Article Text

Abstract
Objective: The objective of this study is to use a new data set to compare the circumstances of fatal poisoning in deaths ruled as suicides to those ruled as unintentional, particularly with regard to the prevalence of mental health, substance abuse, and other risk factors.
Design: The design is an analysis of all fatal poisonings using data from the New Jersey Violent Death Reporting System.
Patients or subjects: Decedents in New Jersey in 2003 whose cause of death was fatal poisoning, and whose manner of death was unintentional, intentional, or undetermined.
Main outcome measures: The relation between risk factors, circumstances of death, and coded manner of death, particularly for those with both mental health and substance abuse related risk factors.
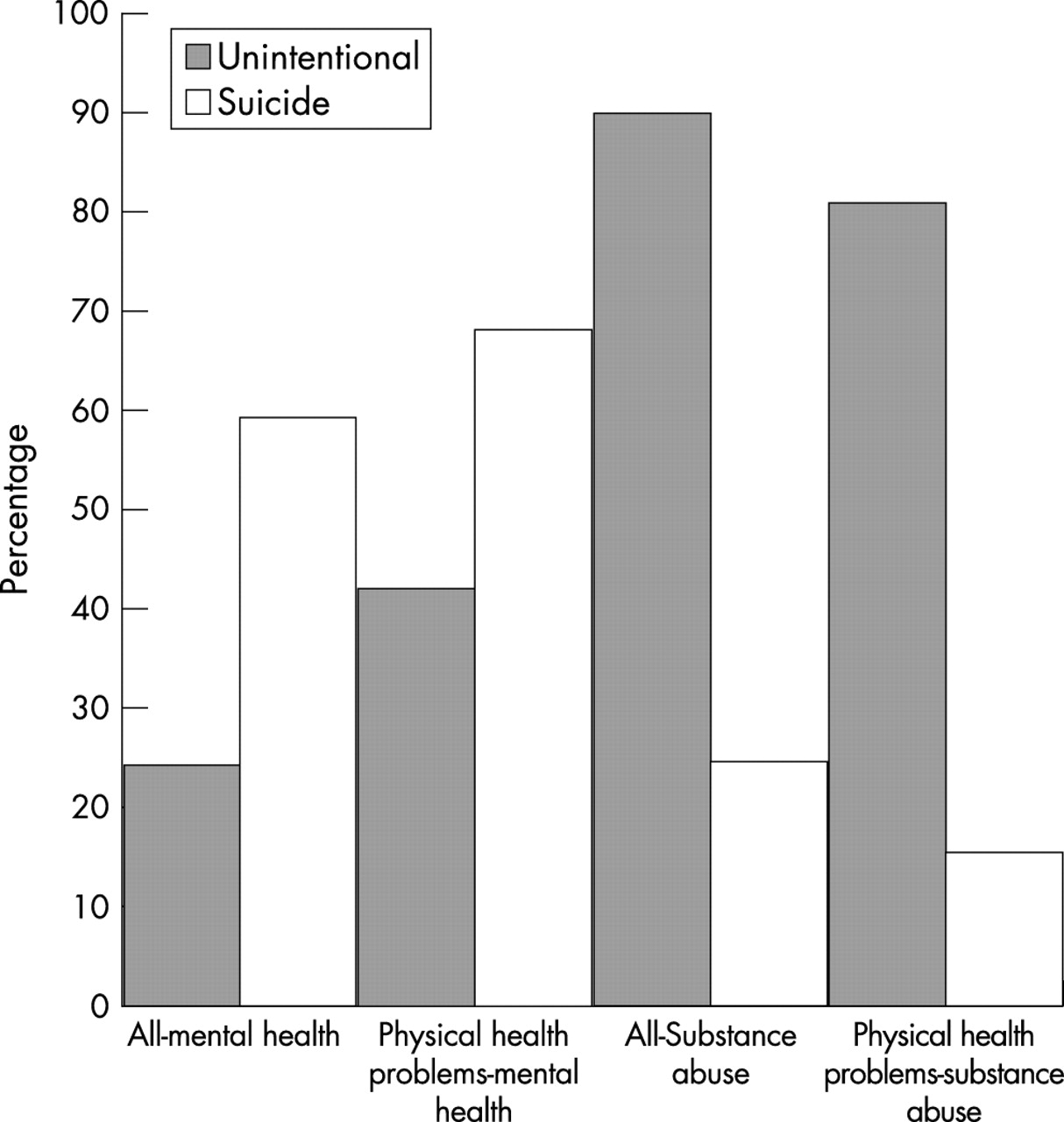
Results: The prevalence of mental health risk factors was considerably higher among intentional poisonings (59.4% v 24.4%, p<0.0001), while that of substance abuse was higher among unintentional poisonings (90.0% v 24.5%, p<0.0001). Approximately 20% of unintentional poisonings and 25% of suicides had a physical health problem. Differences in circumstances by manner were smaller among those with a physical health problem.
