Article Text

Abstract
Objective To elucidate the performance of a shock-absorbing floor material with a mechanical metamaterial (MM-flooring) structure and its effect on the gait and balance of older adults.
Methods The drop-weight impact was applied to evaluate the shock-absorbing performance. The falling weight was adjusted equivalent to the energy exerted on the femur of an older woman when she falls, which was evaluated on the MM-flooring and six other flooring materials.
Nineteen healthy people over the age of 65 years participated in the gait and balance evaluations. The timed up and go and two-step tests were adopted as gait performance tests, and the sway-during-quiet-balance test with force plates and the functional reach test (FRT) were adopted as balance tests. All the participants underwent these tests on the MM-flooring, shock-absorbing mat and rigid flooring.
Results The shock-absorbing performance test revealed that MM-flooring has sufficient shock-absorbing performance, and suggesting that it may reduce the probability of fractures in the older people when they fall. The results of the gait performance test showed that the participants demonstrated the same gait performance on the MM-flooring and the rigid floor. In the quiet standing test, MM-flooring did not affect the balance function of the participants to the same extent as the rigid floor, compared with the shock-absorbing mat. In the FRT, no significant differences were found for any of the flooring conditions.
Conclusions MM-flooring has the potential to prevent fractures attributed to falls and does not affect the gait or balance of older adults.
- Engineering
- Environmental Modification
- Product Modification
- Non-randomized Trial
- Older People
- Hip Facture
Data availability statement
Data are available upon reasonable request. The datasets generated for this study are available on request to the corresponding author.
This is an open access article distributed in accordance with the Creative Commons Attribution 4.0 Unported (CC BY 4.0) license, which permits others to copy, redistribute, remix, transform and build upon this work for any purpose, provided the original work is properly cited, a link to the licence is given, and indication of whether changes were made. See: https://creativecommons.org/licenses/by/4.0/.
Statistics from Altmetric.com
- Engineering
- Environmental Modification
- Product Modification
- Non-randomized Trial
- Older People
- Hip Facture
Introduction
Falls are associated with health risks, such as deterioration of physical functions and limitation of activities of daily living. Considering the incidence of proximal femoral fractures, epidemiological studies have demonstrated that more than 85% of proximal femoral fractures are attributed to falls; the number of falls is a risk factor that increases gradually from 40 years, with a steep increase after 75 years of age.1 Clinical vertebral and hip fractures are associated with a substantial increase in the mortality of relatively healthy older women.2 Although falls are a risk that should be avoided, their complete prevention is impossible in humans who walk on two legs. At least one-third of community-dwelling people aged over 65 years report incidences of fall each year.3
To prevent serious injuries, such as fractures in the event of a fall, research is being conducted on flooring materials that specialise in shock absorption.4 Their aim is to reduce the risk of fractures by cushioning the flooring to mitigate the concentration of the impact force of falls.5 Although softer floors would provide greater attenuation in the fall impact forces, excessive reduction in the floor stiffness may increase instability/body sway, impair mobility and balance, and increase the risk of falls.6–8 Thus, there is a need to consider the effect of the softness of the floor on the body balance. A flooring material with adequate shock-absorbing effect that does not affect gait and maintain balance would be useful in preventing fall-related injuries.
Shock-absorbing flooring materials using conventional materials and using the structural knowledge of mechanical metamaterials (MM-flooring) have now been developed (figure 1). MM are materials for which the macroscale properties are determined by a small-scale topological design.9 These are a class of artificial materials with rare anomalous mechanical properties,10 which have attracted scholarly attention owing to their superior properties.9 11 An example of the use of this technology is the production of auxetic materials,12 which decreases in thickness perpendicular to stress; this property is not observed in nature. This technology can render a rigid object flexible by modifying the structure to distribute the force such that it deforms in a different or torsional direction in response to the force applied to the object.10 13 Furthermore, with the advent of three-dimensional printing, creating objects with complex internal structures has become possible,12 which is expected to be used in various fields to produce materials with more detailed structures and improve production efficiency.11 The newly developed MM-flooring is made of thermoplastic elastomer and has a MM structure that maintains its hardness under normal loading and walking and distributes the impact in the contact area in the event of a fall, thereby providing high cushioning and shock absorption. Confirming the shock-absorbing and walking stability of this flooring material would help resolve the traditional trade-off problem from a structural point of view. This study aimed to compare the shock-absorbing performance of MM-flooring with that of other shock-absorbing flooring materials and examine its effects on walking and balance in healthy older adults.

