Article Text

Abstract
Objectives To determine the incidence, demographics and injury patterns involved in E-Scooter-related hospital admissions due to significant trauma compared with bicycle-related trauma within England and Wales. To compare morbidity and mortality between groups.
Design A retrospective cohort study based on data which has been prospectively collected and submitted to the UK Trauma Audit and Research Network (TARN) registry.
Setting Major trauma centres and trauma units within England and Wales.
Participants Patients of any age who were admitted to hospitals in England and Wales with injuries following E-Scooter or bicycle incidents between the dates 1 January 2021–31 December 2021. All patients must have met TARN database inclusion criteria.
Outcomes In-hospital mortality, critical care admission and length of stay (LoS), hospital LoS and discharge destination.
Results There were 293 E-Scooter trauma incidents compared with 2538 bicycle incidents. E-Scooter users were more likely to be admitted to a major trauma centre (p=0.019) or a critical care unit (p<0.001). Serious head and limb trauma (Abbreviated Injury Scale >2) occurred more frequently among the E-Scooter cohort (35.2% vs 19.7%, p<0.001 and 39.9% vs 27.2%, p<0.001, respectively) while serious chest and pelvic trauma were greater among bicycle users (p<0.001 and p=0.003, respectively). Over one-third of E-Scooter injuries were incurred outside the current legislation by patients who were intoxicated by alcohol and drugs (26%, 75/293) or under the age of 17 (14%, 41/293).
Conclusions These early results suggest a greater relative incidence of serious trauma and an alternative pattern of injury among E-Scooter users compared with bicycles.
Trial registration number TARN210101.
- Traumatic Brain Injury
- Health Education
- Public Health
Data availability statement
All data relevant to the study are included in the article.
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
WHAT IS ALREADY KNOWN ON THIS TOPIC
Prior to this study E-Scooter trauma literature primarily consisted of series of patients with minor injuries, indicating a predominance of trauma involving the head and extremities.
WHAT THIS STUDY ADDS
This is the first nationwide study of E-Scooter trauma and involves the largest number of patients with significant injuries. Injuries involving the head and limbs were the most common causes of serious E-Scooter injury and were more common than in bicycle users. Head injury caused the vast majority of critical E-Scooter-related injuries and helmets were used rarely. Over one-third of E-Scooter patients in England and Wales were under 17 or intoxicated by alcohol or drugs at the time of injury meaning they had not complied with current legislation.
HOW THIS STUDY MIGHT AFFECT RESEARCH, PRACTICE OR POLICY
Greater restrictions and safety measures may improve E-Scooter safety.
Introduction
Electric scooter (E-Scooter) use has dramatically increased in popularity as part of a global trend towards shared mobility. The purported benefits of E-Scooters include improved traffic congestion, reduced greenhouse gas emission and better air quality.1 The potential for E-Scooters to replace cars for short distance journeys such as commutes has fuelled the rapid adoption of E-Scooter rental trials globally, the first of which commenced in the USA in 2017. However, significant concerns over safety practices have stimulated debate over licensing conditions. Critics suggest that numerous factors such as rider visibility, low stability, dangerous driving practices2 3 and high rates of rider intoxication make E-Scooter use hazardous. These concerns have been substantiated within the UK Parliamentary Advisory Committee for Transport recent report,4 and by international data which reports rising rates of E-Scooter-related trauma and injury patterns predominantly involving craniofacial and extremity trauma.5 6
In the UK, E-Scooters are regarded by law as personal light electronic vehicles. Therefore, their public use is permitted only as part of rental trials, although privately owned E-scooters are used widely.4 The UK E-Scooter rental trial commenced in July 2020 and is ongoing. The trial has expanded to include 57 locations including London, which joined the trial in July 2021. To rent an E-scooter within the UK, one must be over the age of 17 and hold a minimum of a provisional driving licence. It is illegal to operate an E-Scooter while under the influence of alcohol or intoxicating substances. The UK government’s Department for Transport ran a public consultation in May 2020 (prior to trial commencement), which resulted in the relaxation of proposed regulations for E-Scooter rental trials. Following consultation, helmet use was made non-compulsory, maximum power was raised from 350 W to 500 W and the maximum permitted speed was raised to 15.5 mph from 12.5 mph.7
E-Scooters are a novel entity, for which limited research has been performed and legislation is still under consideration. The vast majority of contemporary evidence regarding E-Scooter trauma consists of single-centre or citywide case series of emergency department presentations. Within these studies, the majority of patients were discharged home with low levels of injury.6 8 9 Therefore, a detailed analysis of those suffering the most severe consequences of E-Scooter incidents has not been performed. Bicycles represent an analogous mode of transport which are used widely and have been the subject of research into safety,10 11 injury burden12 13 and outcomes.14 In recent years, greater focus on cycle safety has supported the implementation of interventions to improve their safe use such as cycle lanes and cycle filtering systems.15 16 Comparing the burden of serious injuries and outcomes between these similar transport groups may allow inferences to be made regarding the safety of E-Scooters and measures, which could reduce harm to users. The primary aim of this study is to use a nationwide approach to characterise the incidence, demographics and patterns of injury in E-Scooter users who present to hospital with serious injuries, using bicycle riders as a comparative group. Second, we aimed to determine the outcomes involved for these groups.
