Article Text

Abstract
Objective To quantify the effects of increased cycling on both mortality and morbidity.
Design Health Impact Assessment.
Setting Cycling to place of work or education in Copenhagen, Denmark.
Population Effects were calculated based on the working-age population of Copenhagen.
Main outcome measures The primary outcome measure was change in burden of disease (measured as disability-adjusted life years (DALY)) due to changed exposure to the health determinants physical inactivity, air pollution (particulate matter <2.5 μm) and traffic accidents.
Results Obtainment of the proposed increase in cycling could reduce the burden of disease in the study population by 19.5 DALY annually. This overall effect comprised a reduction in the burden of disease from health outcomes associated with physical inactivity (76.0 DALY) and an increase in the burden of disease from outcomes associated with air pollution and traffic accidents (5.4 and 51.2 DALY, respectively).
Conclusion This study illustrates how quantitative Health Impact Assessment can help clarify potential effects of policies: increased cycling involves opposing effects from different outcomes but with the overall health effect being positive. This result illustrates the importance of designing policies that promote the health benefits and minimise the health risks related to cycling.
This is an open-access article distributed under the terms of the Creative Commons Attribution Non-commercial License, which permits use, distribution, and reproduction in any medium, provided the original work is properly cited, the use is non commercial and is otherwise in compliance with the license. See: http://creativecommons.org/licenses/by-nc/2.0/ and http://creativecommons.org/licenses/by-nc/2.0/legalcode.
Statistics from Altmetric.com
Article summary
Article focus
-
Estimation of the overall health effects of cycling to work or place of education.
-
Analysis of effects on both mortality and morbidity.
Key messages
-
Cycling has both positive and negative health effects, but overall, the health effects of cycling are beneficial.
-
The negative effects of air pollution and accidents should be prevented in order to maximise the health effects of policies aiming to increase cycling.
Strengths and limitations of this study
-
Estimation of the effect in a real population, accounting for present exposure.
-
Inclusion of effect on both mortality and morbidity.
-
Simple model of calculation but with modest data requirements.
Introduction
Physical inactivity is a major risk factor for numerous diseases, including cardiovascular diseases and several cancer forms.1 Active transportation, including transportation by bicycle, is a way of incorporating physical activity into everyday life and can thus contribute to public health gains by increasing the level of physical activity in the population. However, cycling also entails greater risk of accidents and exposure to air pollution.2–4 The aggregated health effect of policies aiming to increase transportation by bicycle should therefore be estimated prospectively.
Health Impact Assessment (HIA) can be used for this purpose, hereby contributing to informed policymaking and priority setting. HIA can be used to estimate the health effects of a broad array of policies or projects in different sectors and have especially been applied to areas such as transportation, social services and housing.5 ,6 Despite the possible advantages of quantification, most HIAs performed to date have used a qualitative approach.7
Recent studies have shown that the health benefits of cycling outweighed the risks. However, most of these studies investigated the effects of increased cycling on mortality only, omitting the effects on morbidity.4 ,8 ,9 The aim of this study was to undertake a quantitative HIA of increased cycling to place of work or education in Copenhagen, calculating net health effects by summing up positive and negative effects on mortality and morbidity.
