, scolding, hitting/kicking, eating/holding food ‘with’ the dog, removing something from the dog, entering a room/yard, walking or running to the dog, crawling to the dog, or ‘other’—and were asked to indicate those that applied. The interactions petting/reaching, hugging, and kissing were grouped as positive or ‘benign’; hitting/kicking, scolding, and hurting the dog intentionally or unintentionally were grouped as negative or ‘aversive’.
The dog's physical position and activity were classified as standing or sitting still, lying down, moving towards the child, or moving away from the child. The activity of children included lack of activity such as sitting or standing, ‘somewhat’ active (eg, walking), and ‘very’ active (eg, running, jumping, or bicycling).
Statistical analysis
Differences in bite circumstances by gender, age, and other variables were examined using χ2 or Fisher's exact tests (2×2 tables) for categorical data and t-tests and non-parametric tests for medians for continuous data. Data within each 2×2 table were analysed as a RR (interpreted as relative prevalence here). Given the large number of variables available, a cluster analysis was conducted to gain insight into how 17 broad variables of interest related to one another (ie, variables that apply to all subjects rather than subgroups). This involved computing a matrix of Jaccard measures of similarity among the variables, clustering the variables with an average linkage function, and plotting the results in a dendogram.9 Stata V.11 was used for analysis (StataCorp, 1998).
Results
A total of 203 children ranging in age from 3 months to 17 years old were enrolled, representing 48% of the 423 children who presented to the ED for assessment of a dog bite over the study period (December 2006–February 2009) and 0.6% of the total 31 455 children who presented to the ED for all injuries during this period (table 1). Thirty-seven breeds, of which 10 were each represented at least four times, were reported among the biting dogs (table 1). Fifty-three (31%) dogs were identified as either purebred or mixed pit bull terriers.
Demographic data for 203 children presenting to an urban trauma centre with dog bite injuries, and for 203 dogs reported to have bitten
Familiarity
In 72% of cases, the child and dog were reported to ‘know each other’ (table 2). Younger children, in particular, were more likely to have been bitten by a familiar dog (table 3). The highest percentage of child–dog pairs who knew each other was 0–2-year-old children (N=37; 88%), compared to 50% (N=13) of children >12 years (p=0.005). Children bitten on the face were most likely to have been bitten by a familiar dog: 49 (50%) lived in the child's home, 39 (40%) lived with a relative or friend, and 4 (4%) lived with a stranger (p<0.001). More pit bull terriers than expected (36%, compared to 14% of other breeds) were unknown to the child (p=0.001; table 3).
Circumstances associated with dog bites to 203 children presenting to an urban trauma centre
χ2 test frequencies and relative prevalence (RP) of variables associated with dog bites to children
Location
In 62% of indoor bites, the child was bitten at home by the family pet (table 3). When outdoor location was known, most (75%) outdoor bites occurred at or near the dog's home, regardless of where the child lived (table 3). Twenty-six (41%) outdoor bites were by uncontrolled dogs (not leashed, restricted to a yard, or otherwise restrained), while 17 (18%) were by tethered dogs who could reach the child or whose tether had broken. In 16 (25%) cases there was a fenced yard, but the dog had left the yard by an open gate, by jumping over the fence, or by other means. The dog's owner was ‘close by’ in 61 (64%) outdoor bites.