Methods
The Trauma Audit and Research Network (TARN) prospectively collects and maintains a registry of trauma patients admitted to hospitals in England, Wales and Ireland. A retrospective review of TARN registry data for England and Wales was performed. Information entered onto the TARN database is prospectively collected from patient medical records, radiological investigation and biochemical studies. TARN eligibility criteria includes patients of all ages who (1) were admitted to hospital for ≥3 days, required critical care admission or died in hospital and (2) sustained isolated injuries meeting minimum severity criteria.17
A TARN registry enquiry was performed for all road traffic collisions which occurred between 1 January 2021 and 3 December 2021. All incidents for which the patient was identified as an E-Scooter or bicycle rider were included. Any incident involving variations of E-Scooters which were non-electronically powered or variations of bicycle which were motorised were excluded from the analysis. Any incident in which the patient was a pedestrian or their position (as rider or pedestrian) was unclear was also excluded.
Deidentified demographic data, mode of attendance, mechanism of injury, injuries sustained, Abbreviated Injury Scale (AIS), Injury Severity Score (ISS), operative interventions performed, requirement for critical care admission and length of critical care stay, length of hospital stay, mortality and discharge destination were collated for all patients that met inclusion criteria. Patients were identified as intoxicated by alcohol or drugs based on information stated within clinical notes or biochemical testing. The AIS classifies injuries by body region according to severity according to a 6 point ordinal scale ranging from 1 (mild) to 6 (unsurvivable). For this study, serious injuries are defined as AIS >2.
Statistical analysis and figures were produced using GraphPad Prism V.9.2.0. Continuous data were compared with Mann-Whitney U tests and reported as median with IQR. Categorical comparisons were analysed using χ2 tests and reported as percentages. Statistical significance was defined as p<0.05.
Patient and public involvement
This study was conceived through direct interaction with a number of patients who were admitted to hospital with severe injuries as a result of E-Scooter collisions. An E-Scooter trauma injuries review panel was established at Imperial College Healthcare NHS Trust with attendance from representatives from the hospital trust, Transport for London and London Ambulance Service. Patients were not directly consulted regarding the design of the study.
Results
There were 293 admissions related to E-Scooter injuries and 2538 admissions related to bicycle injuries during the study period (table 1). E-Scooter riders were significantly more likely to receive care at a major trauma centre (60.4% vs 46.9%, p<0.001). Injured riders were predominantly male for both modes of transport however injured E-Scooter riders were younger than bicycle riders (median age: 35.2 years vs 50.4 years, p<0.001). Almost a sixth (14.0%) of E-Scooter riders were aged 16 or under compared with only 8.6% of cyclists (p=0.003). There was a greater than three-fold increase in alcohol/drug use for E-Scooter riders (25.6% vs 7.2%, p<0.001) and these patients were less likely to have worn a helmet (7.2% vs 47%, p<0.001) than injured cyclists.