The MM-flooring. Newly developed flooring material with a mechanical metamaterial structure (MM-flooring). MM-flooring, mechanical metamaterial flooring.
Methods
Experiment 1: effect of shock-absorbing
Floor conditions
The MM-flooring used in this study was manufactured in units of 500×500 mm area and 27 mm thickness. One unit of the MM-flooring was used in experiment 1 (figure 1). The buffer material is a thermoplastic elastomer with a structure based on MM, which is covered with a 1 mm thick vinyl chloride sheet to make a floor material. The following six types of flooring materials and cushions were used for comparison: a carpet tile (polypropylene, 6 mm thickness), vinyl floor (vinyl chloride, 2 mm thickness), Tatami, which is a traditional Japanese floor material (rush, 55 mm thickness), rug (polyester, 18 mm thickness), joint mat (polyethylene foamed material, 20 mm thickness) and shock-absorbing mat (polyethylene and polyurethane foam, 40 mm thickness).
Drop-weight impact test
A drop-weight impact testing system to evaluate femur fractures developed by Nagoya University was used for the shock-absorbing test.14 In this system, weight is dropped vertically and impacted with a physical model simulating the thigh of an older Japanese woman to reproduce a fall (figure 2). This test has been used in previous impact evaluation tests since it can evaluate femur fracture risks with changing impact conditions.15 A steel plate with a mass of 11 kg (area: 300×300 mm, thickness: 30 mm) was dropped at a height of 230 mm to render the energy equivalent to the impact on the femur around the great trochanter of a woman with a height of 149.3 cm and weight of 55.3 kg during falling.16 The height and weight measurements used in the model correspond