Article Text

Abstract
Considered from medical, social or economic perspectives, the cost of musculoskeletal injuries experienced in the workplace is substantial, and there is a need to identify the most efficacious interventions for their effective prevention, management and rehabilitation. Previous reviews have highlighted the limited number of studies that focus on upper extremity intervention programmes. The aim of this study was to evaluate the findings of primary, secondary and/or tertiary intervention studies for neck/upper extremity conditions undertaken between 1999 and 2004 and to compare these results with those of previous reviews. Relevant studies were retrieved through the use of a systematic approach to literature searching and evaluated using a standardised tool. Evidence was then classified according to a “pattern of evidence” approach. Studies were categorised into subgroups depending on the type of intervention: mechanical exposure interventions; production systems/organisational culture interventions and modifier interventions. 31 intervention studies met the inclusion criteria. The findings provided evidence to support the use of some mechanical and modifier interventions as approaches for preventing and managing neck/upper extremity musculoskeletal conditions and fibromyalgia. Evidence to support the benefits of production systems/organisational culture interventions was found to be lacking. This review identified no single-dimensional or multi-dimensional strategy for intervention that was considered effective across occupational settings. There is limited information to support the establishment of evidence-based guidelines applicable to a number of industrial sectors.
- GATE, generic appraisal tool for epidemiology
- RCT, randomised controlled trials
- VDU, visual display unit
Statistics from Altmetric.com
- GATE, generic appraisal tool for epidemiology
- RCT, randomised controlled trials
- VDU, visual display unit
One of the major problems facing industrial countries is work-related musculoskeletal disorders.1 Recent literature suggests that the incidence of such injuries may continue to rise owing to increased exposure to workplace risk factors,2 more segmented and repetitive work, increased mechanisation and shifts in working practices towards the service and information sector.3
There are direct health costs associated with the rehabilitation of workers with musculoskeletal injuries, and also significant economic costs are imposed on the industry as a result of compensation, lost productivity and retraining.4 The magnitude of the problem in financial terms has been estimated in the US to be as much as US$54 billion per year.1
Workers affected by work-related musculoskeletal disorders are often afflicted by long-term pain, loss of function and disability. For the effective prevention and management of such disorders, national organisations (eg, National Institute for Occupational Safety and Health, USA; Health and Safety Executive, UK; Occupational Safety and Health, New Zealand) have often implemented a variety of single-dimensional and multi-dimensional programmes involving medical, physical and psychosocial interventions. As intervention approaches within an industrial setting are often complex and evolving, they require evidenced-based models to be effective.1
Any evaluation of the potential benefits of interventions is difficult. However, the work of Westgaard and Winkel5 provides a model for the classification of interventions, thereby allowing a review of the literature to be undertaken in a structured manner. Westgaard and Winkel5 categorised intervention strategies into three main groups: mechanical exposure, production systems/organisational culture and modifier interventions. Mechanical exposure interventions typically focus on changing the design of tools, such as the computer mouse or keyboard. Production systems interventions, however, generally implement changes to the material production and/or the organisational culture of a company. The latter may involve team building and increased worker participation in the problem-solving of workplace production (ie, participatory ergonomics). Finally, interventions that incorporate specific training of workers to manage exposure levels to physical and psychosocial stressors are termed modifier interventions. These may involve an exercise programme and/or ergonomic education.
Previous reviews have highlighted a dearth of literature examining the effectiveness of intervention approaches for the prevention and management of neck/upper extremity musculoskeletal conditions.6–9 Furthermore, many of the experimental studies included in these reviews have been of low quality and few have included randomised controlled trials (RCT). Thus, the opportunity to establish effective evidence-based management programmes for work-related musculoskeletal disorders has been restricted. Therefore, there is a need to update our current knowledge using a systematic approach. The aim of this study was to fulfil this need by conducting a systematic review and evaluation of the findings of primary/secondary and/or tertiary intervention studies for neck/upper extremity musculoskeletal conditions undertaken between 1999 and 2004.
