Article Text

Abstract
Objectives: To examine the association between tobacco smoking and residential-fire mortality and to investigate whether this association is explained by the confounding effects of selected socioeconomic factors (ie, educational attainment and median household income).
Design: An ecological analysis relating state-level residential-fire mortality to state-level percentages of adults who smoke was conducted. Negative binomial rate regression was used to model this relationship, simultaneously controlling for the selected socioeconomic factors.
Results: After educational attainment and median household income had been controlled for, smoking percentages among adults correlated significantly with state-level, population-based residential-fire mortality (estimated relative rate for a 1% decrease in smoking = 0.93; 95% CI 0.89 to 0.97).
Conclusions: Mortality from residential fires is high in states with high smoking rates. This relationship cannot be explained solely by the socioeconomic factors examined in this study.
Statistics from Altmetric.com
Residential fires remain a substantial public health problem in the USA, causing an estimated 3030 deaths, 13 300 injuries, and upwards of US$6.7 billion in property loss in 2005.1 Numerous studies have identified risk and protective factors associated with residential-fire injuries and deaths.2-7 Whereas many of these factors are not modifiable (eg, age, gender, race), some factors are amenable to change. At the environmental level, the presence of smoke alarms can decrease the risk of death in a home fire by up to 50%.8 At the individual level, cigarette smoking is a modifiable behavior with a documented association with residential-fire injuries and deaths.
Smoking is the fourth leading cause of unintentional residential fires6 and the leading cause of residential-fire deaths, accounting for one-quarter of such fatalities.1 5 In 2003, smoking caused an estimated 15 500 residential fires, 690 related deaths, 1330 related injuries, and US$403 million in direct property damage.5 In the USA, approximately one in five adults smokes cigarettes.9 The presence of a household smoker is a risk factor for residential-fire injuries and deaths,10 and an estimated one-quarter of deaths from residential fires caused by smoking occur among persons other than those whose cigarettes start the fires.5 Many residential fires caused by tobacco products start in the bedroom or living room, and the most common items ignited are upholstered furniture, trash, mattresses, and pillows.4
Ecological study designs are appropriate for studying residential fires because they recognize the complex interactions between individuals and their environment. Several studies have shown the ecological association between smoke alarms and residential-fire injuries and death.11-13 To our knowledge, no ecological study has assessed the association between cigarette smoking and residential-fire deaths. The aim of this study is to quantify the association between state-level residential-fire mortality and percentages of adults who smoke, and to investigate whether this association could be explained by the potential confounding effects of selected socioeconomic factors.
METHODS
Data
All study data represent the year 2004. We obtained counts of residential-fire fatalities and population estimates by state from the Web-based Injury Statistics Query and Reporting System (WISQARS).14 This interactive injury mortality database system contains death certificate information filed in state vital statistics offices and includes fire-related deaths reported by attending physicians, medical examiners, and coroners. Residential-fire deaths were identified by International Classification of Diseases 10th Revision (ICD-10) codes X00–X09 and where the place of death was identified as “home.” These external cause-of-injury/death ICD-10 codes include unintentional exposure to smoke, fire, and flames (including toxic fumes). Population estimates were generated by the US Census Bureau collaboratively with the National Center for Health Statistics.
We obtained data indicating the percentage of adults who smoke (by state) from the Centers for Disease Control and Prevention’s (CDC) Behavioral Risk Factor Surveillance System (BRFSS).15 This ongoing surveillance process aggregates health information from state-based telephone surveys about modifiable risk factors related to chronic disease and other leading causes of morbidity and mortality. BRFSS is a random-digit-dial survey of the non-institutionalized US population aged 18 years or older. The survey design and random sampling procedures are described in detail elsewhere.16 17 In 2004, 49 states and the District of Columbia asked tobacco-use questions; Hawaii was the only state with incomplete BRFSS data for these questions. We analyzed the following survey item, “Do you now smoke cigarettes every day, some days, or not at all?”, and defined current smokers as respondents who indicated smoking every day or some days.