Child–dog interaction and activity
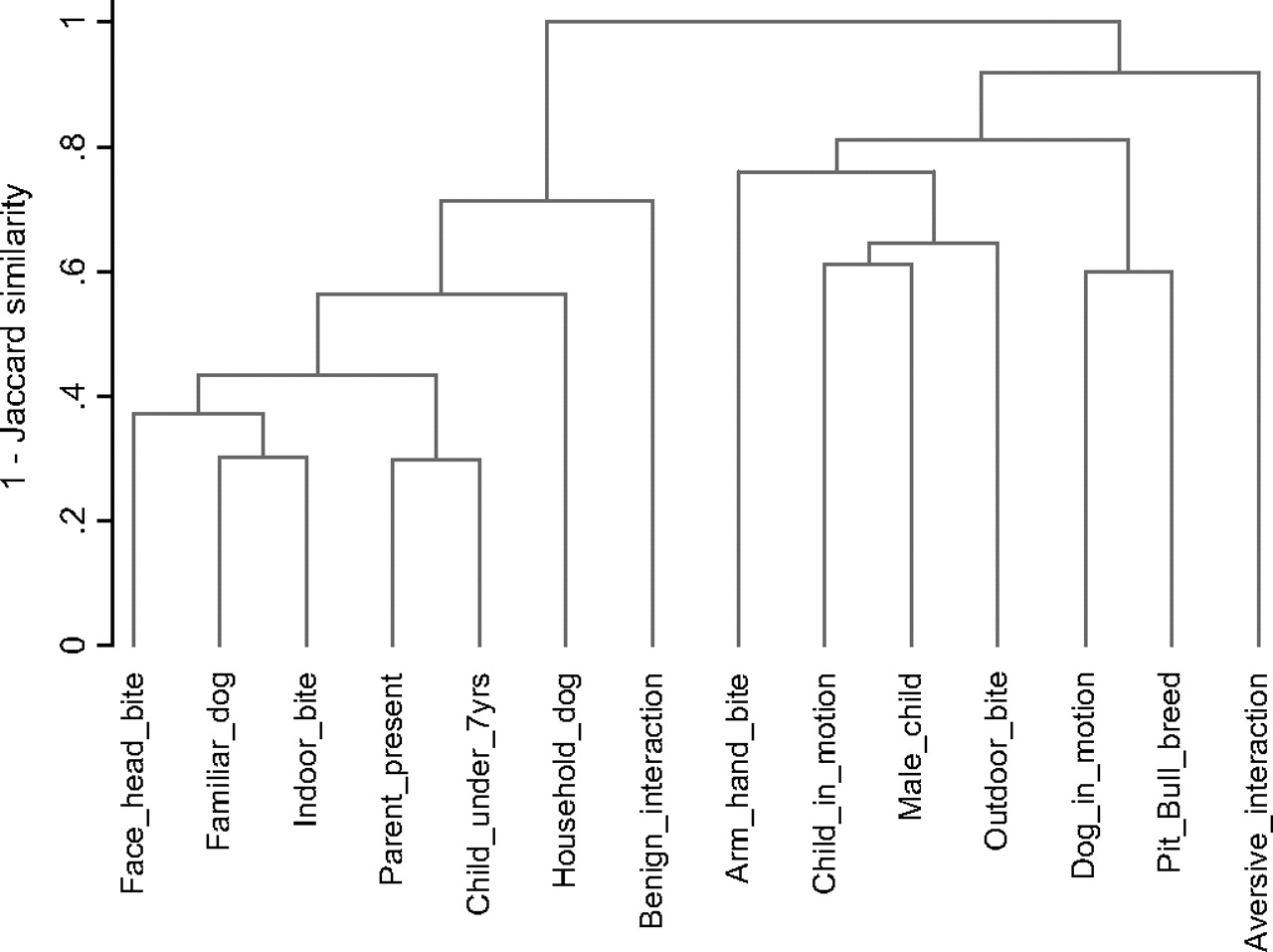
Most children who knew the dog were engaged in some interaction at the time of the bite, while those who did not know the dog were less likely to be doing something together (table 3). There were a number of associations with either benign or aversive interactions (table 3, figure 1). Among other associations, familiarity and being indoors when bitten were most closely related to each other (ie, most often occurred in conjunction with one another), along with the child's age <7 years and the presence of a parent (figure 1).