METHODS
Search strategy
An initial search of the literature integrated a variety of sources including textbooks and conference proceedings, national and international health and safety organisation websites, and a general internet search. From this initial search, an extensive keyword list was developed to incorporate nationally and internationally recognised work-related musculoskeletal terms and definitions (eg, musculoskeletal disorder, repetitive strain injuries and occupational overuse syndrome), inclusive of diagnostic conditions (eg, thoracic outlet syndrome and cubital tunnel syndrome). Keywords specific to intervention studies were generated, which used a combination of generic labels (eg, musculoskeletal control and ergonomic intervention) and specific intervention approaches (eg, workstation design, job rotation and physical training).
Four researchers (BA, MGB, JC and MS), guided by a library and information manager, carried out the literature search. The keyword list and all combinations of keywords were used uniformly by all four researchers to ensure a standardised approach to the search procedure. An initial check of the keyword list was made against each of the subject headings from 15 electronic databases (CINAHL (including Cochrane Reviews); EBSCO Megafile Premier (including Medline, Health Source: Consumer Edition and Nursing/Academic Edition); Embase; Ergonomics Abstracts; Index NZ; AMED (Allied and Complementary Medicine); Annual reviews; Psych INFO (including PsycARTICLES); ProQuest 5000 (including ProQuest Health and Medical Complete); Expanded Academic ASAP; Sports Discus; Science Direct; Blackwell Synergy; Lippincott 100; OSH Reference Collection (including OSHLINE with NIOSHTIC and NIOSHTIC2)). An examination of review articles (unrestricted by date of publication), as well as the personal libraries of the contributing authors, was undertaken to identify further studies. Personal communications with national and international representatives or experts within the field of musculoskeletal conditions were also made. Where appropriate, additional keywords were added and modifications made to the keyword list.
The final search involved the previously mentioned 15 electronic databases and an examination of the bibliographies of recent review papers. To ensure that only high-quality papers were included within the current literature review, strict inclusion/exclusion criteria were adopted. These criteria were based on previous major reviews in this subject area (Bernard10).
Inclusion criteria
-
Published within the past 5 years (Jan 1999–Oct 2004).
-
Participation rate ⩾70%.
-
Health outcomes defined by symptoms and/or well-documented questionnaires and/or physical examination.
-
The body part in question was subjected to an independent exposure assessment—that is, direct observation or actual measurement of exposure.
-
Musculoskeletal conditions of the neck, shoulder, elbow and hand/wrist (neck/upper extremities).
-
Duration of subject follow-up ⩾2 months.
-
Sufficient documentation of intervention and intervention process.
-
English language publications.
Exclusion criteria
-
Back pain and lower extremity injuries.
-
Laboratory-based studies.
-
Clinical treatment of musculoskeletal disorders.
-
Clinically based modifier interventions such as pharmacological treatment, splinting, acupuncture and physiotherapy or chiropractic treatment.
Quality assessment and grading of studies
The critical appraisal and grading of studies involved the use of the generic appraisal tool for epidemiology (GATE): appraisal modules (effective practice, informatics and quality improvement).11 This tool focused specifically on issues of study validity, quality of the study, the measure of occurrence, effect and precision of the study results and external validity.
After completion of the GATE checklists for intervention studies, papers were graded according to the quality of the study using a modified version of the Cochrane Musculoskeletal Injuries Group scoring system, in conjunction with the GATE tool, to provide an overall score for each study.12 The modified Cochrane Musculoskeletal Injuries Group scoring system comprised 13 separate questions graded between 0 and 2, covering aspects of study design and outcome measures. A final overall score (quality rating), out of a possible 26, was awarded to each intervention paper. Once each study had been assigned a rating score, it was graded according to a three-point rating scale: low, medium or high. The cut-off points for each level of grading were based on the overall distribution of scores across the intervention studies: <10 = “low”-quality study; ⩾10<19 = “medium”-quality study; ⩾19 = “high”-quality study.