Methods
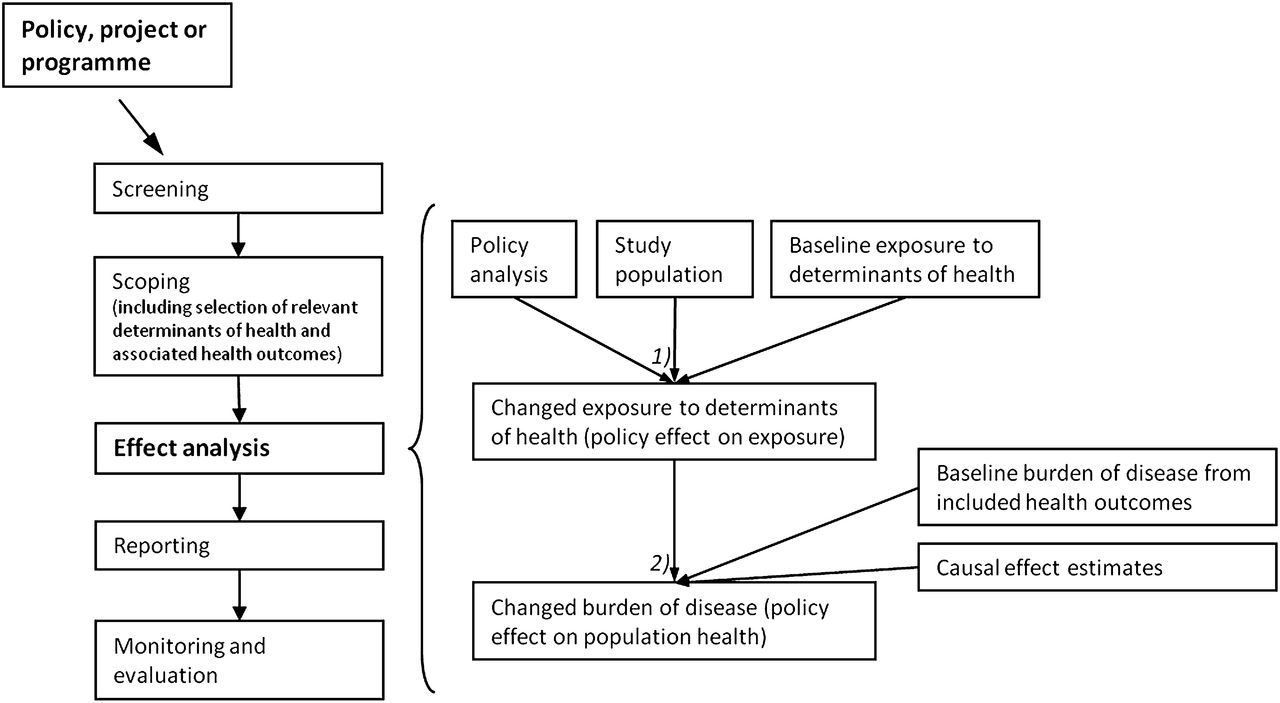
We performed a quantitative HIA of a policy goal of the City of Copenhagen regarding a modal shift from car to bicycle. Figure 1 shows the analytical approach used in the study: left illustrating the overall HIA process and right showing in more detail the approach used for quantification in the effect analysis stage. The analysis consisted of two analytical steps: (1) the effect of the policy on population exposure to determinants of health and (2) the effect of this changed exposure on population health. We used a Burden of Disease approach to assess the effect of increased cycling on both mortality and morbidity. The methods and data sources used for assessing change in exposure and health effects are outlined below.

Overview of the process of health impact assessment with specific focus on quantitative effect analysis. The left side of the figure shows a generalised Health Impact Assessment process, while the right side focuses on the effect analysis stage, involving two subanalyses: (1) the potential effects of the policy on population (or subpopulation) exposure to selected determinants of health (changed exposure) were estimated based on an analysis of the policy, study population characteristic and information on baseline level of exposure to determinants of health. (2) Next, the potential effect of changed population exposure to determinants of health on burden of disease was estimated based on the results of the first subanalysis (change in exposure to health determinants), information on baseline level of burden of disease from the included health outcomes and causal effect estimates of the associations between included determinants of health and health outcomes. The change in burden of disease was estimated for both each determinant of health and each health outcome and aggregated for all included health outcomes (model was developed based on7).
Policy proposal and study population
Today, one in three travels to work or place of education in Copenhagen by bicycle. The target of the City of Copenhagen is to increase this to 50% by 2015.10 As a first step, it has been proposed to transfer half the car trips of 2–10 km and one-third the car trips of 10–15 km to cycling, which would increase the proportion of cyclists to 42%.10 We tested the health impacts of this scenario. The study population consisted of all people travelling to place of work or education in Copenhagen, irrespective of mode of transport (table 1).