Characteristics of E-Scooter and bicycle users
The majority of both types of incidents happened during daytime (figure 1A). However, one-third of cycling incidents occurred in the morning between 06.00 and midday (32.6%) compared with only 10.1% of E-Scooters (p<0.001). Conversely, injuries involving E-Scooters were twice as likely to occur in the evening between 18.00 and midnight compared with cyclists (41.7% vs 18.6%, p<0.001). Rate of incidents per day of the week was variable among E-Scooters (from 11.6% on Thursdays to 17.1% on Sundays), and cyclists (from 10.8% on Tuesdays to 19.6% on Mondays, figure 1B). Seasonal variation in rates of injury were observed among both groups (figure 1C). Between the months of April and September, there was a 50% increase in both E-Scooter-related injuries (119 vs 179) and bicycle incidents (973 vs 1565). The rate of E-Scooter trauma increased as the year progressed, rising from 9 cases in January to 41 cases in July.

Cumulative E-Scooter and bicycle incidents by (A) time of day; (B). day of week and (C) month of the year. P values were calculated using χ2 test. *indicates p<0.001.
While there was no difference in overall ISS, significant differences were observed in body region injuries between groups (table 2). The E-Scooter group demonstrated a higher rate of serious head injury (35.2% vs 19.7%, p<0.001) while the bicycle group experienced higher rates of serious chest injury (32.5% vs 17.1% %, p<0.001). The proportion of major trauma (ISS >15) did not significantly differ by group.
Injured region and severity of E-Scooter and bicycle users
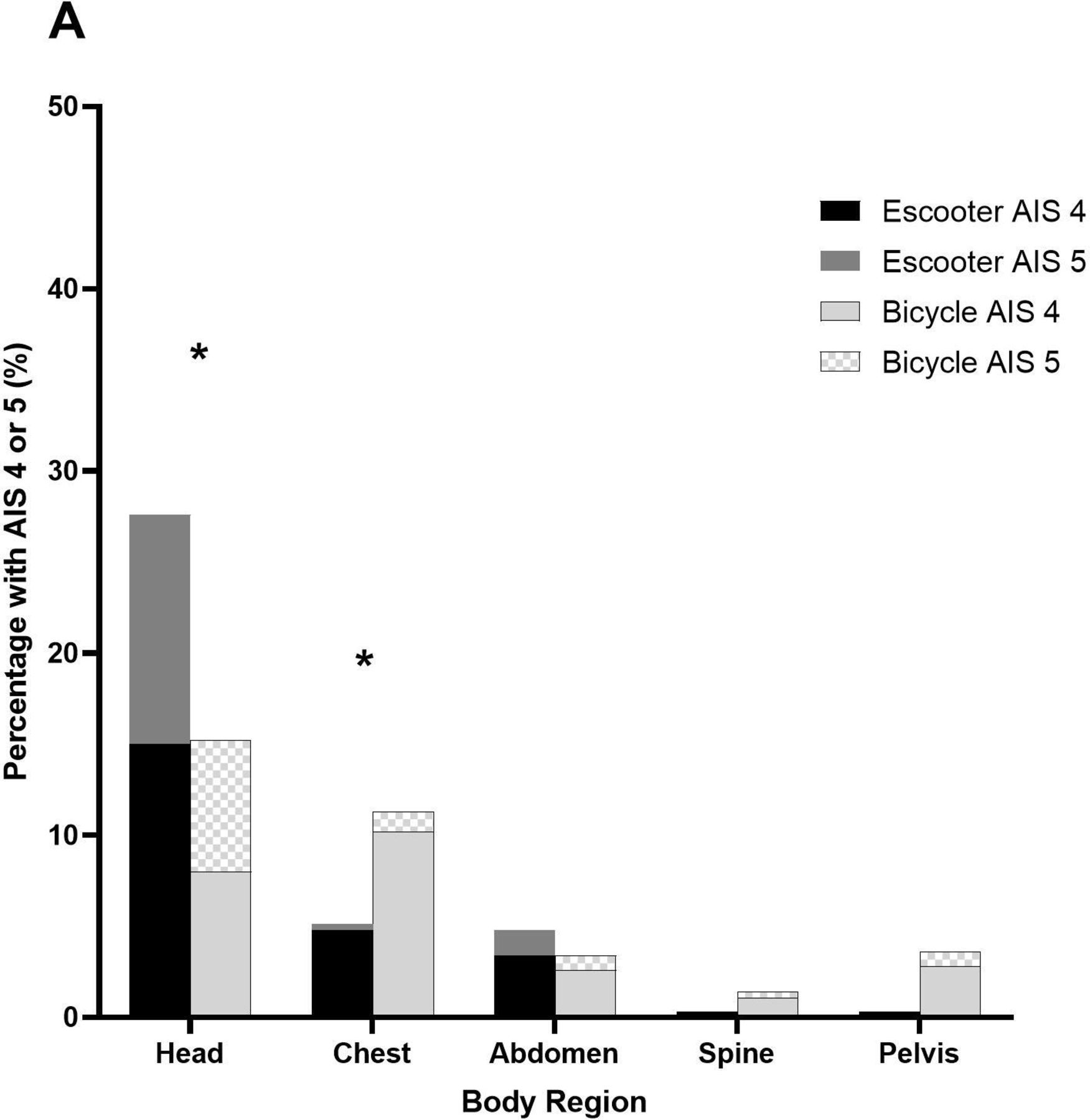
Almost twice the number of E-Scooter patients presented with severe or critical head injuries (AIS 4 or 5, 27.6% vs 15.2%, p<0.001) while double the number of bicycle patients presented with severe or critical chest injuries (5.1% vs 11.3%, p=0.001). Thirty-seven out of the 41 critical injuries (90%) which occurred in the E-Scooter group were head injuries (figure 2).