to the average values of older Japanese women aged 66.9 years old.17 Each flooring material was attached to the underside of the steel plate. The femur model was developed based on biomechanics: a simulated bone similar in size to the model of the older woman described above (Sawbones #3414, A Pacific Research Company, USA) was used. Silicon material simulating the shape and the stiffness of the soft tissue of the thigh covers from the proximal to middle area of the femur bone as well as around the greater trochanter. The load cells were placed at the femoral head to measure the impact force acting on the femur head when the weight collided.
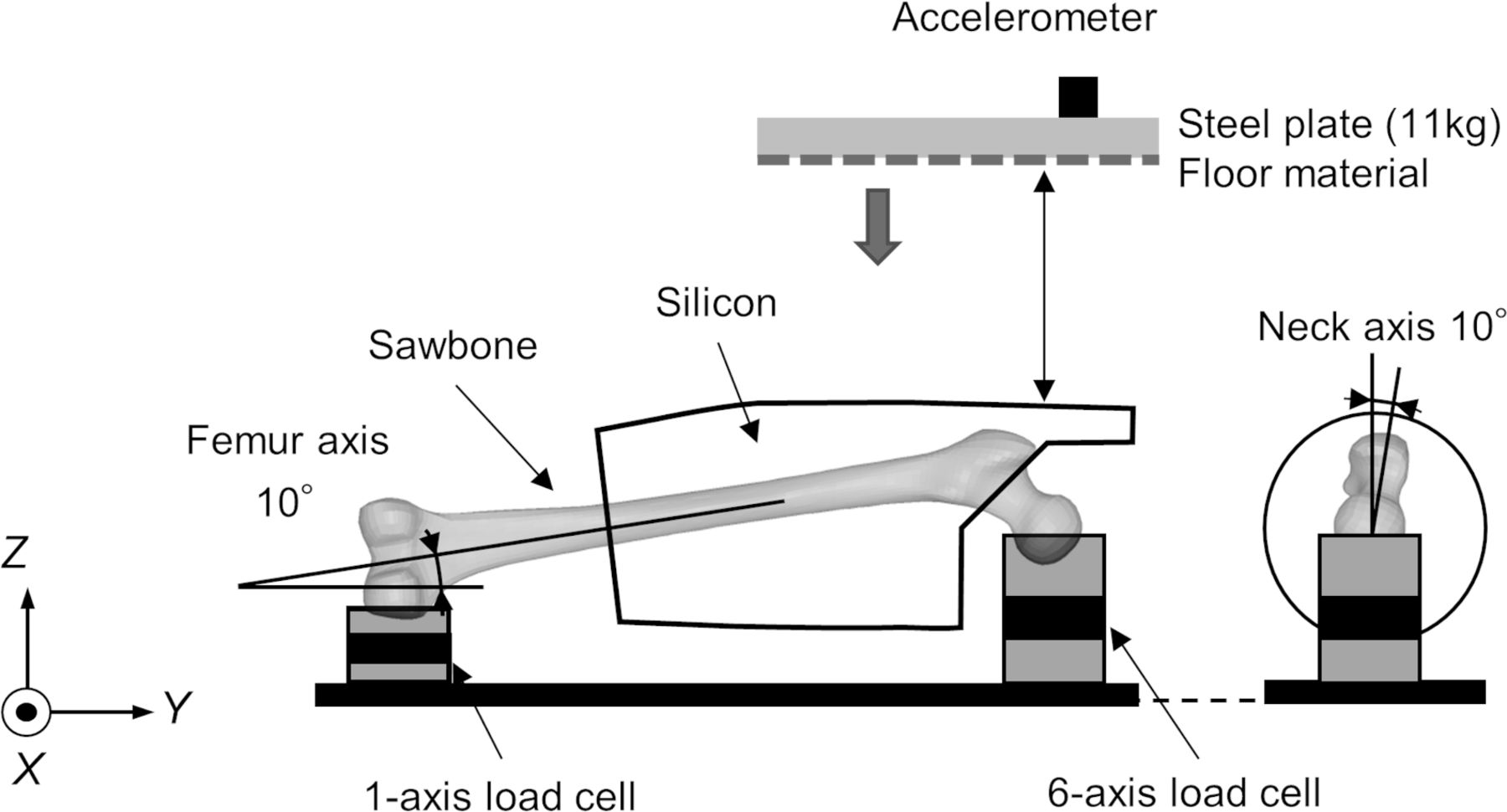
A schematic diagram of the drop weight impact test. Steel plates were set at 230 mm to render the energy equivalent to that of a person with a height of 149.3 cm and weight of 55.3 kg. Each flooring material was attached to the base of a steel plate that was dropped and impacted on the femur model. A silicon rubber shock-absorbing material was attached around the greater trochanter of the femur model as the soft tissue of the buttocks. The force sensors were placed at the femoral head to detect the impact acting on the femur when the weight collided.
Experiment 2: influence on gait and balance
Participants
Nineteen healthy people aged >65 years (mean age 74.4±6.0, 13 men, 6 women, mean height 162.2±9.6 cm, mean weight 59.7±12.7 kg) participated in this study. This study was conducted on community-dwelling people aged 65 years or older who were publicly invited to participate, and who had a stable general condition and were able to perform daily-life activities independently. They were able to maintain a stable closed-eye standing position on a normal floor.
