Article Text

Abstract
Background Recently, the use of specific exercise programmes to prevent musculoskeletal injuries in team ball sports has gained considerable attention, and the results of large-scale, randomised controlled trials have supported their efficacy. To enhance the translation of these interventions into widespread use, research trials must be reported in a way that allows the players, staff and policymakers associated with sports teams to implement these interventions effectively. In particular, information is needed on core implementation components, which represent the essential and indispensable aspects of successful implementation.
Objectives To assess the extent to which team ball sport injury prevention trial reports have reported the core implementation components of the intervention, the intervention target and the use of any delivery agents (ie, staff or other personnel delivering the intervention). To summarise which specific types of intervention, intervention target and delivery agents are reported. To develop consensus between reviewers on the reporting of these components.
Methods Six electronic databases were systematically searched for English-language, peer-reviewed papers on injury prevention exercise programme (IPEP) trials in team ball sports. The reporting of all eligible trials was assessed by two independent reviewers. The reporting of the three core implementation components were coded as ‘yes’, ‘no’ or ‘unclear’. For cases coded as ‘yes’, the specific types of interventions, intervention targets and delivery agents were extracted and summarised.
Results The search strategy identified 52 eligible trials. The intervention and the intervention target were reported in all 52 trials. The reporting of 25 trials (48%) specified the use of delivery agents, the reporting of three trials (6%) specified not using delivery agents, and in the reporting of the remaining 24 trials (46%) the use of delivery agents was unclear. The reported intervention type was an IPEP alone in 43 trials (83%), education/instruction in how to deliver an IPEP in three trials (6%) and multiple types of interventions (including an IPEP) in six trials (12%). Players were the most commonly reported intervention target (88%, n=46), followed by multiple targets (8%, n=4) and coaches (4%, n=2). Of the 25 trials for which delivery agents were reported, 13 (52%) reported a single type of delivery agent and 12 (48%) multiple types. The types of delivery agents reported included coaches, physiotherapists, athletic trainers and team captains.
Conclusions The current reporting of core implementation components in team ball sport IPEP trials is inadequate. In many trial reports, it is unclear whether researchers delivered the IPEP directly to players themselves or engaged delivery agents (eg, coaches, physiotherapists, athletic trainers) to deliver the programme. When researchers do interact with delivery agents, the education/instruction of delivery agents should be acknowledged as an intervention component and the delivery agents as an intervention target. Detailed reporting of implementation components in team ball sport IPEP trials will facilitate the successful replication of these interventions by intended users in practice and by researchers in other studies.
Statistics from Altmetric.com
Introduction
Injuries in team ball sports (eg, soccer, basketball and volleyball) are common. In the European Union, team ball sports injuries account for 44% of all hospitalised sports injuries,1 and in the USA, the three sports resulting in the highest number of hospitalisations in young athletes are football, basketball and soccer.2 The high treatment costs and loss of sports participation associated with these injuries highlight the importance of injury prevention in this context.3 ,4
Recently, there has been considerable interest in strategies to prevent team ball sport injuries, and in particular the use of injury prevention exercise programmes (IPEPs) specifically designed to reduce musculoskeletal injuries.5–9 Examples of IPEPs are the ‘FIFA 11+’,6 the ‘PEP’ programme,10 ,11 ‘Knaekontroll’9 and ‘PAFIX’.12 These programmes generally consist of a combination of balance, plyometric, stability and sport-specific exercises targeting established lower limb injury risk factors.13 ,14 The results of recent published trials support the efficacy of team ball sport IPEPs.6 ,7 ,9 ,15 The FIFA 11+ reduced overall injuries by 32%, overuse injuries by 53% and severe injuries by 45% in female soccer players.6 The ‘Knaekontroll’ programme resulted in a 64% reduction in the rate of anterior cruciate ligament injury in female soccer players.9 A 68% reduction in the number of injured players was reported following implementation of the FIFA 11+ in male basketball players,15 and implementation of an IPEP in female handball players resulted in a 49% reduction in the risk of acute ankle and knee injuries.16
While establishing efficacy is an important step in building the evidence base for team ball sport IPEPs, it has been emphasised that efficacy alone is not enough.17–22 As articulated by Sogolow et al22:
For many years, injury prevention researchers have assumed that an intervention deemed efficacious in an experimental setting will easily (or often automatically) be translated to the field of practice. Unfortunately, this is not the case. (page 494)
Without high-quality implementation, no evidence-based intervention will fully achieve its intended effects in real life.17–27 In addition to information on what can be done to prevent injuries (eg, details of an efficacious IPEP's design), the players, staff and policymakers of sports teams need high-quality information on how it can be done in practice (eg, the staff, training and resources required to implement an IPEP with success). While there is a paucity of knowledge on which factors influence the successful implementation of sports injury interventions,19 ,28 in other research fields the most essential and indispensable aspects of programme implementation have been described.23–25 These aspects have been termed ‘core implementation components’ (also known as ‘implementation drivers’ or ‘core elements’) and include the selection, training and evaluation of the staff who deliver an intervention.22–24 ,29 Identifying and attending to core implementation components is seen as a key process in successfully translating interventions from research into practice.22 ,23 ,28 In the context of team ball sport, injury prevention core implementation components relate to the sports team staff (eg, coaches, physiotherapists, athletic trainers) who deliver the programme to players.
Unfortunately, the reporting of many sports injury prevention trials contains very little or no information on precisely who delivered the intervention and exactly how it was delivered.17 ,19 ,20 ,30 We recently reported the difficulties experienced when attempting to identify information on core implementation components from the reporting of five team ball sport IPEP trials.30 A detailed evaluation of implementation components, as outlined in the RE-AIM framework,31 was hindered by a lack of clear reporting of information relating to three basic components:
-
What is the intervention?
-
Who is the intervention target?
-
Who delivered the intervention and were they under researcher control?
A prerequisite to fully evaluating the reporting of core implementation components in team ball sport IPEP trials, and applying conceptual models such as the RE-AIM framework, is identifying and reaching consensus on these three basic components. Therefore, we conducted a systematic review of published trials on team ball sport IPEPs to assess the reporting of information related to these components. The specific aims were to
-
determine the extent to which IPEP trials reports have clearly reported the intervention, the intervention target and delivery agents;
-
summarise the types of intervention, intervention target and delivery agents reported in published trials;
-
to develop consensus between reviewers on the reporting of these components, as a precursor to applying the full RE-AIM framework to the reviewing of team ball sport IPEP trials.
The term delivery agents (also known as intervention agents) originates from the RE-AIM framework31 ,32 and refers to the staff who deliver an intervention to the intended beneficiaries. As shown in figure 1, one approach to delivering an IPEP is for researchers to directly deliver the IPEP to players themselves; in other words, it is the researchers who have direct engagement with the players (figure 1A). A more common approach, however, is for the researchers to directly engage with others (the delivery agents) who they would then like to deliver the IPEP to players (figure 1B). For example, researchers might educate coaches or other team staff about how to deliver an IPEP and then require the coaches to deliver this to their players.

Illustration of two different methods of delivering an injury prevention exercise programme (IPEP). (A) The research team delivers an IPEP directly to players. The research intervention is the IPEP, and the intervention target is the players. (B) The research team educates and instructs delivery agents (eg, coaches) in how to deliver an IPEP to players. The research intervention is the education/instruction, and the target of the research intervention is the coaches. The injury prevention intervention is the IPEP, and the target of the injury prevention intervention is the players.
Methods
Search strategy
The following electronic databases were systematically searched from their inception to 20 December 2012 by one of the authors (JO'B): PubMed, Medline, CINAHL, Embase, Scopus and the Cochrane Controlled Trials Register. Search terms were combined into the following search strings, representing key themes: (“Team sport” OR “Team sports” OR Soccer OR Football OR Rugby OR Gridiron OR Basketball OR Netball OR Hockey OR Handball OR Volleyball”) AND (Program* OR Exercise* OR Training) AND (Injur*) AND (Prevent*). Additional articles were sought by scanning the reference lists of retrieved articles and by contacting experts.