{kind=link}
{kind=link}
Injuries subdivided by body region in E-Scooter and bicycle users which were AIS 4 or 5 as a proportion of total group population. P value was calculated using χ2 test. *indicates p<0.001. AIS, Abbreviated Injury Scale.
Outcomes did not significantly differ between groups (table 3). Mortality was low for both mechanisms of injury (E-Scooters 2.7% vs cyclists 1.7%, p=0.229). Significantly more E-Scooter patients required critical care (19.8% vs 14.6%, p=0.019) but there were no differences in length of stay between groups. More than four fifths of both cohorts were discharged to home and while numbers were small, transfer for rehabilitation for cyclists was double that for E-Scooter patients (5.5% vs 2.4%, p=0.022).
Outcomes
Discussion
This is the first nationwide study to examine the characteristics, injuries and outcomes of trauma following E-Scooter use. This study considered a large data-set consisting of predominantly moderate to severe trauma due to strict TARN database eligibility criteria.17 In comparison to bicycle patients, E-Scooter patients were younger, more likely to have been injured in the evening, have consumed alcohol or drugs and were less likely to wear helmets. Head and chest injuries were a significant burden for both groups and over one-third of E-Scooter patients sustained serious traumatic brain injury (TBI). While overall mortality was low in both groups, injury following E-Scooter use was significantly more likely to result in Major Trauma Centre and critical care unit admission.
There was a ninefold greater rate of significant injury among bicycle users compared with E-Scooter users. This is similar to other published literature; a case series from Hamburg which considered all E-Scooter-related hospital presentations reported the same increase compared with bicycle-related trauma.18 Bicycle ownership in the UK during 2021 was approximately 31.6 million (47%),19 which vastly outnumbered the estimated 520 000 E-Scooters in use (500 000 privately owned and 20 000 available for rental).4 Based on these figures, bicycle use in the UK is still likely to be at least nine times greater than E-Scooter use. Therefore, it is possible that E-Scooters are resulting in higher rates of trauma than bicycles. However, further detailed statistics regarding the number of trips being made by both methods of transport is required to directly compare the two. Only one other peer-reviewed study has taken a nationwide approach in quantifying E-Scooter-related morbidity and mortality. Tan et al’s review of the Singapore National Trauma Registry found that motorised devices had three times the rate of severe injury when compared with non-motorised counterparts,20 although this included all forms of motorised personal mobility devices and the study did not take an E-Scooter-specific approach. Over one-third of injuries were sustained by those operating E-Scooters outside the parameters of current legislation; 41 riders were children under the age of 16, and therefore, unable to hold a driving licence and a further 75 demonstrated evidence of intoxication with alcohol or drugs. This represents a conservative estimate given that not all intoxicated patients may have been routinely tested or identified on admission to hospital.