Floor conditions
The MM-flooring used the same specifications as that in the drop-weight impact test. For the gait performance test, the measurement environment was constructed by arranging 60 units of MM-flooring in a 3×5 m area without gaps, which were covered a 1 mm thick vinyl chloride sheet. For the gait performance test, the comparison objects were the normal rigid floor surface. For the balance test, a rigid floor and a shock-absorbing mat with an area of 500×500 mm and a thickness of 40 mm (the buffer material parts were polyethylene and polyurethane foam, respectively) were prepared and compared with 1 unit of MM-flooring.
Evaluation of the gait performance
The timed up and go (TUG)18 and two-step tests19 20 were adopted as gait performance tests. Two floor conditions, the MM-flooring and rigid floor, were used for evaluating the gait performance.
The TUG is a standard clinical assessment tool, which assesses the balance during a range of activities of daily living (eg, transfers, locomotion and turning).18 The test involves the participant standing up from a chair, walking forward 3 m at a self-selected speed, turning around, walking back to the chair and reseating themselves. The time from the moment of rising to that of return to the seated posture was measured with a stopwatch. Participants were measured for each of the clockwise and counterclockwise turns, and the fastest time was taken as the measured value.
The two-step test was developed as a screening tool for walking ability.19 20 The participant starts from the standing posture and moves two steps forward with maximum stride with caution to prevent losing balance. If the participant succeeds in holding the final standing position for longer than 3 s without any additional steps, the trial was judged as completed. The distance is then standardised by dividing the participant’s height for calculating the two-step test value. The test was performed two times, and the best result was used for the analyses.
Evaluation of balance
The sway during the quiet balance test with force plates21 and the functional reach test (FRT)22 were adopted as balance tests. Three floor conditions were used for balance evaluation: MM-flooring, shock-absorbing mat and rigid floor.
The evaluation of sway during quiet stance is a common balance assessment tool owing to its ease in measurement and significant association with fall risk.21 A portable force platform (AccuGait, Advanced Mechanical Technology, Watertown, Massachusetts) with a custom-written computer program (LabVIEW V.2019 software, National Instruments, Austin, Texas) was used. The platform was equipped with strain gauges that facilitated monitoring of the changes in ground reaction forces. Based on the data collected by the platform, estimating the position and deflection of the centre of pressure (COP) is possible. The external dimensions of this platform were 500×500 mm, and raw data were collected at a frequency of 100 Hz; low-pass filtering with a cut-off frequency of 10 Hz was performed to eliminate noise from the obtained COP displacement signal. Participants were instructed to stand quietly with their legs closed on each floor set up on the force platform. During the quiet stance task, the movement of the COP under the participant’s feet with their eyes open and closed was assessed for 10 s each. The rectangular area was calculated by multiplying the maximum trajectory length of the left–right with anterior–posterior COP displacements for 10 s.
The FRT assesses functional balance and limit of stability (in centimetres) during standing, which is reliable and valid in older adults.22 23 The participant was instructed to stand on each floor and close to a wall without touching the wall and position the arm that is close to the wall at a 90° angle of shoulder flexion with the fingers extended. The assessor marked the tip of the middle finger on the wall as the starting position. The participant was instructed: ‘Reach forward as far as you can without taking a step’. The location of the middle fingertip at the end of reaching forward was recorded. The difference between the starting and ending positions was measured in centimetres. A larger distance indicates better balance. All the participants performed the procedure two times for each floor condition, and the better score was used.
Data analysis and statistical analysis
For all the tests, the mean and SD of the adopted values for all the participants were calculated and used for comparison. For the gait performance, TUG and two-step tests, a paired t test was used. For the balance and sway during quiet standing tests, as well as the FRT, a one-way analysis of variance (ANOVA) was performed to analyse the effect of the different floor conditions. Tukey’s Honestly Significant Differences method for multiple comparisons was used for post hoc analysis if a given ANOVA demonstrated a significant main effect. All the statistical analyses were conducted using R V.3.6.1 (2019-07-05). Statistical significance was set at p<0.05 for all the tests.