Change in travel mode for persons travelling to place of work or education in Copenhagen, distributed on mode of transport and travel distance, before and after the policy intervention (rounded numbers)10
Individual-level data or information regarding specific travel routes was not available for the study population. This complicated estimation of exposure and outcome levels and led to the results being reported in absolute numbers for the study population only, not generalised to the Danish population. To obtain the best comparability with the study population, exposure data from individuals living in municipalities within the included travel distance from Copenhagen only were included in the analysis. Furthermore, the population was limited to the age group 15–69 years since this age group was in best accordance with both the study purpose and WHO's age-specific estimates of burden of disease.11
Determinants of health
Our main factor of interest was change in travel pattern for people travelling to place of work or education in Copenhagen on weekdays. The health effect of this factor was mediated through exposure to specific determinants of health. These determinants were identified in the scoping stage of the HIA (figure 1). Based on reviews of Danish and international epidemiological literature on transportation and health,i physical inactivity, air pollution and road traffic accidents were found to be relevant to include as determinants of health in the effect analysis (figure 2).

{kind=link}
{kind=link}
Analytical model of the health impact assessment of increased cycling to place of work or education. The figure illustrates the relationship between policy proposal, relevant health determinants, health outcomes and aggregated effect.
Estimation of exposure levels of the included determinants of health before the proposed policy intervention and calculation of the potential change in exposure due to a modal shift were based on the following data sources:
Exposure to physical inactivity at baseline was estimated based on data from a postal health survey from 2010, where physical activity was measured as minutes spent weekly on moderate or vigorous physical activity during leisure time and active transportation (see Hammer-Helmich et al,12 specific data extracted for the study population). Physical activity was not analysed as a continuous variable, but categorised according to the current recommendations as (1) sufficiently active: >60 min activity daily, (2) moderately active: 30–60 min activity daily and (3) inactive: <30 min activity daily,1 ,13 hereby obtaining agreement with the causal exposure estimates used in the analysis. The population that could be shifted from car to bicycle consisted of those who spent <15 min a day on active transportation at baseline since it was assumed that these did not already cycle to work or place of education. Change in the proportion of the population being physically inactive, moderately active and sufficiently active was then calculated based on the baseline distribution of physical activity and increase in time being physically active (calculated based on kilometres travelled by bicycle and average speed of cycling).10
Due to risk of double counting, air pollution was restricted to fine particulate matter (PM2.5), although evidence suggests that other components can also affect health.14 ,15 Baseline exposure level was estimated from data on PM2.5 concentration in Copenhagen (see Ellermann et al,16 specific data extracted for the study population) and information regarding 1 min ventilation,3 ,17 travel speed,2 ,10 mode and distance.10 To describe the level of PM2.5 in traffic, the average value from two street monitoring sites was used (18.23 μg/m3),16 whereas the average from an urban and a rural background measurement site was used for non-traffic exposure (13.83 μg/m3).16 For travel speed, we used estimates from a Danish study and differentiated between car and bicycle (21.0 and 15.8 km/h, respectively),2 hereby including the health effect of longer exposure to air pollution when cycling due to lower speed. In congested traffic, travelling by bicycle can be faster than by motorised transport, but since the study population travel both within Copenhagen and in the surrounding municipalities, we applied the average of speed in congested and normal traffic to describe travel speed by car.2 One-minute ventilation was calculated as an average of the estimates reported by van Wijnen et al and Zuurbier et al (12.1 l/min for car drivers and 26.1 l/min for cyclists).3 ,17 Change in exposure to air pollution was calculated based on the changes in travel mode. A possible decrease in the level of air pollution due to less travel by car was not included in the analysis but is likely to be an extra benefit of increased travel by bicycle.18 ,19
Exposure to accidents was calculated as the number of accidents per million passenger kilometres travelled by bicycle and car, respectively. This was based on travel data from the Danish National Travel Survey (see Brems and Munch,20 updated and specified data extracted for the study population) and police-reported accident data from Statistics Denmark.21 Change in exposure to accidents was calculated based on the amount of kilometres shifted to cycling.