State-specific percentages of people with a high school degree or higher (population aged 25 years and older) and median household income (in 2004 inflation-adjusted dollars) were collected through the US Census Bureau’s American Community Survey.18 This is the largest US annual household survey, and its estimates are based on a nationwide sample of about 250 000 addresses per month, or ∼2.5% of the population each year. We chose these potential confounders on the basis of their association with both residential-fire deaths3 19 and smoking.20
Statistical analysis
Data for Hawaii were excluded from the analysis because of incomplete BRFSS results for 2004. The analysis was conducted in two phases. In the first phase, we performed a descriptive analysis of national data. In the second phase, we conducted a negative binomial rate regression analysis to model residential-fire mortality, by state (and the District of Columbia). We used a negative binomial model as an alternative to a Poisson model to accommodate overdispersion in the count data. The rate regression model adjusts for the size of each state’s population by incorporating the logarithm of the population size as an offset term.21 This results in a model of residential-fire mortality rates rather than a model of residential-fire death counts. The main predictor was the estimated percentage of current adult smokers. The rate regression model also included estimated median household income and estimated percentage of adults with a high school education as covariates to control for the influence of socioeconomic status, thereby avoiding an overstatement of the effect of smoking behavior. Using the fitted model, we estimated the relative rate (and 95% CI) of residential-fire mortality corresponding to a 1% decrease in the smoking percentage, controlling for the sociodemographic characteristics. The regression model was fitted using PROC GENMOD in SAS V9.1.3.