Eligibility criteria
All identified records were pooled and duplicates removed. The titles and abstracts of all records were screened for eligibility by one of the authors (JO'B). Papers were included if they were English-language, peer-reviewed, reported an IPEP in team ball sport players and included an outcome related to changes in injury incidence. In the context of this review, an IPEP was defined as a structured exercise programme specifically aimed at preventing musculoskeletal injuries. Review papers, abstracts and case studies were excluded. A full list of eligibility criteria is shown in the online supplementary appendix 1. Full-text versions of all remaining trial reports were obtained, and eligibility screening was repeated.
Quality appraisal
The reports of all eligible trials were assessed by two independent reviewers using a purposely designed data extraction sheet. One data extraction sheet was used for each unique trial; in cases where multiple papers reported results from the same trial they were considered together. The content of the data extraction sheet was based on our three previously identified components relating to essential information when reporting sports injury prevention interventions.17 The reporting of the intervention, the intervention target and delivery agents was coded as ‘yes’, ‘no’ or ‘unclear’. In cases coded as ‘yes’, reviewers also extracted information to answer the following questions in the data extraction sheet: “What is the intervention?”, “Who is the target?” and “Who are the delivery agents?”
The intervention was defined as the change in conditions trialled by the researchers. The intervention target was defined as the trial participants on whom the intervention was imposed. Delivery agents were defined as non-researchers who directly delivered the IPEP to players (eg, coaches). Two methods were used to calculate agreement between the two reviewers. The first method aimed to assess agreement on whether or not the intervention, the intervention target and delivery agents were reported, and only considered the coding of questions as ‘yes’, ‘no’ or ‘unclear’. For this method, the percentage agreement for each of the three questions was calculated as (the number of trials with matching codes/the total number of trials)×100. The second method aimed to assess the level of agreement on extraction of information about the reported type of intervention, intervention target and delivery agents, and considered both the coding and answers to the data extraction questions. For this method, the percentage agreement for each question was calculated as (the number of trials with matching codes and answers/the total number of trials)×100. Percentage agreement was considered the most appropriate measure of reliability as only two reviewers were involved, and the high prevalence of ‘yes’ codes was considered problematic for κ coefficients.
The two reviewers met to compare their results and reach agreement on the coding and answers of all eligible trials, through a process of discussion and mutual consensus. Trials were only coded as ‘yes’ or ‘no’ if the relevant information was explicitly reported. For example, trials were coded as ‘yes’ for the question relating to delivery agents if the use of multiple, non-researcher agents (eg, team staff) to deliver the programme to players was explicitly reported. Similarly, trials were coded ‘no’ if it was clearly reported that delivery agents were not involved (eg, trials in which researchers delivered an IPEP directly to players). All other trials were coded as ‘unclear’. After consensus, the percentage of trials coded as ‘yes’, ‘no’ and ‘unclear’ for each question was calculated. From the consensus answers, the percentage of trials reporting each different type of intervention, intervention target and delivery agent was calculated.