Six reviewers (BA, MGB, JC, PJL, PJM and MS) were trained in the review and scoring protocols. Two reviewers scored each paper independently, and if any discrepancy was found between their scores a third person reviewed the paper to reach a consensus.
Evidence classification
A “pattern of evidence” approach for classifying the level of evidence attached to intervention studies was adopted.1 The terminology and criteria used to define these levels of evidence were adapted from previous review papers6,7,10,13–15 and modified according to the quality assessment procedure adopted by this review (table 1). The overall level of evidence (ie, strong, moderate, some or insufficient) was then based on the number of studies, study design and the quality rating ascribed to that study.
Level of evidence for evaluating the importance of intervention studies in the management of neck/upper extremity musculoskeletal conditions
Classification of intervention studies
Using a format similar to Westgaard and Winkel,5 studies in this review were categorised into subgroups depending on the type of intervention: mechanical exposure interventions, production systems/organisational culture interventions and modifier interventions. Interventions were also classified as primary, secondary and/or tertiary according to the definitions of the National Research Council1—that is, primary interventions before members of the population at risk having acquired a condition of concern; secondary interventions after occurrence of the condition within the population of concern and tertiary intervention strategies designed for individuals with chronically disabling conditions.
RESULTS
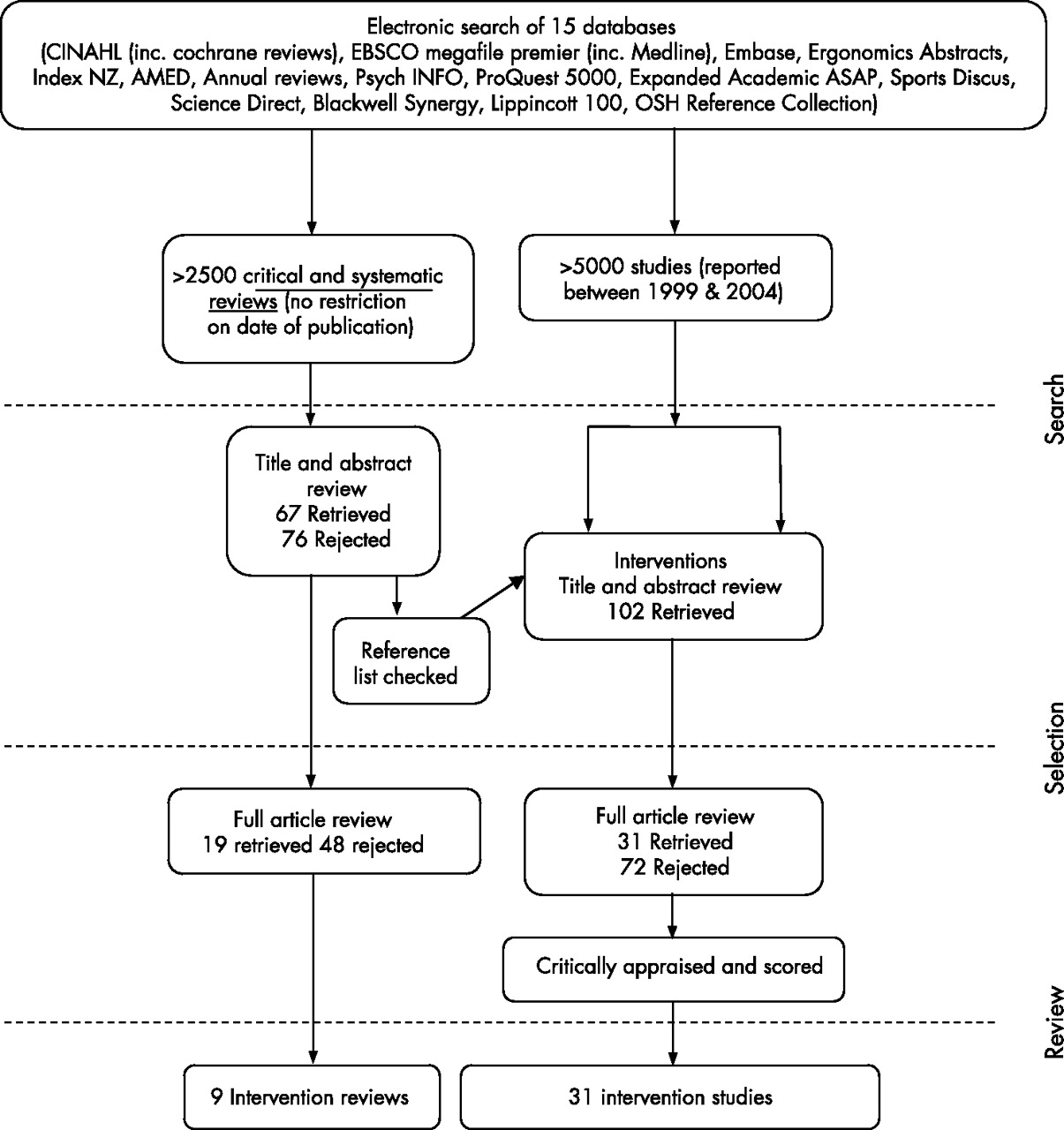
In excess of 5000 articles were identified from the initial search, of which 451 were suitable for abstract review; after a review of the abstracts, 102 intervention studies were considered. In total, 31 intervention studies were considered to have met the inclusion criteria and were suitable for full review (fig 1). Ten were classified as mechanical exposure interventions, two as production systems/organisational culture interventions and 19 as modifier interventions. On the basis of the type of mechanical intervention involved and the group of workers reported upon, it was possible to further classify mechanical interventions into three subgroups: (1) work environment/workstation adjustments and visual display unit (VDU) workers, (2) workstation equipment and VDU workers and (3) ergonomic equipment and manufacturing workers. Although no subgroups of production systems/organisational culture interventions could be identified, it was possible to group studies in the area of modifier interventions under six broad categories: (1) exercise and neck/upper extremity conditions; (2) exercise and fibromyalgia; (3) multiple modifier (including exercise) and neck/upper extremity conditions; (4) multiple modifier (including exercise) and fibromyalgia; (5) multiple modifier (excluding exercise) and neck/upper extremity conditions and (6) multiple modifier (excluding exercise) and fibromyalgia. Table 2 gives the tabulated information pertaining to each paper.
Summary of intervention studies
{kind=link}
Overview of the literature search and review strategy.
Mechanical exposure interventions
Ten studies were classified as mechanical exposure interventions, and thereafter subdivided into three main groups as described previously. Within the subgroup of work environment/workstation adjustments (eg, modified lighting, new work place, office layout and software application) in VDU workers with neck/upper extremity conditions, four studies16–19 presented positive outcomes. Three were of medium quality,16,17,19 and included an RCT,19 whereas one study18 was of low quality. On the basis of the levels of evidence identified in table 1, it was concluded that there was some evidence for positive health effects after work environment/workstation adjustments in VDU workers with neck/upper extremity conditions.
Three studies20–22 that involved changes to workstation equipment (ie, keyboards and mouse design) in VDU workers with neck/upper extremity conditions reported positive outcomes resulting from these types of interventions. Rempel et al’s21 and Tittiranonda et al’s22 studies were RCTs of high and medium quality, respectively, while Arras et al’s20 study was of low quality. Hence, there was moderate evidence to support this type of intervention.
Three studies23–25 that involved the introduction of ergonomic equipment (eg, adjustable chairs and vibration-proof tools) for workers with neck/upper extremity conditions used in the manufacturing industry found positive health outcomes. However, all were rated as low quality. Thus, it was concluded that there was insufficient evidence for positive health effects resulting from this type of intervention.