Conclusions: Substance abuse, mental health, and physical health problems were the most frequently cited risk factors for unintentional and intentional poisoning fatalities. There were many differences in characteristics and risk factors by manner of death. Those with physical health problems were more similar in terms of demographic characteristics and presence of other risk factors.
- NVDRS, National Violent Death Reporting System
Statistics from Altmetric.com
While suicide by poisoning has remained relatively flat in past years, fatal unintentional poisonings have increased considerably. In the US state of New Jersey, poisoning was the second leading cause of unintentional injury mortality in 2003, and the number of poisoning deaths (623) approached the number of deaths from motor vehicle crashes (761).1 There are more than three times as many unintentional poisoning fatalities each year in New Jersey as compared with suicides by poisoning (fig 1).
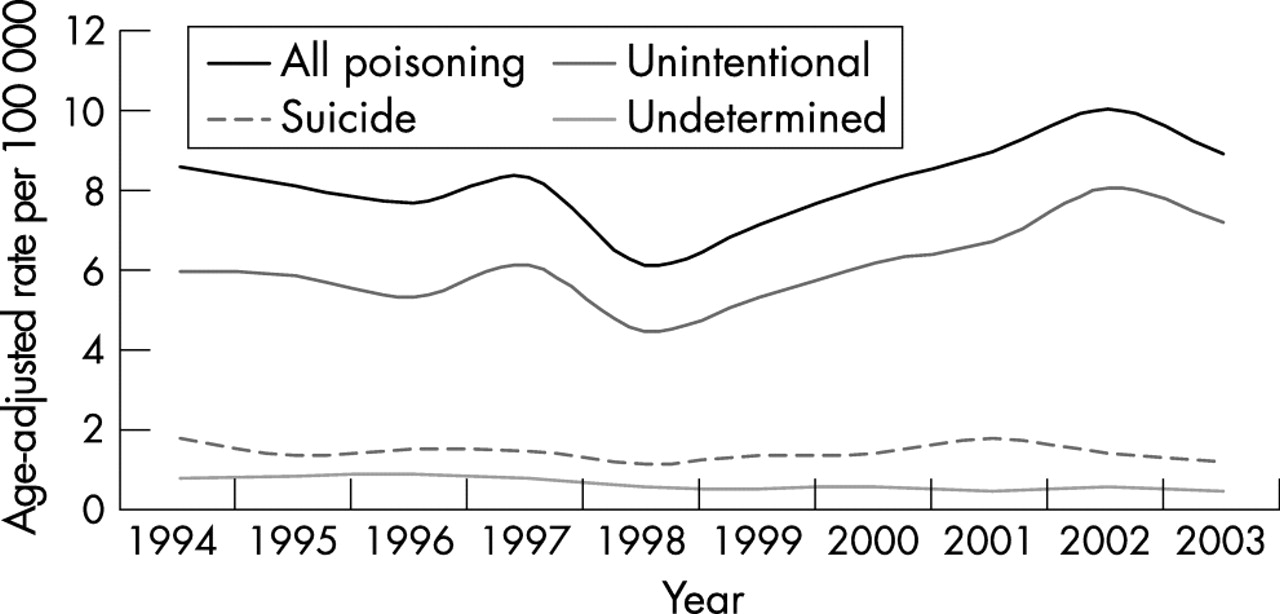
Poisoning deaths in New Jersey by intent, 1994–2003.
In part, these high rates of unintentional poisoning fatalities are attributable to the fact that New Jersey has high rates of substance abuse, and a supply of street drugs which is above average in terms of purity.2 While New Jersey’s rate is above average, unintentional poisoning is also a growing national problem.3,4
Poisoning is defined as damaging physiologic effects from substances classified as illicit drugs, pharmaceutical drugs (both prescribed and over the counter), chemicals, such as pesticides, heavy metals (such as mercury), gases/vapors, such as carbon monoxide, or household substances, such as antifreeze or bleach. This classification is somewhat unsatisfactory in that many pharmaceutical drugs, such as oxycodone, are often sold illicitly, or otherwise obtained by persons without a valid prescription. Among adults, chemicals, household substances, and gases and vapors are almost exclusively used in suicides, and are rarely the cause of an unintentional death.