{kind=link}
Cluster analysis dendogram representing the co-occurrence of dog bite characteristics. The height of bars (ie, measured on the y-axis) connecting variables represents the level of association among variables, with lower values corresponding to greater similarity among clustered variables.
Negative interactions more often involved children over 12 years old (N=8; 31% of this age group) than younger children (N=2, 6% of 0–2 year olds; N=5, 13% of 3–6 year olds; N=6, 8% of 7–12 years old; p=0.015).
Dogs were more often sitting, lying, or standing—rather than moving to or away from the child—at the time of the bite, and face bites were usually delivered by dogs that were lying down (N=31, 42% vs N=16, 22% moving towards the child or N=26, 35% standing still, p<0.001). Younger children were more frequently bitten in the face than were older children (table 3).
An adult was present at the time of the bite in 60% (n=101) of all bites in which this information was reported (not available for 92 (45%) subjects). In the case of bites by household pets specifically, the adult was most often a parent or grandparent (n=68; 60%). Most of the latter interactions involved petting (N=30, 79% of children petting the dog did so in the parents' presence, vs N=8, 21% when parents were not present, p=0.003) which was initiated by the child, and which resulted in a bite to the child's face.
Figure 1 shows that two broad themes emerged through the cluster analysis, where bar height (ie, measured on y-axis) represents the magnitude of association among clustered variables and lower values correspond to greater similarity. Knowing the dog and being indoors when bitten were closely related (ie, often occurred in conjunction with one another), along with being bitten in the face/head. Bites to young children often occurred with a parent present. All these characteristics were associated with being bitten by a dog living in the child's home and being bitten during a benign interaction. The second broad theme involved male children, being bitten outdoors, and being bitten in an extremity. Aversive interactions and being bitten by a pit bull were represented in this theme.
Discussion
In focusing on the behavioural and circumstantial factors associated with dog bites to children who present to a hospital emergency department, two subgroups of behavioural circumstances emerged: those directed to younger children bitten indoors who were familiar with and, in many cases, lived with the dog, and those directed to school age or older children outdoors, to whom the biting dog was unfamiliar. While some basic associations have been reported in previous studies, the broader, behaviour-focused overview that we have gained improves our understanding.2 11 In addition, we note that bites are more likely to occur where the dog lives (either in the dog's home, or in the vicinity of the home in the case of outdoor bites), regardless of where the child lives, and that lack of the dog's activity is associated with indoor bites, while movement towards the child is associated with outdoor bites.
Interactions between the dog and child were common. Those with familiar dogs were largely initiated by the child and were ‘benign’, or positive, as has been noted by others.6 We report that interaction can be quiet or even passive (eg, proximity only), settings in which provocations for dog bites are frequently overlooked or misinterpreted. Verification of such interactions contradicts the common view that dogs bite spontaneously, or that they usually initiate interactions leading to bites.12 We report that the child is more likely to initiate interaction with familiar dogs. The recognition that ordinary or ‘everyday’ interactions can lead to bites13 is an important step towards their prevention.
A parent or grandparent was present in more than half the cases in our study, with increased likelihood when the bite involved a family pet, indoors, with whom the child initiated an interaction—most often, petting the dog. Presence of an adult did not necessarily imply adequate supervision, however, since parents can be unaware of bite risks and therefore less vigilant when the child is being quiet or affectionate with the dog.14 15
Territorial defence appears to be a common motivation for bites to unfamiliar children, often in the absence of interaction, since even (largely unfamiliar) dogs that bit outdoors were at or near the dog's home at the time of the bite.6 Ultimately, however, we recognise that the dog's motivation or ‘intent’ for biting, whether a familiar and interactive or unfamiliar and non-interactive child, can only be inferred.