Health outcomes
In the scoping stage of the HIA (figure 1), health outcomes causally associated with the included determinants of health were identified. Based on the results of WHO's Comparative Quantification of Health Risks Study and an updated literature search,ii we included the following: ischaemic heart disease, ischaemic stroke, type II diabetes, breast cancer, colon cancer, cardiopulmonary diseases, lung cancer and injuries (figure 2).
Burden of disease
The potential health effect of changed exposure to the included determinants of health was calculated using a burden of disease approach, applying disability-adjusted life years (DALY) as the measure of health. DALY is a summary measure of health, which expresses the combined effect of disability and mortality: DALYs for a disease or health condition are calculated as the sum of the years of life lost (YLL) due to premature mortality in the population and the years lost due to disability (YLD) for incident cases of the health condition.22 This is advantageous when estimating the overall effect of a policy since the relationship between mortality and disability often varies for different outcomes.23 ,24 DALY valuates diagnosed health states, hereby enabling the estimations to be based on epidemiological evidence of disease-specific associations, impact calculations and WHO's calculations of burden of disease, leading to higher comparability and validity.25 There is, however, ongoing discussion regarding the use of DALY, especially due to the value judgements involved, for example, discounting and age weighting.26 ,27
Burden of disease in the study population before an increase in cycling was calculated using WHO's burden of disease estimates for Denmark.28 To account for the selected age groups in the study population, the Danish estimates were adjusted for the age distribution of burden of disease in WHO subregion EUR-A (consisting of Denmark and other Western European countries).11 This distribution was used since age-specific estimates of burden of disease are not available at country level. Estimates of burden of disease were calculated for all health outcomes included in the analysis (see table 3 for baseline estimates and notes regarding specific calculations).
A preliminary calculation of burden of disease in Copenhagen has shown that the burden of disease from accidents was lower in Copenhagen and surrounding municipalities than in Denmark overall.29 The baseline estimate of burden of disease from accidents was therefore adjusted to account for this difference. No differences were found for the other outcomes included in our analysis.29
Change in burden of disease was calculated using the potential impact fraction (PIF), an epidemiological method to estimate the effect of an exposure on population health, expressed as the change in incidence of disease if an exposure is modified.30 ,31 PIF was calculated for each of the included associations between determinants of health and health outcomes. Calculation of PIF requires information regarding the proportion of the population being exposed before and after the intervention and estimates of the RR for each exposure category of the included associations.
Estimates of RR from WHO's Comparative Quantification of Health Risks study were used to describe the association between physical inactivity or air pollution and associated health outcomes (table 2).1 ,14 For air pollution, the RR estimates were transformed to account for differences in air pollution exposure due to differences in duration (travel speed), concentration and ventilation between car drivers and cyclists (applying the method described by de Hartog et al).4
Estimates of RR for the included association between determinants of health end health outcomes
Estimated pre-intervention and post-intervention annual burden of disease in the study population
Due to the complexity of traffic accidents and the many possible injury outcomes, no studies have estimated the RR associated with bicycle accidents. The risk of travel by bicycle relative to car was therefore calculated for the study population as the ratio of the injury rates per million kilometres travelled by bicycle and car, respectively (table 2).
For each of the included health outcomes, change in burden of disease was calculated based on the PIF and the burden of disease at baseline (BoDafter=BoDbaseline(1 − PIF)).32 For each determinant of health, the related burden of disease was calculated as the sum of the burden of disease estimates from all health outcome associated with this determinant of health. Lastly, the overall change in burden of disease in the study population was calculated by summing the estimates of change in burden of disease from all included health outcomes.