Little effort has been made to compare risk factors and circumstances of intentional and unintentional poisonings, but this may be of interest, because there may be similarities in circumstances which would have implications for prevention. It is believed that some fraction of fatal poisonings coded as unintentional or undetermined are actually suicides. Underreporting of suicide has been attributed to factors such as pressure from families and subjectivity among coroners and medical examiners.5,6,7,8,9,10,11 As compared with firearms and suffocation, suicide by poisoning is considered to be particularly susceptible to underreporting. The rapid rise in unintentional poisonings in recent years has led some to wonder whether part of this increase represents misdiagnosed suicides.
Intent may be a somewhat continuous concept in the case of fatal poisonings. Poisoning through pharmaceuticals or illicit drugs is a less “lethal” means of suicide as compared with firearms or hanging or even ingestion of noxious substances. There is also evidence that many substance abusers who survived “unintentional” overdoses had an ambivalent attitude toward their potential death.12,13 The rigid delineation created by manner of death coding may somewhat arbitrarily separate decedents who are not that dissimilar.
The purpose of this study is to use a new data set, the National Violent Death Reporting System (NVDRS), to examine how decedent characteristics, circumstances, and risk factors vary by coded manner of death in fatal poisonings. An examination of circumstances surrounding fatal poisonings as a group may reveal some similarities in circumstances across manner of death categories. A better understanding of these patterns may inform preventive practices in both the areas of suicide and substance abuse. Although the NVDRS is currently in use only in the US, this basic approach of coding circumstances of certain causes of death can be adapted to other contexts where there are medical examiner or coroner’s reports in addition to death certificate data for fatal poisonings.
DATA AND METHODS
The data used are death certificates and medical examiner reports for fatal poisonings occurring to adult residents of New Jersey in 2003. This study uses data on 679 fatal poisonings which occurred to New Jersey residents in New Jersey during 2003. There were 107 cases coded as suicides, 537 coded as unintentional, and 35 coded as undetermined. Poisoning deaths that occurred in hospitals are excluded. Cases were identified from medical examiner narratives and death certificates. The study is limited to cases where the immediate cause of death is toxicity, rather than cases where the immediate cause is trauma or is related to a medical condition exacerbated by drug ingestion. The causes of death included are those with underlying cause of death from unintentional poisoning (International Classification of Diseases, 10th revision, X40–X49), intentional poisoning (X60–X69), and poisoning of undetermined intent (Y10–Y19). Poisonings coded as homicides and legal intervention are excluded. The underlying cause of death and the manner of death are determined by the medical examiner at the scene investigation, and confirmed by autopsy and toxicology reports.
For all poisoning fatalities in 2003, the medical examiner narrative and death certificate were coded according to NVDRS protocols. The NVDRS is a detailed surveillance system which uses medical examiner narratives, law enforcement records, and death certificate data. These sources are linked for each violent death, and data items are coded according to a standardized protocol by trained coders from each participating state.
We first describe the differences in decedent characteristics and circumstances by coded manner of death. In particular, circumstances by manner are compared for those with and without evidence of physical health problems. We estimate a logistic regression to see which decedent and circumstance characteristics best predict documentation of physical health problems. The goal is to see whether there is evidence that risk factors and circumstances differ by manner of death categories, and to see what risk factors are significant in fatal poisonings.
RESULTS
Characteristics of fatal poisonings by manner of death
There were significant differences by manner of death in terms of demographic characteristics as well as presence of other circumstances. As shown in table 1, decedent gender varied by manner of death (p<0.01). The percent of decedents who are male is highest for unintentional poisonings. Non-Hispanic blacks were disproportionately represented among unintentional poisonings relative to other manners of death (p<0.01). The age distribution also varies significantly by manner, with unintentional poisonings relatively more likely to be younger adults (p<0.01). In part due to the different age composition, decedents from unintentional poisonings are significantly more likely to be never married (p<0.01). The category of undetermined intent, which is relatively small in New Jersey, falls in between the suicide and undetermined categories with regard to age and marital status, but is most likely to be female, and most likely to be non-Hispanic white.
Demographic characteristics, fatal poisonings, New Jersey, 2003
The most common drug type used were illicit drugs, which in New Jersey largely consists of heroin and cocaine. Illicit drugs were used in nearly 70% of all fatal poisonings, but were far more common in unintentional poisonings as opposed to suicides (82.3% v 12.2%; p<0.01). The category “illicit” drugs excludes drugs such as oxycodone which, although they are prescription drugs, are often purchased and used in an illicit manner. Therefore the significance of “illicit” drugs is understated by the current typology. Use of pharmaceutical products was far more common in suicides (57.0% v 13.8%; p<0.01).