Results
Experiment 1: effect of shock absorbing
Time histories of the load cell force at the femur head in the drop-weight impact tests are shown in figure 3. The maximum force decreased and the time duration increased by attaching the floor materials, which implies that the floor materials absorbed impact energy. The maximum impact force was 3.51, 2.91, 2.64, 2.46, 2.12, 1.33 and 1.98 kN on the carpet tiles, vinyl floor, tatami, rug, joint mat, shock-absorbing mat and MM-flooring, respectively.

Result of the drop weight impact test. The results of the drop-weight impact tests on seven types of flooring materials, including mechanical metamaterial (MM) floors, are shown. The horizontal axis indicates the time from the moment the weight hits the greater trochanter of the femur model, and the vertical axis indicates the magnitude of the impact on the femur.
Experiment 2: influence on the gait and balance
Evaluation of the gait performance
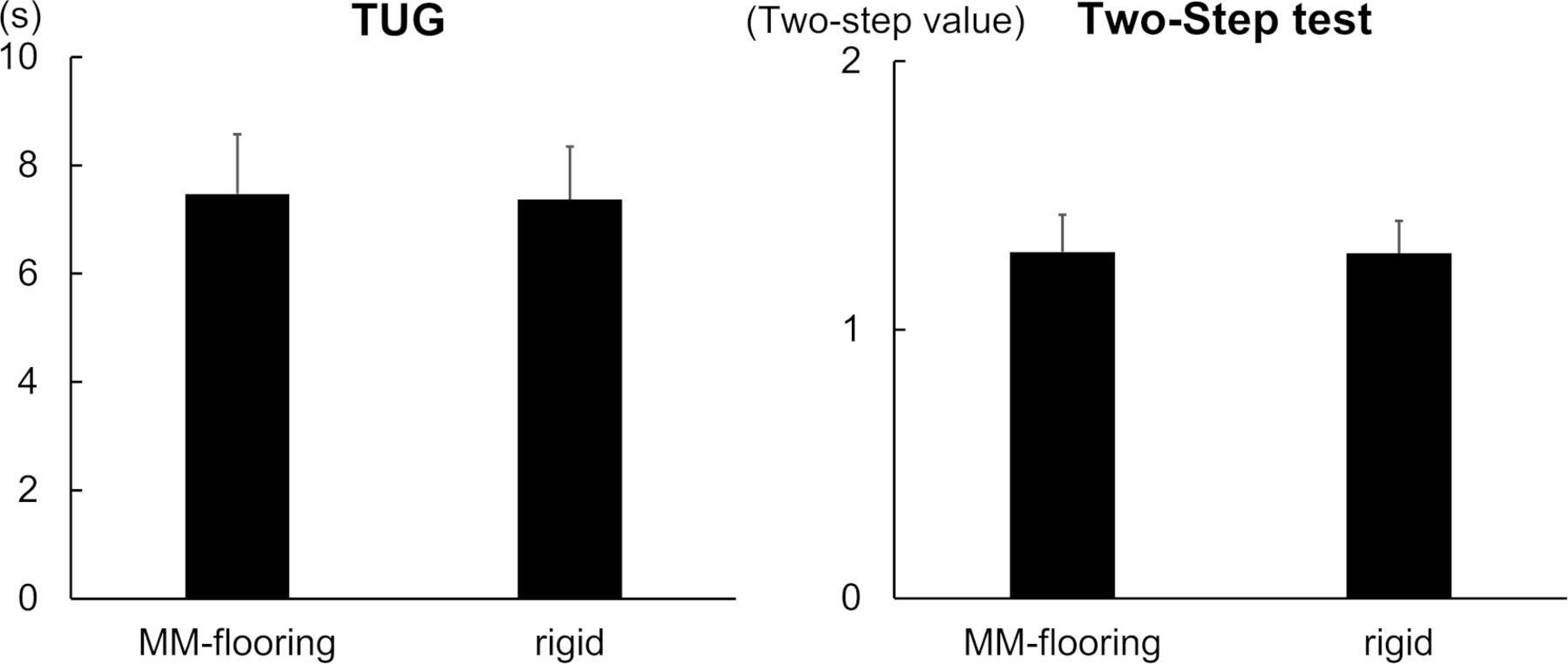
The TUG results were obtained by analysing the data of 19 participants, with the MM-flooring at 7.5±1.1 s and rigid flooring at 7.4±1.0 s (figure 4). There were no significant differences between the conditions (p=0.548). The two-step test value results were obtained by analysing the data of 19 participants, with the MM-flooring at 1.3±0.1 and rigid flooring at 1.3±0.1 as shown in figure 4. There were no significant differences between the conditions (p=0.653).