Results
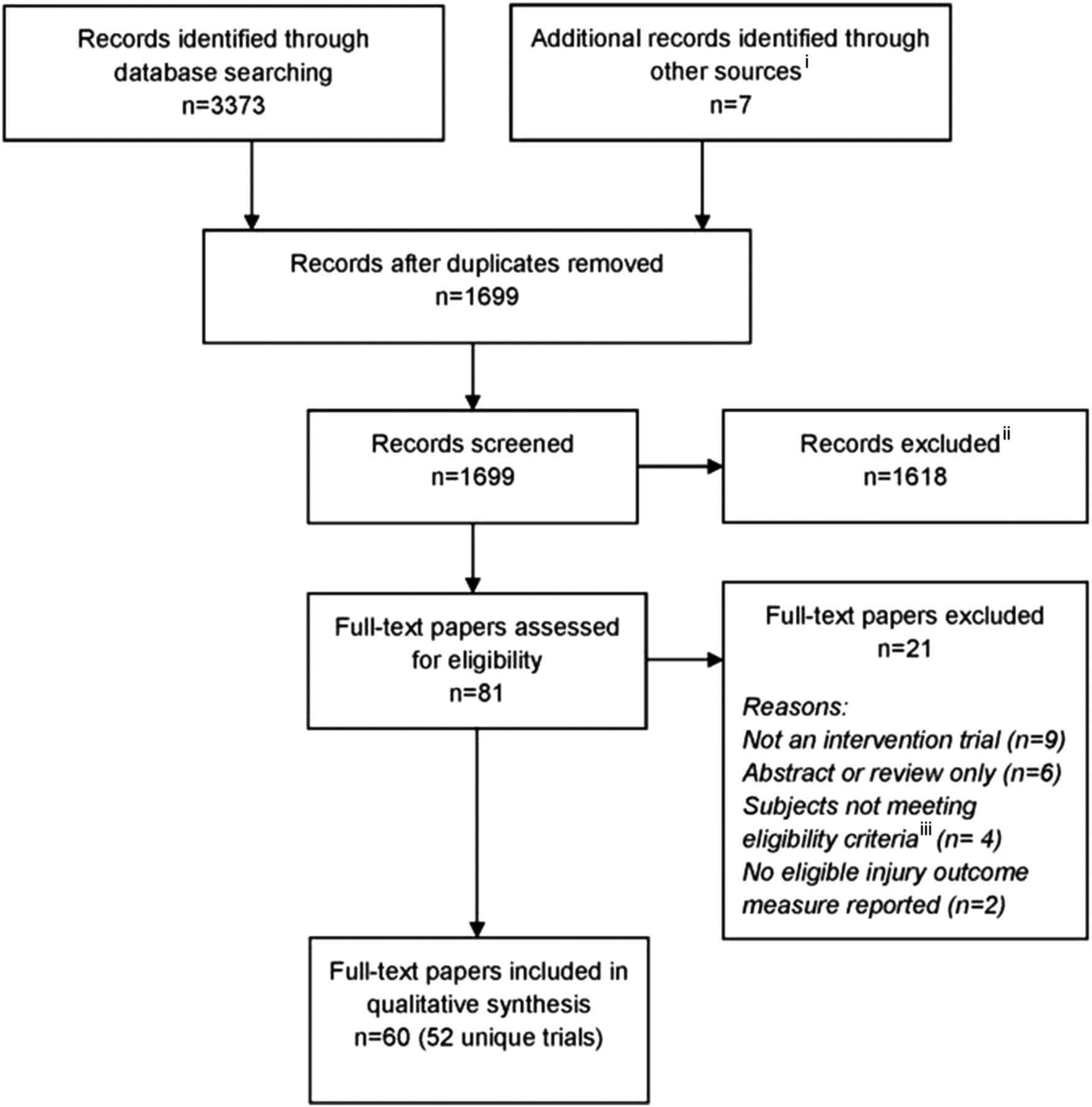
The systematic search identified a total of 60 eligible papers, covering 52 unique intervention trials (figure 2). As multiple papers covering the same trial were considered together, the following results are presented in terms of the 52 trials.

Search strategy used to identify team-based injury prevention exercise programme (IPEP) trials. iSeven additional records were identified in the reference lists of retrieved articles. iiThe most common reasons for excluding records were (1) they were not intervention trials; (2) they did not investigate musculoskeletal injuries and (3) they did not include an injury outcome. iiiFour studies were excluded due to the subjects having existing injuries or not being team ball sports players.
The independent-review level of agreement when only considering the codes ‘yes’/‘no’/‘unclear’ was 100% for reporting of the intervention, 98% for reporting of the intervention target and 58% for the reporting of delivery agents. The level of agreement when also considering the reviewers’ extraction of information in relation to “What is the intervention?”, “Who is the target?” and “Who are the delivery agents?” was 79% for the intervention, 77% for the intervention target and 58% for delivery agents.
The consensus codes and extracted information agreed upon by the two reviewers are summarised below, and readers are referred to the online supplementary appendices 2 and 3 for a full listing of consensus codes and the reported interventions, intervention targets and delivery agents.