Results
Overall, the proposed policy intervention would change the share of cyclists from 35.5% to 42.4%. Pre-intervention 28.9% of the population was inactive, 29.5% moderately active and 41.6% sufficiently active. Obtainment of a shift in travel mode would change this distribution to 25.5%, 30.2% and 44.2%, respectively. For air pollution, people travelling by bicycle were exposed to a concentration of PM2.5 of 15.7 μg/m3, while people travelling by car were exposed to 18.2 μg/m3 PM2.5. The number of fatal or serious injuries was 0.18 and 0.01 per million kilometres travelled by bicycle or car, respectively.
Table 3 shows the pre-intervention and post-intervention annual burden of disease in the study population. If the proposed increase in cycling could be reached, the burden of disease could be reduced by 19.5 DALY (from 13 625.6 to 13 606.1 DALY). For outcomes related to physical inactivity, the burden of disease decreased by 76.0 DALY (from 5634.8 to 5558.7 DALY), whereas the burden of disease from outcomes related to air pollution and traffic accidents increased by 5.4 DALY (from 9784.3 to 9789.7 DALY) and 51.2 DALY (from 303.2 to 354.3 DALY), respectively.
To test the robustness of our results, we carried out selected sensitivity analyses (results not shown). We tested the uncertainty associated with the RR estimates used, by calculating the burden of disease based on upper and lower 95% CI limits. This ranged from 13.8 DALY using low RR to 24.3 DALY using high RR estimates.
In the analysis, we assumed that change in travel mode was independent of current level of leisure-time physical activity. We tested what the potential health effect would have been if it was assumed that all those shifted to cycling were physically inactive at baseline. This would lead to a fourfold increase in the health gain compared with the primary analysis, decreasing the burden of disease by 90.2 DALY.
Finally, we tested the implications of our assumption of equal outcome severity from bicycle and car accidents. To do this, we calculated PIF for fatal and non-fatal accidents, respectively, based on the relative share of bicycle and car accidents of all fatal and non-fatal traffic accidents and estimates of risk of travel by bicycle relative to car for fatal and non-fatal accidents. We then split the burden of disease from traffic accidents in terms of years of life lost (YLL) and years lost due to disability (YLD), based on the distribution of YLL and YLD in the burden of disease from traffic accidents in WHO's subregion EUR-A since estimates of YLL and YLD are not available at country level.11 This calculation showed that fatal accidents caused 39.8 DALY and non-fatal accidents caused 9.8 DALY, summing to a total of 49.5 DALY: a slightly lower increase in burden of disease than found in the main analysis (51.2 DALY).
Discussion
Principal findings
Our results showed that if the share of people travelling to work or place of education by bicycle increased from 35% to 42%, the burden of disease in the study population would decrease. This overall effect was composed of a reduction in the burden of disease from health outcomes associated with physical inactivity and an increase in the burden of disease from outcomes associated with air pollution and bicycle accidents. Our results thus showed that increased cycling was associated with both positive and negative effects that partly cancelled out. This result illustrates the importance of designing policies that promote the health benefits and minimise the health risks related to cycling.
Our overall result, that the positive health effects of increased cycling outweigh the negative effects, agrees with the findings of other studies that have estimated the effects of cycling.4 ,8 ,9 ,18 ,35 However, compared with de Hartog et al 4 and Rojas-Rueda et al,8 we found a relatively larger effect of accidents, as was also found by Woodcock et al 18 This might be explained by many bicycle accidents being non-fatal since the studies by Hartog et al 4 and Rojas-Rueda et al 8 only analysed the effects of cycling on mortality.
Our results showed a smaller health effect of increased cycling than found by de Hartog et al and Woodcock et al 4 ,18 However, these studies modelled changes in larger fictive populations, whereas we modelled the potential effects of a real policy goal formulated by the City of Copenhagen. This is in line with Rojas-Rueda et al 8 who estimated the effects of an implemented intervention. Compared with the scenarios analysed in the studies by Lindsay et al 9 and Rabl et al 35 our study included longer commuter trips (up to 15 km). This could result in larger health benefits for the individual, but might also make it harder to obtain the stated policy.