Result of the gait performance test. The mean of the gait performance test results of the 19 participants is shown. Error bars indicate SD. In the TUG test, the shorter time is the better performance. In the graph of the two-step test, the vertical axis indicates the two-step value, which is the distance between two steps divided by the height of each participant; a larger value indicates better performance. MM, mechanical metamaterial; TUG, timed up and go.
Evaluation of balance
For the rectangular area data of COP displacements, only one participant showed displacements beyond the 95% CI of the data distribution; thus, the data of 18 participants were analysed (figure 5). The values of the rectangular area with opened eyes were 5.0±2.1 cm2, 5.8±2.6 cm2 and 7.1±3.0 cm2 on the MM-flooring, rigid flooring and shock-absorbing mat, respectively. There was a main effect in the three conditions (F2, 34 = 3.821, p=0.032). The results of the post hoc test showed a significant difference between the MM-flooring and shock-absorbing mat (p=0.026).

Comparison of the rectangular area of the centre of pressure displacement under each floor condition. The mean of the rectangular area of 18 participants’ centre of pressure displacement under each floor condition of is shown. Error bars indicate SD; here, a smaller area is a better performance. *p<0.05, **p<0.001. MM, mechanical metamaterial.
The values for the rectangular area with closed eyes were 9.3±4.1 cm2, 10.6±6.8 cm2 and 21.5±10.1 cm2 on the MM-flooring, rigid flooring and shock-absorbing mat, respectively. There was a main effect in the three conditions (F2, 34 = 27.518, p<0.001). The results of the post hoc test showed a significant difference between the MM-flooring and shock-absorbing mat (p<0.001) and between the rigid flooring and shock-absorbing mat (p<0.001).
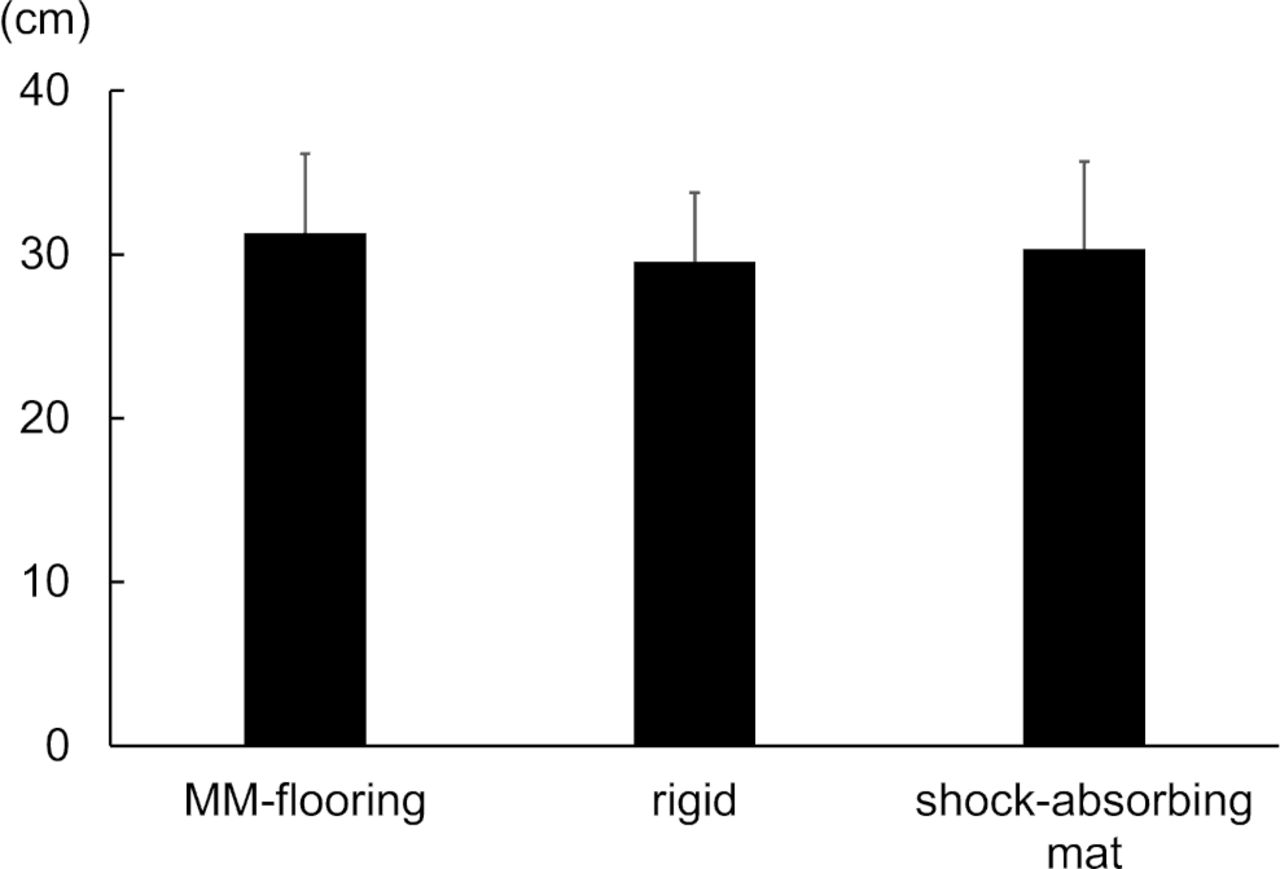