The reporting of the intervention and intervention target were coded as ‘yes’ for all 52 trials. For the reporting of delivery agents, 25 (48%) trials were coded as ‘yes’, 3 (6%) as ‘no’ and 24 (46%) as ‘unclear’.
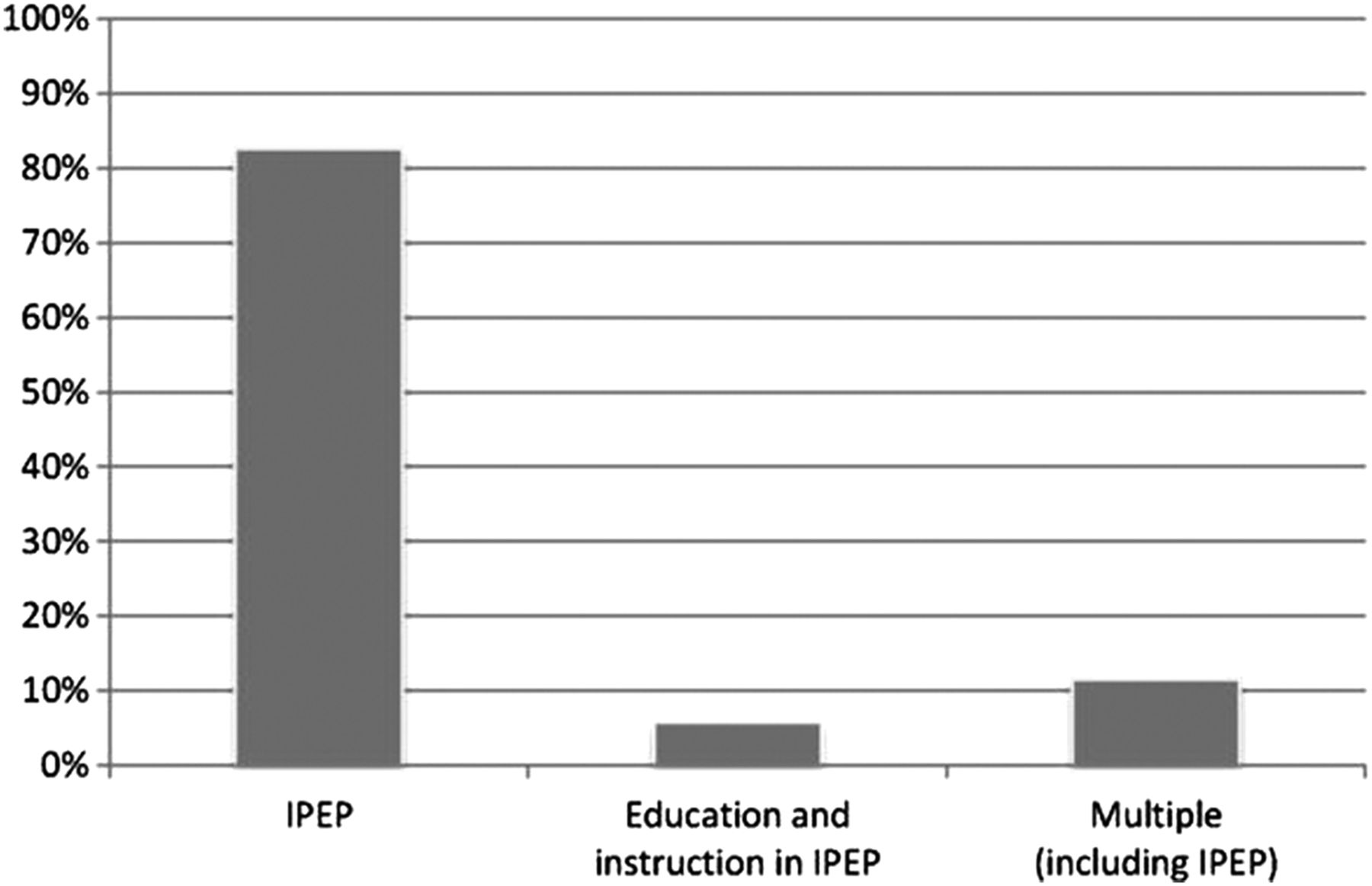
The types of reported research intervention and the proportion of trials for which each type was reported are summarised in figure 3. An IPEP was reported in all trials (as per eligibility criteria), and for 43 (83%) of the trials the IPEP was reported as the sole intervention. For three trials (6%), the education and instruction of coaches3 ,33 or coaches and team captains6 in how to deliver an IPEP was reported as the research intervention. For six trials (12%), multiple interventions (including an IPEP) were reported. The other types of interventions in these trials included the education and instruction of coaches, team staff, players or parents,34–36 ankle orthoses37 ,38 and a seven-part prophylactic programme.39

Percentage of team ball sport injury prevention exercise programme trials (n=52) reporting each type of intervention.