Education of preschoolers about the potential dangers of interacting with dogs can be helpful,16 but instructions to parents or caregivers are ultimately needed4 and can be simplified into several points. First, dogs that are lying down or stationary should never be approached by children. Second, for dogs, whatever is in proximity—whether edible or not—is potentially a high-value item. Even a parent might be viewed as a high-value ‘resource’ when the dog and adult are together and approached by the child, resulting in resource-guarding aggression.6 Third, even ‘benign’ touch might cause pain (or anticipation of pain) and trigger defensive aggression. Fourth, dogs and humans interpret social and postural signals differently: human affection, such as hugging, can be perceived as a direct threat by dogs.17
Although it was not possible to assess the health of the dogs that had bitten, medical problems such as skin disease or osteoarthritis were common in child-biting dogs that were presented to a veterinary behaviour clinic,6 and should be a consideration in any case of aggression by household pets.
Bites by unfamiliar dogs were likely to involve active children and dogs. Prevention in these cases is at once more straightforward and more challenging, because it depends on control of unrestrained dogs. Public education about restraint of dogs might include warnings that underground electric fencing is not a reliable barrier for either the fenced dog or for neighbourhood children, and that long-term tethering can increase aggression.18 Although adults are ultimately responsible for child safety, school-aged children might be old enough to learn safe habits in the presence of unfamiliar dogs.19 In addition, communities can encourage anonymous reporting of dogs that repeatedly fence-run or escape from yards, or that aggressively bark or lunge at pedestrians, even if a bite has not yet occurred. The use of muzzles for dogs that have bitten historically might decrease the risk of biting when owners are present and the dog is restrained, but would not apply to free-running dogs who are not in direct control by owners.
Having enrolled bitten children at hospital and during certain hours only, the data may not represent all children presenting to hospitals nor the general population of bitten children or biting dogs. Also, because data were obtained by self-report, reliability of dog breed identification (particularly when dogs were not the family's own) and circumstances of bites was limited. The cluster analysis served well as a tool to help synthesise such rich data and identify the co-occurrence of characteristics associated with dog bites. But being a tool for data exploration, the intriguing associations reported here should be used for hypothesis generation rather than viewed as conclusive. Subsequent studies that include control groups are now needed to conduct more robust tests of risk factors for dog bites.
Our study supports the need for preventive strategies which rely on adult knowledge of risks. Younger children, in particular, cannot make their own decisions about safety with dogs, and even adults are often unaware of implicit provocation or risks of biting. In the case of outdoor bites, community and dog-owner awareness of proper restraint is needed. In the case of indoor bites to younger children, separation of the dog from children might ultimately be necessary. We suggest that recognition of differences between the two situations would lead to more effective prevention strategies.
What is already known on the subject
Children are frequently presented to emergency departments for dog bite injury.
Younger children are most likely to bitten on the face and head, by familiar dogs.
Petting, hugging and similar interactions were commonly associated with bites to familiar children, and territory-associated bites were commonly associated with bites to unfamiliar children, by dogs presenting to a veterinary behaviour service.
What this study adds
Behavioural circumstances associated with dog bites to children can be grouped into (a) face bites to younger children by quiet, familiar dogs, largely indoors in the presence of parents, and (b) extremity bites to active school-aged or older children by active, unfamiliar dogs outdoors.
Bites to familiar children are more likely to involve stationary dogs; bites to unfamiliar children are more likely to involve dogs in motion towards the child.
In the case of younger children, interactions are often initiated by the child and involve “positive” provocations such as petting or hugging.
In the case of older children, bites are triggered by the presence of the child in or near the dog's home or neighborhood, even without direct interaction.
Acknowledgments
We would like to acknowledge the support and assistance of Dr Joseph Zorc, Ms Marlena Kittick, and the Academic Associates and staff at the Children's Hospital of Philadelphia. We are grateful for the participation of the children and their families.
References
Footnotes
Competing interests None.
Ethics approval This study was conducted with the approval of the Institutional Review Board, Children's Hospital of Philadelphia (CHOP), Philadelphia, Pennsylvania, USA.
Provenance and peer review Not commissioned; externally peer reviewed.