The FRT results were obtained by analysing the data of 19 participants, with that on the MM-flooring at 31.3±4.9 cm, rigid at 29.6±4.2 cm and the shock-absorbing mat at 30.3±5.4 cm (figure 6). There was no significant difference between the three conditions (F2, 36 = 2.795, p=0.074).
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Result of the functional reach test. The mean of the functional reach test results for the 19 participants is shown. Error bars indicate SD; here, the longer distance is the better performance. MM, mechanical metamaterial.
Discussion
The results of the two experiments (the shock-absorbing test, and the evaluation of gait and balance ability) showed that the newly developed MM-flooring has sufficient shock-absorption to reduce the incidence of fractures attributed to falls without affecting the gait and balance of older adults. It was suggested that the conventional problem of the balance between shock absorption and stability on standing could be solved by the structural property of MM.
In a previous study, some shock-absorbing systems that attenuated impact by approximately 47% compared with a normal floor surface were reported to have a minor effect on the standing balance of older women.6 In this study, compared with carpet tiles that have a shock-absorbing performance, the MM-flooring showed a 43.5% reduction in the impact force. Using Kleiven et al’s probability curve of hip fracture risk in the older people based on the impact force,24 the probability of hip fracture for carpet tile at the highest impact observed in the present modelling study (3.51 kN) was estimated as 70.5% for women, whereas that for MM-flooring (the highest impact force of 1.98 kN) was estimated as 29.0% for women. Thus, MM-flooring has the potential to substantially reduce the risk of fracture. In addition, there was no effect on the gait or balance when using MM-flooring, suggesting that the flooring material maintains rigidity during gait and standing and sufficiently reduces the risk of fracture when subjected to instantaneous impacts such as falls.