The types of intervention target and the proportion of trials for which each type was reported are shown in figure 4. Players were the reported target of the interventions in 46 (88%) of the included trials. In the reporting of two (4%) trials, coaches were the intervention target, while in four (8%) trials multiple targets, including coaches, team staff, parents and players, were reported.
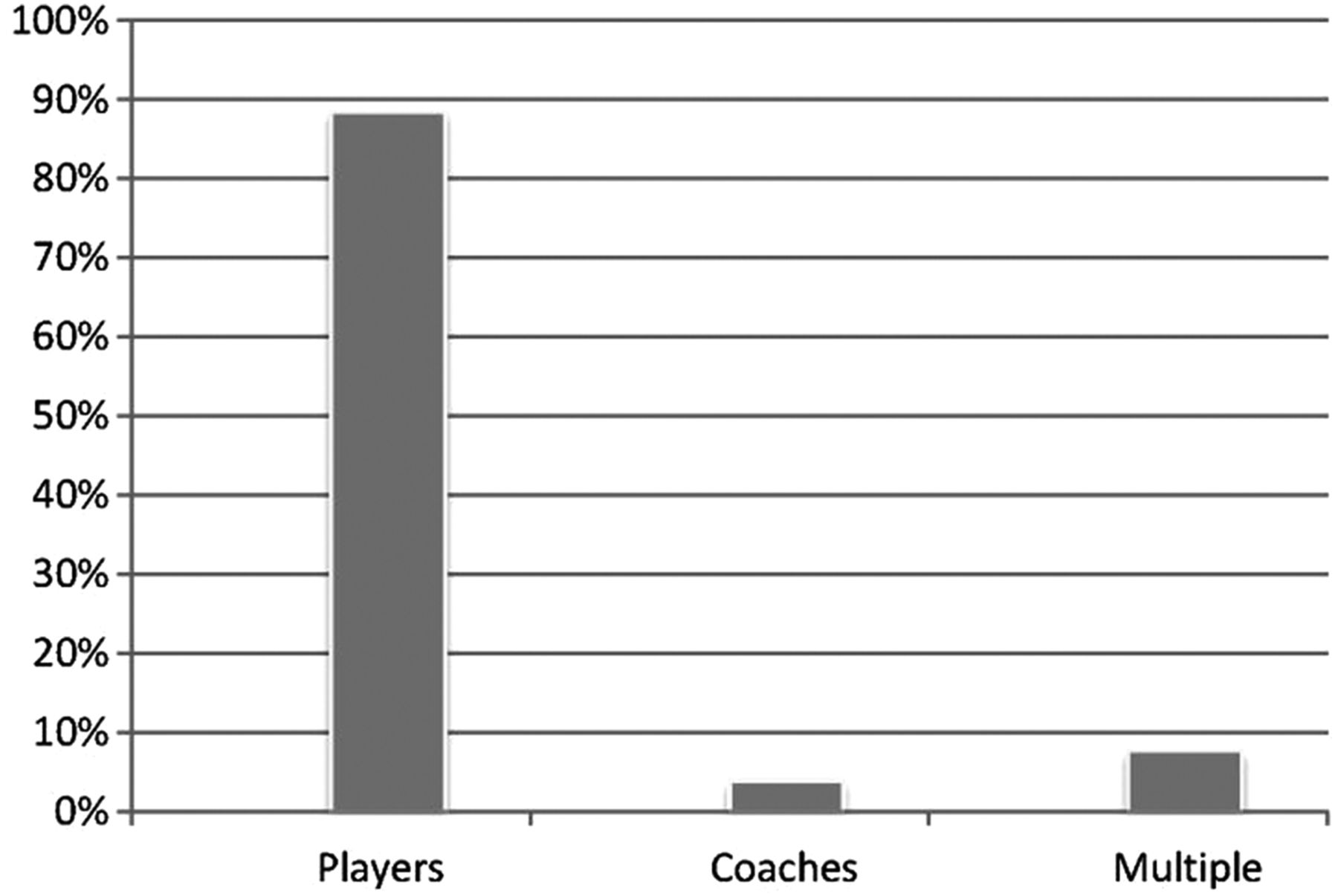
Percentage of team ball sport injury prevention exercise programme trials (n=52) reporting each type of intervention target.