Table 2 lists leading individual drugs mentioned in fatal poisoning. Cocaine and heroin each are mentioned in nearly 40% of cases, although they are used jointly in approximately 15% of all deaths. Other leading drugs are morphine and oxycodone. The use of opiates is far more common in the case of unintentional as compared to intentional poisoning (79% v 28%; p<0.01), with undetermined deaths falling somewhere in between.
Leading drugs mentioned in fatal poisonings, New Jersey, 2003
Table 3 shows the prevalence of mental health and substance abuse risk factors in fatal poisonings. The true prevalence of these conditions is probably underreported, as information from friends and relatives or evidence at the scene may not be present in all cases. The NVDRS includes a number of questions about mental health, pertaining to diagnosis and current treatment. For the purposes of this analysis, any positive responses were coded as evidence of a mental health risk factor. The NVDRS also has a circumstance question relating to whether the decedent had a known problem with substance abuse, either alcohol and/or other substances. The prevalence of mental health related risk factors is highest among those deaths coded as undetermined as compared with suicides and unintentional (71% v 59.4% (suicide) v 24.3% (unintentional); p<0.01), while substance abuse is most likely among those coded as unintentional poisonings.
Mental health and substance abuse risk factors, fatal poisonings, New Jersey, 2003
Only 10% of all cases had neither of these risk factors, while 20% had both types. The prevalence differed by manner. In only approximately 6% of unintentional poisonings was there no reported mental health or substance abuse risk factors, while this was true for more than 30% of suicides.
Selected circumstances are shown in table 4. The presence of a physical health problem was most commonly noted. Most of the other circumstances were noted fairly infrequently, and many of these circumstances were more likely to be reported in suicides as compared with unintentional poisonings. For example, in deaths ruled suicides it was more likely that there was a crisis in the past two weeks (p = 0.01), prior evidence of an intent to commit suicide (p<0.01), prior suicide attempts (p<0.01), a financial problem (p = 0.03), an intimate partner problem (p<0.01), a job problem (p = 0.012), or a legal problem (p<0.01), as compared with unintentional poisonings.
Presence of selected circumstances, fatal poisonings, New Jersey, 2003
Decedents with physical health problems
Aside from substance abuse and mental health problems, which are major and well known risk factors for overdose and suicide, respectively, the existence of a physical health problem was the most prevalent risk factor to emerge from this analysis of circumstance data. This is the only circumstance that appeared important in all manner categories. While the proportion citing a physical health problem is higher for suicides than in the case of unintentional poisonings, the difference is not statistically significant. Further, the presence of a physical health problem stands out as a particularly important circumstance of death in the case of unintentional fatalities, as the prevalence of most of the others is quite low.
Compared to other fatal poisonings, those with physical heath problems were more likely to be female (42% v 22%, p<0.01), were an average of approximately five years older, (44.1 v 39.2 years, p<0.01), were more likely to use prescription drugs (42.5% v 17.8, p<0.01), and were less likely to have a manner of death coded as unintentional (70.0% v 81.5%, p<0.01). Given the frequent stories of addiction to painkillers following illness or injury, one might expect that physical health problems and substance abuse problems would be positively correlated, but in fact the opposite is the case. For fatal poisonings as a whole, there is a significant and negative correlation between having a physical health and substance abuse problem (r = −0.1491, p<0.01), while the correlation between physical and mental health problems is positive and significant (r = 0.1989, p<0.01). This relation is also significant for unintentional poisonings, but not among those coded as suicides.
Among decedents with a physical health problem, some differences by manner of death categories are lessened. For example, gender, race and ethnicity and marital status do not differ significantly by manner of death among those with a physical health problem, although significant age differences remain. Additionally, while use of illicit drugs still differs by manner (65.3% v 11.5%, p<0.01), the difference is smaller than when all deaths were included. As shown in figure 2, while differences in substance abuse and mental health risk factors differ less by manner among those with a physical health problem, they remain significant (p<0.01).

{kind=link}
{kind=link}
Mental health, substance abuse, and physical health problems by manner.