Production systems/organisational culture
Two studies26,27 did not find improvements in health outcomes associated with organisational and work-task design changes in office workers and manufacturing assembly workers; both studies were of low quality. Thus, there was insufficient evidence to support production systems/organisational intervention strategies.
Modifier interventions
Nineteen studies were classified under modifier interventions, and subsequently subclassified as described previously. Positive health outcomes were observed in three medium-quality studies28–30 that examined the effects of exercise (eg, strength training, coordination and flexibility) in workers with neck/upper extremity conditions (excluding fibromyalgia). These studies included an RCT.28 Thus, it was concluded that there was some evidence that exercise has positive effects in workers with neck/upper extremity conditions.
Of the four studies31–34 that investigated the effects of exercise (ie, aerobic, flexibility and biofeedback for relaxation) in patients diagnosed with fibromyalgia, one study32 was rated as high quality and three31,33,34 as medium quality. Schachter et al32 and van Santen34 found no significant differences across control and experimental groups. Meiworm et al31 and Valim et al33 noted positive findings after the intervention, although a control group was lacking in the latter study. Overall, it was concluded that there was some evidence in support of the use of exercise as an intervention for managing patients diagnosed with fibromyalgia.
One RCT of medium quality38 and three of low quality35–37 provided some evidence that multiple modifier interventions including exercise (ie, rest-breaks, Getsom programme, education and strengthening) can have positive effects in workers with neck/upper extremity conditions (excluding fibromyalgia). Furthermore, four medium-quality studies40–43 that included an RCT,41 and one low-quality study39, provided some evidence that multiple modifier interventions including exercise (ie, land and pool exercises, relaxation, education and cognitive behavioural therapy) can have positive effects in workers with fibromyalgia.
An RCT of medium quality,44 which examined multiple modifier interventions excluding exercise (ie, cognitive behavioural training and education), showed positive effects for workers with neck/upper extremity conditions (excluding fibromyalgia). By contrast, one low-quality study45 examining education found no significant effects. Therefore, there was some evidence to support the use of this strategy. With respect to multiple modifier interventions excluding exercise (ie, social support and education) for workers with fibromyalgia, there was insufficient evidence from an RCT in a medium-quality study46 to support this strategy.
DISCUSSION
This review embodied the principles of a systematic review. Although some authors have suggested that an important facet of a systematic review might be to include a meta-analysis,47 this was not considered appropriate for this review due to the heterogeneity of study designs, the general poor quality of studies and the diversity of exposure and outcome measures reported.
This review attempted to classify interventions according to whether they were primary, secondary or tertiary. Most studies were considered to involve secondary and/or tertiary interventions, although the type of intervention was often difficult to determine or not clearly stated, particularly for tertiary interventions (ie, studies often failed to define chronically disabling conditions). In most cases, tertiary interventions fell within the group of modifier interventions and, typically, involved subjects with fibromyalgia. Although some studies included both subjects with pain (ie, secondary intervention) and those without pain (ie, primary intervention), those without pain were rarely discussed independently within the results sections of the respective studies. These difficulties, combined with the heterogeneity of outcome measures, prevented direct comparisons between interventions or the evaluation of the efficacy of certain intervention types. Furthermore, where studies failed to make a clear distinction between subjects with and without pain, or to stratify their analysis according to the different participant groups, it is difficult to fully appreciate whether an intervention was benefiting one group of subjects more than another—for example, findings may well have been driven more by the prevention of new disorders than existing cases. The design of future studies should clearly define the purpose and population groups targeted, clearly documenting those participants who benefited most from the intervention.
To group intervention types and facilitate comparisons with previous reviews, the classification system proposed by Westgaard and Winkel5 was adopted. This classified interventions according to whether they were mechanical, production systems/organisation culture or modifier interventions. In some instances, further sub-grouping of interventions was possible, thereby enabling interventions to be more closely aligned to specific industries, population groups and/or musculoskeletal conditions.