Of the 25 trials with clear reporting of delivery agents, the types of delivery agents and proportion of trials for which each type was reported are shown in figure 5. A combination of delivery agent types (including coaches, physiotherapists, team captains and athletic trainers) was reported for 12 (48%) of the included trials. In the reporting of 10 (40%) trials, the delivery agents were all coaches, and in three (12%) trials, they were all physiotherapists.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Percentage of team ball sport trials (n=25) reporting each type of delivery agent.
Despite the presence of delivery agents being reported in 25 trials, only four (16%) of these identified the delivery agents as an intervention target, and the education and instruction of these delivery agents as an intervention.
Discussion
This is the first systematic review to evaluate the extent to which interventions, intervention targets and delivery agents are reported in team ball sport IPEP trials. Accurate identification of these three components is a prerequisite to more extensive evaluation of implementation components.30 In many of the trial reports included in this review, it was unclear whether researchers delivered the IPEP directly to players or engaged delivery agents (eg, coaches, physiotherapists, athletic trainers) to deliver the programme. Clear reporting of precisely how IPEPs were delivered in their intervention trials is necessary to facilitate the replication of these programmes by intended users in practice and by researchers in other studies.
The need to bridge the gap between research and practice and focus more research efforts on the successful implementation and dissemination of evidence-based interventions has been emphasised in many areas of health promotion.17–29 40–42 A key process in enhancing implementation is identifying core implementation components as the indispensable aspects of an implementation programme.23 The authors of intervention trials can potentially contribute valuable information regarding core implementation components, but often these aspects are not sufficiently reported.17 ,30 ,42–45 This review demonstrates the current poor level of reporting implementation components in team ball sport IPEP trials.
Although all the trials in this review were coded as ‘yes’ for reporting an intervention and intervention target, in many cases it was difficult to ascertain whether the intervention was the IPEP, education/instruction in the IPEP, or both. Similar difficulty was encountered in labelling the intervention target as the players, the delivery agents, or both. From a reporting perspective, it is worrying that the use of delivery agents was unclear in 46% of the included trials. The rare examples where detailed information on delivery agents was provided illustrate the potential value of this information for future implementation efforts. For example, Soligard et al7 reported an 87% higher probability of an IPEP having low compliance if the coach believed the programme was too time consuming. Similarly, if the coach believed the programme lacked football-specific activities, the probability of low compliance with the IPEP was 81% higher. Another study on the effects of an IPEP in high school team ball sports reported over 60% of eligible coaches not enrolling, primarily due to lack of time or interest in collecting data on injuries and athletic exposure.33
Many team ball sport injury prevention trials use team coaches, physiotherapists or other delivery agents to deliver IPEPs to players. Most IPEPs are intended to be integrated in the team training warm-up, and the successful adoption, implementation and maintenance of the IPEP will largely be determined by the coaches or other team staff members who deliver the warm-up. While the players are the intended health beneficiaries of IPEPs, a prerequisite to players fully benefiting from the programme is the successful engagement of delivery agents. Educating delivery agents about the IPEP, instructing them in how to deliver it, providing support and evaluating their delivery are all key components for achieving the desired outcome.