The study by Rojas-Rueda et al has been criticised for overstating the increase in physical activity attributable to the bicycle scheme analysed.36 In our analysis, we assumed that only people spending l<15 min a day on active transportation at baseline could be shifted to cycling. We did not assume that all people shifted from driving to cycling were physically inactive at baseline but included estimates of the baseline distribution of physical activity in the study population to account for existing activity. Our sensitivity analysis showed that the health gain could be increased fourfold if the entire population shifted to cycling changed their level of physical activity from inactive to moderately or sufficiently active. This might account for some of the lower benefit of physical activity found in our study compared with other studies.4 ,9 This also illustrates the importance of motivating currently inactive commuters to use active transportation.
Methodological strengths and weaknesses
Where possible, our modelling of the effects of cycling was based on local data; however, a general limitation when performing impact assessments is data availability. We were only able to include associations between determinants of health and health outcomes for which there was quantifiable evidence. This meant that health effects of, for example, stress and other psychosocial exposures were not included in the analysis, although there is some evidence that these outcomes could be affected by a change in mode of transport.37 ,38 This might imply that the health benefits from increased cycling could be greater than shown by our analysis. When modelling the possible future impacts, it was necessary to make assumptions. The influence of selected central assumptions was tested in sensitivity analyses (described above).
The associations between the included determinants of health and health outcomes were described using estimates of RR. Estimates from the WHO study Comparative Quantification of Health Risks were used for health outcomes related to physical inactivity and air pollution.1 ,14 These estimates were based on reviews and meta-analyses and provided high validity.
Evidence on the precise relation between increase in cyclists and change in accident incidence is on the other hand lacking.39 ,40 The RR of injuries was therefore calculated from the accident rate per million kilometres travelled by bicycle versus car, based on register and survey data (see Brems and Munch20 (updated and specified data extracted for the study population) and statistics Denmark21). Thus, there is greater uncertainty attached to the estimates of change in burden of disease from injuries than from the other health outcomes included in the analysis. Research on transportation and safety has indicated the possibility of a safety-in-numbers effect, where a higher proportion of cyclists are associated with a relatively lower risk of accidents.40 ,41 In our calculations, this effect was not assumed since there is lack of knowledge on the precise association between cyclist numbers and accident risk. It can also be questioned if the trend will continue to exist above a certain amount of cyclists, when drivers and bicyclists learn to coexist, or whether the effect is due to a focus on traffic management rather than the sheer number of cyclists.42 However, in recent years in Copenhagen, the number of cyclists has increased and the number of accidents has decreased,10 proposing that our estimate of the change in burden of disease from accidents might be overestimated. This indicates a need for further research on bicycle accidents and the association between increased numbers of cyclists, safety and accident trends.
Traffic accidents can result in a wide range of health outcomes resulting in very different burden of disease. We did not have knowledge on the exact injury outcomes but calculated the burden of disease from accidents based on WHO's estimate of burden of disease from road traffic accidents, which also includes a diverse mix of outcomes, and the relative distribution of traffic accidents involving different road users and vehicles in Denmark. We, thus, assumed equal outcome severity from bicycle and car accidents. In the sensitivity analyses, we tested the implications of this assumption by separating fatal and non-fatal accidents. This analysis suggested that our results might have slightly overestimated the burden of disease from bicycle accidents. However, the main analysis was not separated into relative contributions from mortality and morbidity due to lack of country-specific data on YLL and YLD.11
Only bicycle and car accidents that caused police-reported fatal or serious injuries were included in the analysis due to non-complete registration of accidents causing mild injuries.43 We believe that this did not affect our results greatly since reporting of accidents causing fatal or serious injuries, which contributes mostly to the burden of disease, is almost complete.43
We used the PIF to calculate change in population health due to changes in exposure to selected health determinants. For health outcomes affected by several determinants, fractional measures such as PIF can sum to more than one, implying that more than 100% of disease cases are preventable.44 This problem arises when exposures interact. To avoid overestimation, the potential preventive effect should be calculated sequentially. In our analysis, only the health outcome ischaemic heart disease was affected by more than one of the included health determinants. For this outcome, the change in burden of disease was calculated for both possible sequences of changed exposure, which did not alter the results. We assumed that burden of disease from outcomes related to the same determinant of health was not affected by comorbidity, an assumption also applied by WHO in calculations of burden of disease.27
The approach presented here is a fairly simple model of calculation that does not include a time dimension, competing risks or demographic factors. Furthermore, the calculations were based on expected changes in incidence, whereas changes in duration or severity (disability weights) were not included. However, with modest data requirements, it gives an estimate of the potential health effects of a policy proposal.