Economic feasibility is also an important consideration when introducing shock-absorbing flooring materials. According to the Shock-Absorbing Flooring Effectiveness SysTematic (SAFEST) review, some studies found shock-absorbent floors to dominate standard floors, which indicate lower costs and better outcomes. One study estimated that shock-absorbing floors increased both the cost and quality-adjusted life year; however, the quality of these studies is not high.25 The shock-absorbing flooring interventions have the potential to be cost-effective compared with standard flooring, while further research is required to determine whether shock-absorbing flooring is likely to increase the fall rate.26 Since reliable shock-absorbing performance and ease of mass production are important in terms of cost, the MM-flooring has a manufacturing style that is relatively easy to mass produce since the cushioning material is made of elastomer and manufactured in units of 500×500 mm area. As of February 2022, MM-flooring has been commercialised by Magic Shields named ‘Coroyawa’, and is now being sold to hospitals and nursing homes in Japan. As the number of installation cases is increasing, further research on the incidence of injuries following installation would confirm the cost-effectiveness of the MM-flooring.
This study has certain limitations. We were not able to compare the same thermoplastic elastomer material with one that had no MM structure as a control in the impact absorption test. Since the thermoplastic elastomer itself possesses a shock-absorbing effect, the effect of the shock-absorbing property of the MM structure could be more clearly demonstrated by comparing materials with different structures made with thermoplastic elastomer. Furthermore, in the evaluation of gait ability, we could not prepare adequate shock-absorbing flooring to form a walking path for the TUG and two-step tests; thus, we only compared the two groups with a rigid floor. Since a sufficient difference was observed in the balance test, a difference in gait stability is anticipated as well; however, this point needs to be examined closely. In the present study, drop-weight impact testing was performed only in one bone model of an older woman. Simulations with various models of different sex and ages are warranted to enhance the generalisability of the present results.
It was confirmed that MM-flooring has the potential to prevent fractures caused by falls and does not affect the gait or balance of older adults. Further clinical studies would confirm the effectiveness of the MM-flooring in real-world settings.
What is already known on the subject
Shock-absorbing flooring is anticipated to prevent serious injuries after falls.
There is a need to consider the effect of shock-absorbing performance and gait stability when choosing flooring materials.
What this study adds
A flooring material with a mechanical metamaterial structure demonstrated high shock-absorbing properties with no effect on the gait stability of older adults.
The possibility of solving traditional issues with a structural property has been demonstrated.
Data availability statement
Data are available upon reasonable request. The datasets generated for this study are available on request to the corresponding author.
Ethics statements
Patient consent for publication
Ethics approval
Experiment 2 involving human participants was reviewed and approved by the Ethics Review Committee of Fujita Health University (registration number HM20-270). Participants gave informed consent to participate in the study before taking part.
Acknowledgments
We would like to thank all the participants and Nagoya City Silver Human Resources Center for their cooperation in recruiting participants.
References
Footnotes
Correction notice This article has been corrected since it was first published. The open access licence has been updated to CC BY.
Contributors TT conducted the research design, data collection (Experiment 2) and analysis (Experiments 1, 2), original draft preparation, review and editing; TS developed the shock-absorbing material and performed data collection (Experiments 1, 2) and review; NK and ST assisted with the data collection, programming and review; TI and SK conceptualised the study and aided in the methodology and review; YH and HS developed the shock-absorbing materials, conceptualised the study, performed data collection (Experiment 1) and review; KM assisted in setting up the experimental environment (Experiment 1), data collection and analysis (Experiment 1) and review; and YO conceptualised the study, supervised the experiments, drafted and reviewed the manuscript, and responsible for the overall content as a guarantor of this study.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests Flooring materials were provided by Magic Shields, Inc. TS, YH and HS are company stockholders of Magic Shields, Inc. The other authors have not received any financial support and have no shares in the company.
Patient and public involvement Patients and/or the public were not involved in the design, or conduct, or reporting, or dissemination plans of this research.
Provenance and peer review Not commissioned; externally peer reviewed.