This systematic review represents an important initial step towards a better understanding of core implementation components in team ball sport IPEPs. In addition to illustrating deficits in the current reporting of IPEP trials, we believe the process of reaching consensus between reviewers on the intervention, intervention target and delivery agents will allow us to overcome our previous difficulties in applying the RE-AIM framework to this specific context.30 While no such review has been conducted in the field of sports injury prevention, application of the RE-AIM framework as a reviewing tool in other fields of health promotion has identified important knowledge gaps and potential directions for future research.46–48
The key challenge in reaching consensus between the reviewers was ascertaining (from the available reporting) who actually delivered the IPEP to the players: the members of the research team or non-researcher delivery agents such as team coaches or physiotherapists. In many trial reports, details of the IPEP design (eg, individual exercises and dose) were reported in detail, but information on how the IPEP was delivered, and by whom, was either scarce or completely absent. In some cases, it was reported that physiotherapists or athletic trainers delivered the IPEP, but it was not clearly reported whether these individuals were sporting team or research team members. In other cases, while it was reported that coaches were educated about the IPEP, whether the coaches actually delivered the programme was not stated. The lack of clear reporting made it difficult to judge which delivery method (as depicted in figure 1) had been employed by the researchers, and accordingly whether the research intervention should be labelled as an IPEP, education/instruction in a IPEP, or both, and the intervention target as players, delivery agents, or both.
Limitations
The data extraction tool used in this systematic review has not been previously validated or subjected to reliability testing. The authors are aware that other studies meeting the eligibility criteria may have been published since completion of the search strategy. The use of more than two independent reviewers may have strengthened the methodology of this review. As the use of κ coefficients was judged inappropriate, the results for reviewer agreement may have been influenced by chance agreement. This review focussed on the use of IPEPs designed to reduce musculoskeletal injuries: the inclusion of injury prevention strategies designed to reduce other types of injuries (eg, spinal cord injury, concussion) may have yielded different results. Despite the importance of the reporting issues covered in this review, the ultimate effectiveness of any injury prevention intervention will only be as strong as the difference in injury incidence and severity before and after its intervention.49
Conclusion
The current reporting of core implementation components in team ball sport IPEP trials is inadequate. In many trial reports, it is unclear whether researchers delivered the IPEP directly to players or engaged delivery agents (eg, coaches, physiotherapists, athletic trainers) to deliver the programme. When researchers do interact with delivery agents, the education/instruction of delivery agents should be acknowledged as an intervention and the delivery agents as an intervention target. Detailed reporting of implementation components in team ball sport IPEP trials will allow intended users to successfully replicate these programmes in practice.
What is already known on the subject
-
Recent research supports the efficacy of injury prevention exercise programmes (IPEPs) in team ball sports.
-
To enhance the reproducibility of IPEPs in practice, information is needed on how they were implemented in their evaluation trials.
-
Core implementation components represent the most crucial and indispensable aspects of an implementation programme.
What this study adds
-
The current level of reporting of delivery agents in team ball sport injury prevention exercise programme trials is inadequate.
-
For almost half (46%) of the 52 included trials, it was unclear whether or not delivery agents were used.
-
In many cases, the key interaction between researchers and delivery agents was not reflected in the reporting of the intervention and intervention target.
Acknowledgments
This work was led by JO'B as part of his PhD studies, supervised by CFF. The Australian Centre for Research into Injury in Sport and its Prevention (ACRISP) is one of the International Research Centres for Prevention of Injury and Protection of Athlete Health supported by the International Olympic Committee (IOC).
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Files in this Data Supplement:
- Data supplement 1 - Online supplement
Footnotes
-
Contributors JO'B designed the study, led its conduct, performed the systematic search and had a major role in writing the paper. CFF independently reviewed the eligible full-text papers, participated in the consensus discussions and contributed to the writing of the paper.
-
Funding JO'B was supported by a University of Ballarat Postgraduate Scholarship. CFF was supported by NHMRC Principal Research Fellowships (ID: 565900 and 1058737).
-
Provenance and peer review Not commissioned; externally peer reviewed.