Our results and the methods applied have certain limitations, which points towards future research questions. These include further development of methods for quantitative HIAs and how to better include social and psychological health effects in quantitative assessments. Other important research areas relate more specifically to transportation and the systemic nature of transport. This includes a specific need for further research on accidents and the association between numbers of cyclists and risk of accidents and also the wider implications of transport such as effects on climate change, access to goods and services and social connection in communities.
Conclusions
Decision makers or stakeholders often request quantified estimates of the potential effects of prospective policies or projects. Our study illustrates an approach to quantitative risk assessment in HIA, and our results showed that it could have overall beneficial health effects to reach the preliminary aim of the City of Copenhagen of 42% cycling among those travelling to work or place of education. Numerically, the net health effect was moderate, which was partly due to the modelled scenario only including a relatively small population. Partly this was also a result of the burden of disease from health outcomes related to physical inactivity decreasing while the burden of disease from outcomes related to air pollution and accidents increased. The potential health gain was, however, more than a third larger than the potential health loss.
Our result, where positive and negative effects partly cancelled out, illustrates how quantitative HIA can help clarify the underlying elements that contribute to the effects of a policy. This result points to the policy relevant conclusion that it is important to focus on improving cycling safety and reducing the exposure of cyclists to air pollution. This would enhance the health gains potentially obtainable through increased cycling.
Acknowledgments
We would like to thank the Research Centre for Prevention and Health, Capital Region of Denmark, the Technical and Environmental Administration, City of Copenhagen and the Department of Transport, Technical University of Denmark for providing data.
References
Footnotes
-
To cite: Holm AL, Glümer C, Diderichsen F. Health Impact Assessment of increased cycling to place of work or education in Copenhagen. BMJ Open 2012;2:e001135. doi:10.1136/bmjopen-2012-001135
-
Contributors ALH was the main contributor to data analysis and writing of the article. FD contributed to the design of the study, interpretation of data and drafting of the article. CG supplied parts of the data material and contributed with important revisions of article drafts. All authors approved the final version of the article.
-
Funding This research received no specific grant from any funding agency in public, commercial or not-for-profit sectors.
-
Competing interests None.
-
Provenance and peer review Not commissioned; externally peer reviewed.
-
Data sharing statement Study data are available from the corresponding author upon request (e-mail: asho{at}sund.ku.dk).
-
↵i Searched PubMed (search term: ‘Transportation’ (MeSH) and ‘Health’ (Mesh)), Cochrane Collaborations Library (search term ‘Traffic and health’ and ‘Commuting’) and the Danish Medical Journal's database (search term ‘Transport og sundhed’ [Transport and health] and ‘Aktiv transport’ [Active transportation]). Furthermore, reference lists of relevant publications were reviewed.
-
↵ii PubMed MeSH search terms: “(Motor activity OR Exercise)” “AND” “Cardiovascular Diseases” or “Diabetes Mellitus Type 2” or “Neoplasms” or “Musculoskeletal Diseases” or “(Depression OR Depressive Disorder)”. Cochrane Collaborations Library search term: “(Physical inactivity OR physical activity OR exercise)” “AND” “cancer” or “cardiovascular disease” or “type 2 diabetes” or “musculoskeletal*” or “depression”. To examine whether special circumstances existed for the health effects of cycling, the Danish Medical Journal's database was searched using the broad keywords “Cykling – Sundhed [Cycling – Health]”.