Because we had only 50 data points, we were conservative in our inclusion of potential confounders in the regression model. In addition to educational attainment and median household income, we examined further potential confounding by starting with our existing model and including other candidate confounders one at a time. The additional candidate confounders were represented by the following state-level variables: percentage of the population living in rural areas (in 2000), per capita alcohol consumption, and cumulative heating degree days. The addition of these variables to the existing model did not change the main effect (data not shown), and they were consequently excluded from the reported model.
RESULTS
Descriptive analysis
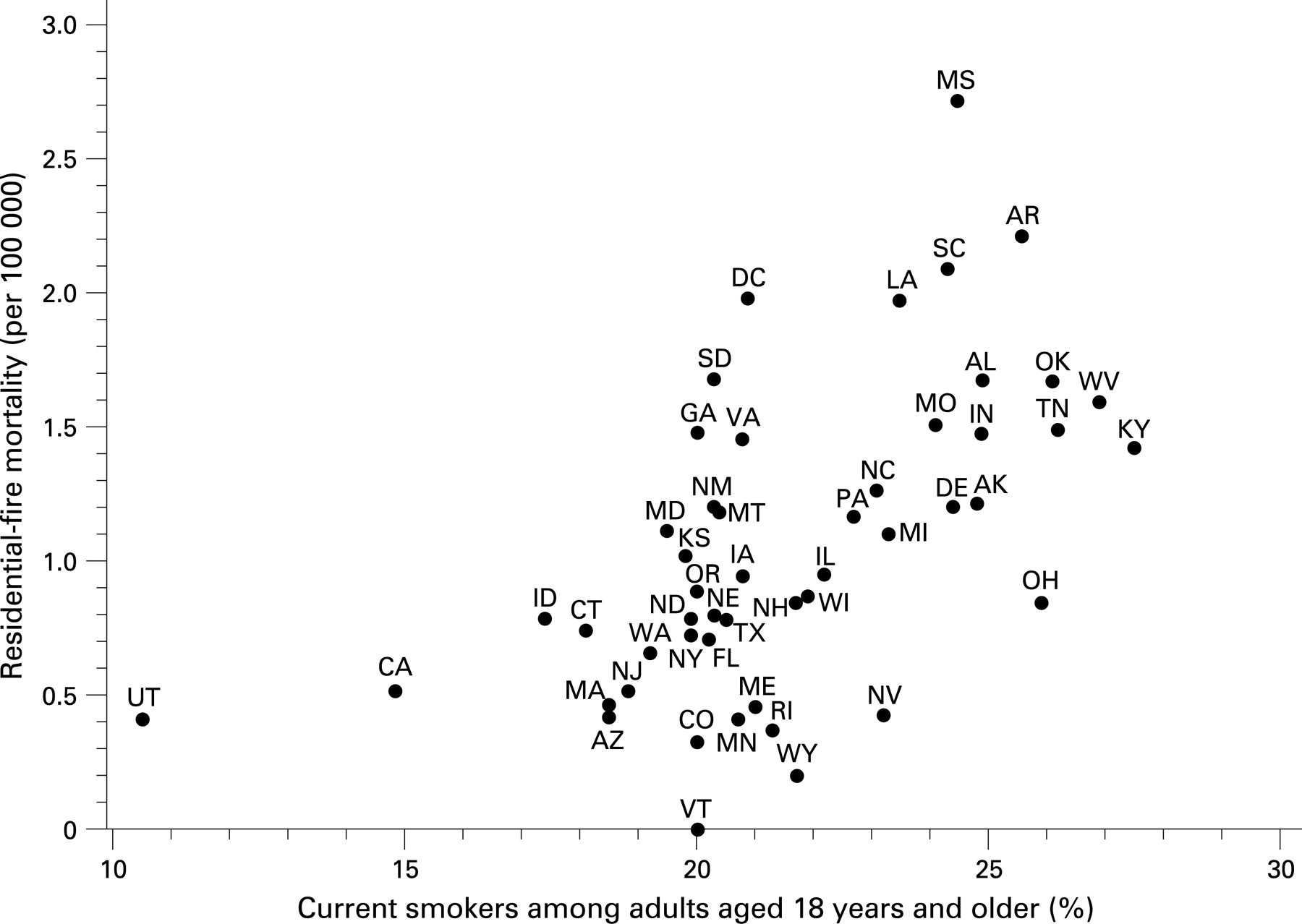
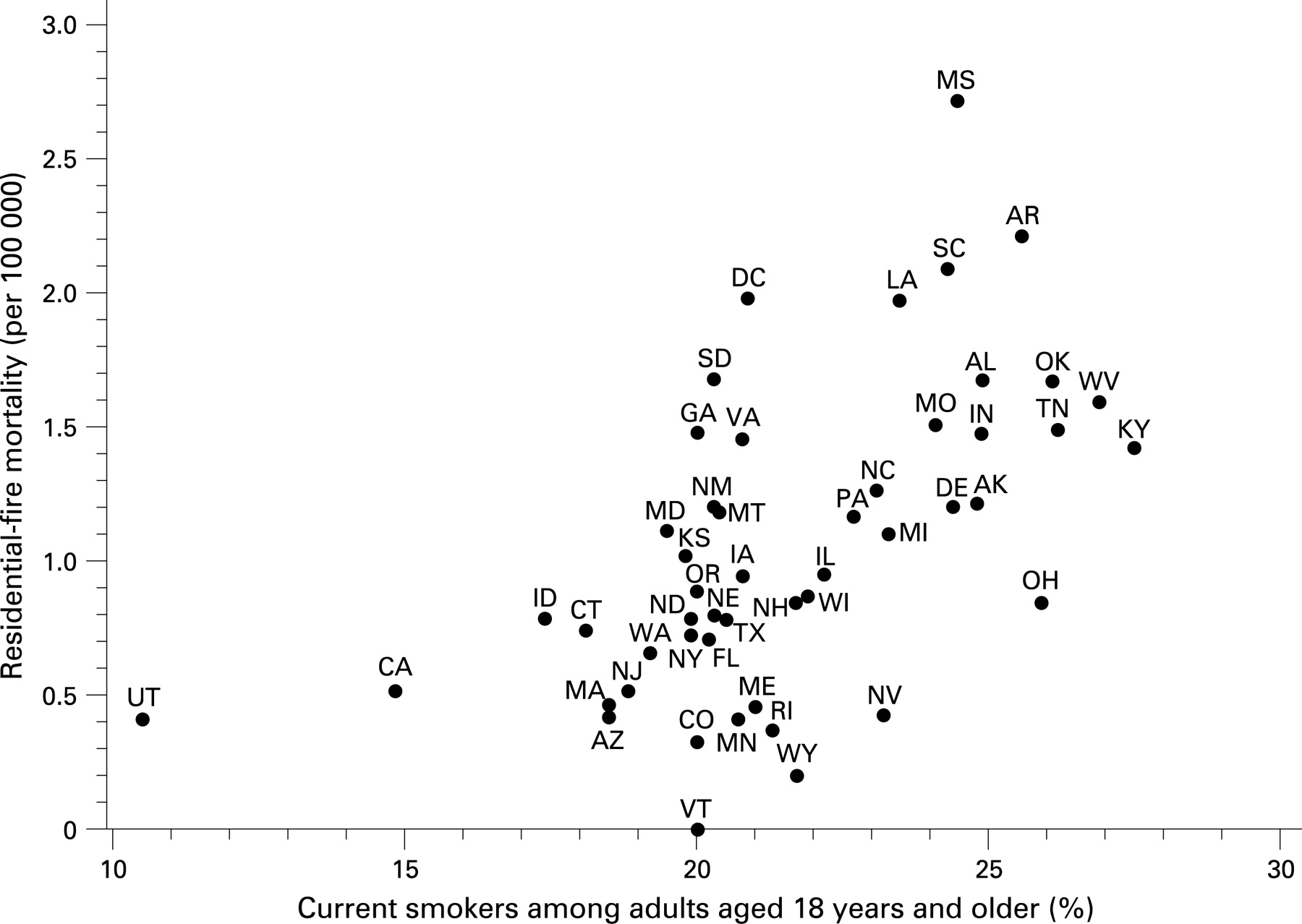
In 2004, there were 2810 residential-fire-related fatalities in the USA, corresponding to a national unintentional residential-fire mortality rate of 0.96 per 100 000. State-specific rates ranged from 0.00 in Vermont to 2.72 in Mississippi.14 Among adults aged 18 and older, the range of current smokers was 10.5–27.5%.15 Among adults aged 25 and older, 83.9% had a high school or high school equivalent degree.18 The median household income was US$44 684.18
Figure 1 displays the relationship between state-specific smoking percentages and residential-fire mortality. We found a significant, positive association between state-specific smoking and residential-fire mortality rates (r = 0.57).
{kind=link}
Regression analysis
Table 1 presents the estimated regression model coefficients. The percentage of current smokers remains significant in this model, after the effects of education and income are controlled for.