Mechanical interventions
Table 3 provides an overall summary of the effectiveness of mechanical interventions based on the findings of the current review and makes comparisons with those of previous reviews. The finding that there was some evidence for work environment/workstation adjustment for improved health outcomes in VDU workers with neck/upper extremity conditions was consistent with two previous reviews5,48 and similar to that of Verhagen et al.9 With respect to the latter review, it should be noted that different levels for indicating evidence were adopted and, on examination, their level denoted as “limited” can be considered similar to our level “some”.
A comparison between the current and previous reviews for the level of evidence in support of mechanical interventions for neck/upper extremity musculoskeletal conditions
In this study, there was moderate evidence that workstation equipment (mouse and keyboard design) can lead to positive health benefits in VDU workers with neck/upper extremity musculoskeletal conditions. However, there was insufficient evidence for equipment interventions among manufacturing workers with neck/upper extremity musculoskeletal conditions. Previous reviews have not delineated according to types of occupation. With respect to the findings for VDU workers, Williams et al8 reported a trend towards positive benefits for several workplace interventions associated with modifications to keyboard designs, while our findings showed stronger support for this intervention strategy. This difference may reflect the more objective approach to grading evidence used in this review. In contrast to our conclusions related to VDU workers were those of Verhagen et al,9 who found limited evidence for the efficacy of some keyboards in people with carpal tunnel syndrome. However, it should be noted that Verhagen et al9 reported that the RCT study by Tittiranonda et al22 provided no evidence to support modifications to keyboard design, a finding in contrast with our appraisal of the paper and also that of Williams et al.8
Production systems interventions
The finding of insufficient evidence for the benefits of production systems/organisation culture interventions was consistent with one previous review.5 Westgaard and Winkel5 identified seven Swedish production systems intervention studies and concluded that “this group of papers provided little evidence to suggest that improved health can be achieved through redesign of the production systems”.
The two production systems/organisation culture interventions26,27 identified in this review were of low quality, showed no improvements in outcome measures and involved non-RCT. Although RCTs are considered the most powerful study design, ensuring randomisation and control within the workplace, particularly with respect to changes in production systems or the organisational culture within a company, is not always possible or ethical.1,49 This raises the question as to whether these types of interventions should be subjected to the same rigour as those used to evaluate the efficacy of mechanical or modifier interventions, and whether different criteria on which to base evidence classification should be adopted.
Modifier interventions
Table 4 provides an overall summary of the efficacy of modifier interventions based on the findings of the current review and also makes comparisons with the findings of previous reviews. Westgaard and Winkel5 concluded that modifier interventions involving the worker (eg, physical training) often achieve positive benefits. The current study concurred with these conclusions in that it found there was some evidence that exercise alone had positive effects in workers with neck/upper extremity musculoskeletal conditions. This finding was similar to Verhagen et al,9 but in contrast to Williams et al8 who found insufficient evidence for the effectiveness of exercise programmes when managing neck/upper extremity musculoskeletal conditions. With respect to Williams et al,8 only one paper with a low sample size and without a control group formed the basis of their conclusion. However, in this study, evidence was based on the findings from three medium-quality studies, one of which was an RCT. With regard to fibromyalgia, some evidence for exercise interventions was found, although it should be noted that contrasting findings led to this conclusion. No other reviews have focused upon the effects of exercise and fibromyalgia.