Our study revealed the differing injury patterns among E-Scooter users compared with bicycle users, who experienced twice the number of serious head and significantly more extremity injuries. This data echoes a recent systematic review of E-Scooter injuries which found the limbs and the head to be the most frequently injured body regions, with falling being the most common mechanism of injury.21 While other studies have report high rates of head injury among E-Scooter users,6 22 this study is the first to demonstrate the overall high severity of head injury encountered. The majority of E-Scooter users with head injuries, sustained injuries categorised as severe or critical (AIS 4 or 5) and higher AIS scores correlate with a higher relative risk of threat to life.23 Despite this, few riders in this study wore helmets, which is in keeping with US data reporting helmet use in no more than a quarter of patients.6 24 25 Helmet use is associated with reduced rates of TBI in cyclists,10 11 26 and has been shown to reduce the risk of head injury among a small cohort of E-Scooter users (OR: 0.18, p=0.029).27 In contrast to the UK, helmet use while riding E-Scooters in Australia is compulsory rather than recommended and rental companies provide helmets at the point of use. Consequently, helmet compliance has been observed to be substantially higher between 61.4% and 95.5%.28
From a resource perspective, E-Scooter use was associated with a higher rate of admission to MTCs and critical care units. This may be related to the higher rates of TBI among E-Scooter users, but the exact reasons for these differences require further national investigation.
Areas for further research and limitations
This study only includes injuries to E-Scooter riders with no measure of injury to pedestrians or other road users who may be involved in an E-Scooter-related incident and may therefore under-represent the true burden of injury from this mode of transport. Furthermore, only patients who were admitted to hospital are included in the TARN database, and therefore, overall mortality rates which include death at the roadside may reveal a higher mortality from E-Scooter use than reported here. Finally, a significant proportion of E-Scooters are privately owned and ridden illegally. While rental companies have made some effort to encourage safe use of E-Scooters with the introduction of mechanisms such as speed limitation during first use, preuse quizzes and restriction on location of use, private users of E-Scooters are not subject to these limitations. It was therefore beyond the scope of this study to measure the effect that rental trial enrolment had on rates of injury and safe use, but this represents an area for further research. Finally, some COVID-19 travel restrictions were in place in early 2021, representing a small proportion of the period of data collection. At present, E-Scooter use continues to rise so further study is required in order to monitor the growing impact in the fullness of time.
Conclusions and implications
E-Scooters are an emerging mode of transport in the UK, and full characterisation of rates and types of injury will require ongoing study. However, these preliminary results indicate that E-Scooter use may result in a higher relative rate of hospital admission due to significant trauma than bicycles and in particular, higher rates of severe head injury. As the number of E-Scooter trips taken continues to grow, further legislation and tighter regulation of E-Scooter rental are required to reduce the already significant burden of injury associated with this mode of transport.
Licensing
The corresponding author has the right to grant on behalf of all authors and does grant on behalf of all authors, an exclusive licence on a worldwide basis to the BMJ Publishing Group to permit this article to be published in BMJ editions and any other BMJPGL products and sublicences such use and exploit all subsidiary rights, as set out in our licence.
Data availability statement
All data relevant to the study are included in the article.
Ethics statements
Patient consent for publication
Ethics approval
TARN has Health Research Authority approval (Patient Information Advisory Group (PIAG) Section 251) for research on the anonymised data it holds from NHS Trusts. Local approval by the NHS Trust was granted by the trust Caldicott Guardian and a formal data transfer agreement was completed.
Acknowledgments
With thanks to Paul Symonds, data analyst and all members of the Trauma, Audit and Research Network team.
References
Footnotes
Contributors RC, EP and CA conceived of the work and acquired the data. All authors designed the study, are responsible for implementation of the study and jointly drafted the manuscript. RC performed statistical analysis. All authors analysed the data, revised the manuscript and approved the final version submitted for publication. CA takes responsibility for and is guarantor of all aspects of the work. The corresponding author attests that all listed authors meet authorship criteria and that no others meeting the criteria have been omitted.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests All authors have completed the Unified Competing Interest form (available on request from the corresponding author) and declare: no support from any organisation for the submitted work; no financial relationships with any organisations that might have an interest in the submitted work in the previous three years, no other relationships or activities that could appear to have influenced the submitted work. CA is responsible for the overall content as the guarantor.
Patient and public involvement Patients and/or the public were not involved in the design, or conduct, or reporting, or dissemination plans of this research.
Provenance and peer review Not commissioned; externally peer reviewed.