The statistically significant regression coefficient estimate of 0.075 for current smoking percentage observed in this study can be interpreted by recognizing the logarithmic transformation of rates inherent to the selected modeling process. Starting from a base fire mortality “R” for a given population, the value exp{0.075}≅1.08 suggests that a change in the smoking percentage of +1% (eg, from 20% to 21%) corresponds on average to a modeled rate of 1.08 × R. Similarly, the value exp{−0.075} ≅0.93 suggests that a change in the smoking percentage of −1% (eg, from 20% to 19%) corresponds on average to a modeled rate of 0.93×R. The latter is equivalent to an estimated relative rate associated with a 1% fall in the smoking percentage of (0.93×R)/R = 0.93. Similarly, the 95% CI end points for the relative rate associated with a 1% fall in the smoking percentage are calculated from the CI end points for the coefficient estimate, resulting in the 95% CI exp{−0.115} to exp{−0.034} or 0.89 to 0.97.
DISCUSSION
This study suggests a strong ecological association between residential-fire deaths and smoking. To our knowledge, this is the first study that quantifies this association using an ecological study design. This relationship was robust and remained significant even after selected socioeconomic factors had been accounted for. We found that even a modest 1% decrease in the percentage of current smokers corresponds to a 7% decrease in the modeled residential-fire mortality rate, which is promising for prevention. This finding is consistent with studies describing individual-level associations between smoking and residential-fire deaths.1 5 7 10
Key points
This ecological study quantified the association between smoking and residential-fire mortality, while controlling for selected socioeconomic factors.
A 1% decrease in smoking corresponded to a modeled 7% decrease in residential-fire mortality rates.
The ecological association found in this study is consistent with findings from studies examining individual-level associations between smoking and residential-fire deaths.
Successful smoking cessation efforts and adherence to fire protection recommendations may reduce the risk of cigarette-related residential-fire injuries and deaths.