A comparison between the current and previous reviews for the level of evidence in support of modifier interventions for neck/upper extremity conditions
The current review found some evidence for multiple modifier interventions, inclusive and exclusive of exercise, in patients with neck/upper limb conditions. Such programmes included a combination of various types of low-intensity group exercise training, education, relaxation techniques and/or cognitive behavioural therapy. A review by Karjalainen et al7 focused upon multidisciplinary biopsychosocial rehabilitation studies and found insufficient evidence to support these programmes in the rehabilitation of adult patients with upper limb repetitive strain injuries. However, only two studies were reported upon in this review and these were published in 1994–5. Similarly, Verhagen et al9 concluded that there was a clear lack of evidence for multidisciplinary treatment. However, this conclusion was based on a single study, whereas the current review identified 12 studies examining multiple modifiers. Some evidence was found to support the use of multidisciplinary rehabilitation inclusive of exercise for fibromyalgia. Multiple modifier interventions exclusive of exercise were not effective in improving musculoskeletal health in patients with fibromyalgia, although there was an indication that some psychological factors, such as feelings of helplessness, may be improved. Similarly, Karjalainen et al14 considered the effects of multidisciplinary rehabilitation exclusive of exercise for fibromyalgia, reviewing seven studies of which four were of low quality, and concluded that there was insufficient evidence to support these programmes.
Limitations of the review
Although this review included those studies that used well-documented questionnaires for pain symptom outcomes, the validity and reliability of these measures could not always be determined. Unpublished studies, conference proceedings, reports and PhD theses were not reviewed. Reviewers were not blinded to authors or affiliations of published articles and, finally, the review was restricted to studies written in English.
CONCLUSION
This review identified no one single strategy for intervention that was considered effective for all types of industrial settings. The findings provided evidence to support the use of some mechanical and modifier interventions as approaches for the prevention and management of neck/upper extremity musculoskeletal conditions and fibromyalgia. With respect to the latter, there was a distinct lack of well-designed modifier intervention studies where the intervention was specifically tailored for the work environment and the tasks performed by the workers. Evidence to support the benefits of production systems/organisational culture interventions was lacking. These findings may be a reflection of the difficulty of undertaking studies within the workplace that include interventions focused upon health benefits compared with increased productivity and performance.
Overall, there seemed to be no clearly defined research strategy targeted at the identification of effective interventions specific to high-risk industrial workers or individual neck/upper extremity musculoskeletal conditions. At present, there are only isolated studies, often of low quality, that provide limited information for the establishment of new evidence-based guidelines applicable across a number of industrial sectors. Future consideration should be given to a national/international research strategy plan targeted at specific groups (industries) or neck/upper extremity musculoskeletal conditions. In this respect, a series of well-designed, related projects will improve our understanding of the complexity of issues related to injury and occupational health management. Until then, we will continue to be faced with isolated research projects, the findings of which do not provide sufficient evidence for changing existing injury prevention and management practices.
Main messages
-
An international systematic review of contemporary literature (within the past 5 years) found 31 ergonomic interventions for the prevention and management of neck/upper extremity musculoskeletal conditions
-
Findings support the use of some mechanical and modifier interventions for managing upper extremity conditions and fibromyalgia
-
Although evidence is lacking to support the benefits of production systems/organisational culture interventions, new quality criteria to replace that of blinding and randomisation may be necessary if the efficacy of these interventions is to be properly understood
-
Future consideration should be given to a national/international research strategy plan targeted at specific high-risk industry groups and/or neck/upper extremity conditions.
Policy implications
-
Until such evidence is available, interventions for the prevention and management of neck/upper extremity musculoskeletal conditions should continue to use multifactorial approaches
-
The use of production systems/organisational culture changes should not be viewed as a single specific intervention that will bring about improved outcomes in those workers with neck/upper extremity musculoskeletal conditions.
Answers (true (T), false (F)) to the questions on How to undertake a systematic review in an occupational setting by Nicholson, on pages 361–6
1. a) T; b) T; c) F; d) F; e) T.
2. a) F; b) F; c) T; d) T; e) F.
3. a) F; b) T; c) T; d) T; e) T.
4. a) T; b) F; c) T; d) T; e) F.
5. a) T; b) F; c) T; d) T; e) T.
Acknowledgments
The financial support of the Accident Compensation Corporation of New Zealand in funding this research project is greatly appreciated. We acknowledge the valuable assistance and guidance of AUT’s Information and Education Services, in particular Andrew South.
REFERENCES
Footnotes
-
Published Online First 14 September 2006
-
Competing interests: None declared.