There is also more similarity across manner of death categories in the prevalence of event related circumstance variables when the population is restricted to those with a physical health problem. For example, the proportion experiencing a crisis in the past two weeks, having an intimate partner problem, a job problem, legal problem, relationship problem, and/or death of a friend/family member are not significantly different by manner when the population is restricted to those with a physical health problem. Interestingly, a physical health problem is positively related to the presence of these other types of circumstances for unintentional poisonings, while negatively for suicides, causing a lessening of differences by manner of death for this group. So the probability of having a crisis in the past two weeks, for example, is positively and significantly correlated with having a physical health problem among deaths coded as unintentional (r = 0.1713, p<0.01), while negatively but not significantly correlated in the case of suicide (r = −0.1706, p<0.07). These findings could be summarized by noting that unintentional poisonings with a physical health problem are more like suicides in terms of decedent characteristics and circumstances of death as compared with other unintentional poisonings.
The presence of a physical health problem is also related to drug used. As noted, the use of illicit drugs is less common in the cases where a physical health problem is present as compared with all fatal poisonings. There are also particular drugs which are more likely to be used in poisonings with reported physical health problems. The most notable of these is oxycodone, which is positively correlated with physical health risk factors for all fatal poisonings and for unintentional poisonings (p<0.01).
The various correlates of physical health problems can be assessed more completely through a multivariate logistic regression, where the probability of having a physical health problem is estimated as a function of demographic and other circumstance characteristics. As can be seen in table 5, physical health problems are more likely to occur among older adults (p<0.01), females (p<0.01), those with mental health risk factors (p<0.01), and those without substance abuse problems (p<0.05). Additionally the probability of a physical health problem was lower in the case of suicides (p<0.05). Physical problems among poisoning victims were more common in cases where decedents had experienced a crisis in the last two weeks (p<0.05) and where oxycodone was used (p<0.01).
Probability of physical health problem, fatal poisonings
DISCUSSION
This analysis of circumstances of fatal poisonings suggests that overall, poisonings coded as unintentional and intentional have quite different risk factors and characteristics. The most apparent differences relate to substance used and documentation of substance abuse and mental health risk factors. Results of this analysis do not suggest that a sizable portion of unintentional poisoning fatalities are miscoded suicides, as the characteristics of decedents and the circumstances of death are quite different. However, physical health problems appear to be a risk factor which cuts across manner of death categories, and differences between manner of death categories are smaller for this group of decedents.
Implications for prevention
The main factor involved in fatal poisonings in New Jersey is clearly illicit drugs, namely cocaine and heroin, so prevention of these fatalities must involve in great part substance abuse treatment, drug interdiction, and attempts to reduce the purity of these substances. The trend in suicide by poisoning has been essentially flat over the past several years, and risk factors for these deaths include mental health risk factors and several of the other suicide circumstances, such as existence of a recent crisis. It is worth noting that the great majority of poisoning suicides did not occur to decedents with documented substance abuse problems, suggesting either that substance abuse is undermeasured or that addiction per se was not a major factor in many of these suicides by poisoning.
The importance of physical health problems in both unintentional and intentional fatal poisonings, and the relation between physical health problems and use of certain substances, most particularly oxycodone, provides an opportunity for prevention. More needs to be learned about the nature of these physical ailments, and whether inadequate or inappropriate medical care and potentially overreliance on pain medications may be a factor. The US Drug Enforcement Agency has noted the existence of suspicious prescribing practices in some areas of New Jersey.2 It may be the case that controlled substances need to be more carefully monitored, as has been initiated in several other states.14 Further work needs to be done to analyze potential spatial patterns in fatal poisonings, particularly those that involve physical health problems and prescription pain medications.
Key points
-
Poisoning is a cause of death which is increasing in New Jersey and elsewhere.
-
Characteristics of fatal poisonings coded as unintentional versus intentional differ considerably, with decedents in unintentional poisonings (overdoses) being more likely to be male, non-white, young, and to have used illicit drugs, compared with suicides.
-
Decedents coded as suicides were more likely to have mental health risk factors; those coded as unintentional were more likely to have substance abuse risk factors.
-
Presence of a physical health problem was an important circumstance that seemed to cut across different manner of death categories. Decedents with physical health problems had fewer differences by manner.
-
About 70% of poisoning deaths involve illicit drugs, and poisoning deaths with a physical health problem are disproportionately likely to involve oxycodone. Increased monitoring of controlled substances and increased availability of substance abuse treatment services may be important strategies to prevent poisoning deaths.
Footnotes
-
This work was supported by the Centers for Disease Control and Prevention (CDC), National Violent Death Reporting System Grant No #U17/CCU222395.
The findings and conclusions in this report are those of the authors and do not necessarily represent the views of the Centers for Disease Control and Prevention.
-
Competing interests: none.