The results of this analysis are strengthened by research that suggests that real-world reductions in smoking-related fire deaths are achievable. Hall22 compared forecasted versus actual deaths due to fires involving smoking materials for the period 1984–1995. The forecast estimate, which was based on changes in cigarette consumption patterns, predicted a 30% net decline in smoking-related fire deaths. This estimate was identical with the actual decline in the percentage of smoking-related fire deaths during the same time period (ie, 30%). Similarly, Garbacz and Thompson23 concluded that a “…60% decline in (cigarette) consumption from 1963 to 2003 may have accounted for about a 60% decline in fire deaths over that period” (p 15). This was based on an elasticity estimate derived from a risk model that tested the impact of smoke detectors and other factors, such as cigarette consumption, on fire deaths. Results from the Garbacz and Thompson study also indicated that cigarette smoking had an estimated 10-fold impact on fire death rates when compared with smoke alarms. Although these findings point to the potential of efforts to reduce cigarette smoking, changes in smoking patterns may not be sufficient to produce continued declines in residential-fire deaths.22
Behavior change efforts that focus on individual behaviors, such as smoking, often have a limited effect at the population level. Social ecological theory suggests that there are environmental influences at the relationship, community, and societal levels that interact with, and influence, individual-level human behavior.24 Policy and legislation efforts may offer a broader public health impact.25 In recent years, legislative efforts have promoted the adoption of fire-safe cigarette laws at the state level. Fire-safe cigarette legislation is a population-based strategy for reducing cigarette-ignited fires and associated injuries. Fire-safe cigarettes reduce the risk of cigarette-ignited fires by using technology that makes the cigarette self-extinguish when left unattended.26 As of January 2008, 22 states across the USA have passed fire-safe cigarette legislation, and these states represent 52% of the national population.25 In 2005, Canada became the first country to require fire-safe cigarettes nation-wide. Fire-safe cigarette laws provide an excellent example of the interplay between environmental factors (state laws and technological advances) and individual factors (smoking behaviors).
This study had several limitations. The BRFSS and US census data were subject to potential errors associated with survey research, including exclusion from the sampling frame, non-response, and reporting errors (eg, recall bias and under-reporting). Although the model estimates for our predictors are also subject to modest sampling variability, and the estimated model coefficients may thus incorporate bias, such bias is typically toward the null.27 Further, the analysis relies on state-level data, and extending the findings to individuals is limited by the familiar ecological fallacy.28 In other words, it is not possible to know—solely on the basis of these aggregate data—whether the individuals who were smokers are also the individuals who were involved in a fatal residential fire. Nonetheless, we believe that this association is also plausible at the individual level because smoking is the leading cause of residential-fire deaths5 and the presence of smokers in a house is a risk factor for residential-fire injury.29 The impact of cigarette smoking on residential-fire death rates may be considerable in poor nations, which often have high rates of smoking, substandard housing conditions, and inadequate fire protection and response systems.30 31
Conversely, the ecological design used in this study can also be viewed as one of its primary strengths because it offers a convenient and low-cost approach to quantifying the relationship between group level factors. Ecological approaches are ideal for studying unintentional injuries19 and residential fires32 because these phenomena are both complex in nature and influenced by factors at the individual and environmental levels. According to Stevenson and McClure, 33 the use of this design “is also particularly valuable when an individual level association is evident and an ecological level association is assessed to determine its public health impact” (p 2).
IMPLICATIONS FOR PREVENTION
Although smoking cessation campaigns aim to reduce the occurrence of chronic diseases such as lung cancer, emphysema, and cardiovascular disease, the statistical findings in this paper suggest that reductions in smoking that result from such programs may also contribute to a reduction in residential-fire deaths. Smoking cessation programs have shown promise,32 and a survey indicated that 70% of current US adult smokers report wanting to quit.34 In 2005, an estimated 19.2 million (42.5%) adult smokers who were trying to quit had stopped smoking for at least 1 day during the preceding 12 months.9
People who smoke should attempt to quit. The US Department of Health and Human Services, National Institutes of Health, and National Cancer Institute provide a free helpline (1-800-Quit Now) for smokers who want to quit and need help doing so.
Those who continue to smoke should do so outside the house. However, people who smoke indoors may reduce their risk of injury from residential fires by following several recommendations:
Use deep, sturdy ashtrays that are set on something secure and hard to ignite, such as an end table
Douse cigarette and cigar butts in water, or extinguish them with sand, before dumping them in the trash
Do not allow smoking in a home where oxygen is used
Never smoke in bed or leave burning cigarettes unattended
Do not smoke if sleepy, drinking, or using medicine or other drugs
Use fire-safe cigarettes, where available
Additional tips for residential-fire prevention are available at http://www.cdc.gov/ncipc/factsheets/fireprevention.htm.
CONCLUSIONS
Residential-fire mortality rates are high in states with high smoking rates. This relationship cannot be explained by selected socioeconomic factors alone, which suggests that successful efforts to reduce smoking may translate into a reduction in residential-fire mortality rates.
REFERENCES
Footnotes
The findings and conclusions in this report are those of the authors and do not necessarily represent the official position of the Centers for Disease Control and Prevention/the Agency for Toxic Substances and Disease Registry.
Competing interests: None.