Article Text

Abstract
Objective This paper analyses costs and potential lives saved from a door-to-door smoke alarm distribution programme using data from a programme run by the Baltimore City Fire Department in 2010–2011.
Design We evaluate the impact of a standard home visit programme and an enhanced home visit programme that includes having community health workers provide advance notice, promote the programme, and accompany fire department personnel on the day of the home visit, compared with each other and with an option of not having a home visit programme (control).
Results Study data show that the home visit programme increased by 10% the number of homes that went from having no working alarm to having any working alarm, and the enhanced programme added an additional 1% to the number of homes protected. We use published reports on the relative risk of death in homes with and without a working smoke alarm to show that the standard programme would save an additional 0.24 lives per 10 000 homes over 10 years, compared with control areas and the enhanced home visit programme saved an additional 0.07 lives compared with the standard programme. The incremental cost of each life saved for the standard programme compared with control was $28 252 per death averted and $284 501per additional death averted for the enhanced compared with the standard.
Conclusions Following the US guidelines for the value of a life, both programmes are cost effective, however, the standard programme may offer a better value in terms of dollars per death averted. The study also highlights the need for better data on the benefits of current smoke alarm recommendations and their impact on injury, death and property damage.
Statistics from Altmetric.com
Introduction
Annually, an estimated 378 600 fires in US residences result in 2850 deaths.1 Smoke alarms reduce the risk of death in residential fires by roughly a half.1 Despite an estimated 96% of US households observed to have at least one smoke alarm, only four-fifths of homes have smoke alarms working at any given time.1
Past studies found that households with a smoke alarm directly installed (by firefighters or community volunteers, for example) were more likely to have that smoke alarm still working 6 months later.2 The Centers for Disease Control sponsored Smoke Alarm Installation and Fire Safety Education programme recommends installation of long-life lithium battery smoke alarms for low income families.3 Such programmes can be costly and labour intensive; therefore it is essential to determine if they are cost-effective in preventing deaths from fires. Parmer et al (2006) conducted a cost analysis of smoke alarm installation programmes in multiple states across the USA and found that, as expected with economies of scale, the more smoke alarms installed, the less the cost of each smoke alarm,4 Haddix et al conducted one of the few cost effectiveness analyses of a programme in Oklahoma in 1990 in which teams (including members of the local fire department, health department and others) conducted door-to-door distribution of smoke alarms along with education about fire safety and maintenance.5 Haddix et al estimated that over 5 years the programme saved $1.5 million in medical costs and over $14 million in productivity losses, and reduced deaths and injury. The programme analysed by Haddix et al is similar to the Baltimore programme examined in this paper, in that it involved door-to-door distribution of smoke alarms using fire department personnel and included educational materials. Other cost-effective analyses of smoke alarm distribution programmes have been less conclusive. Ginnelly et al (2005) did a cost-effectiveness analysis of a randomised control trial of smoke alarm distribution in the UK and found that the programme was not cost-effective.6 They included a wide range of costs, including property damage, healthcare utilisation, police and fire department time and resources, etc. The main problems with the programme, the authors argue, were that not enough alarms were installed, and those that were installed were not maintained over time.
Because safety experts want to spend their resources wisely, it would be useful to update estimates of the cost-effectiveness of smoke alarm distribution measures to reflect recent changes. The existence of a mature smoke alarm distribution programme in Baltimore, MD provides us with an opportunity to revise and update estimates of the cost-effectiveness of smoke alarm distribution in a modern urban setting.
Baltimore, Maryland, has one of the highest poverty and crime rates in the USA, and a large number of vacant houses, which are at increased risk for fires.7 Baltimore has an estimated 2866 residential fires per year (in a population with 214 787 dwellings).8 In 1992 the Baltimore City Fire Department (BCFD) began to routinely deploy fire department personnel to visit homes door-to-door. In this standard home visit programme, the teams of firefighters park their fire truck in the neighbourhood (enabling them to be ‘on call’ to respond to fires while still doing the home visits), and knock on all the doors in the selected area. When residents let them in, the firefighters obtain consent, and inspect premises for the adequacy of smoke alarms. Personnel install up to four smoke alarms per home and provide fire safety education. Beginning in 2010, the smoke alarms were long-life lithium battery powered.
In 2010–2011 the BCFD partnered with Johns Hopkins Center for Injury Research and Policy to conduct a quasi-experimental trial to compare the results of the city's standard approach to smoke alarm distribution with an enhanced home visit programme designed to increase the number of homes the fire personnel gained access to and thereby the number of alarms they installed. This enhanced programme maintained all the elements described above for the standard programme but added having community health workers (CHWs) provide advance notice to the community about upcoming home visits.9 The CHWs, trained by the Center for Community Health at the Urban Health Institute, Johns Hopkins University, went door to door 4 days or 5 days before a home visit event, encouraging residents to be home for the event and delivering a scripted promotional message. The CHWs also promoted smoke alarm awareness and provided education to communities through posting lawn signs and posters around the neighbourhood. The main focus of these activities was to raise awareness about the programme, encouraging people to accept new smoke alarms and increase the trust of residents so they would open their doors to the fire department team. On the morning of the event, CHWs would again knock on all doors, reminding those who were at home to wait for the fire department's visit.
This paper performs a cost-effectiveness analysis of the standard and enhanced programmes using the programmatic data collected in the trial. The standard programme is compared with a hypothetical no programme control area, and then the marginal additional benefit of the enhanced programme is compared with the standard programme. The aim was to understand the cost per life saved of the standard and enhanced programmes. This analysis adopts an approach similar to that of Miller and Levy (1997) and follows their guidelines for how to estimate cost effectiveness for injury prevention programmes.10 The analysis takes a societal perspective, but since there is only weak evidence to support cost savings from prevented injury, disability and property damage, these elements of the societal perspective are zero and the social cost of the smoke alarm programme is weighed against the benefit of deaths averted and averted potential life years lost. Our analysis is of a specific programme in Baltimore City, however, it may be applicable to other poorer urban settings that are considering using fire department resources to increase smoke alarm distribution.
Methods
We used the Baltimore data to model the impact of the standard and enhanced programmes and a control in three hypothetical populations of 10 000 dwellings each. For the model, we assumed that the probability of a fire was independent of the existence of a smoke alarm. We could not find evidence that smoke alarm installation would prevent fires from occurring. There are mixed reports on whether smoke alarms prevent property damage. The national data show some evidence that property damage values are paradoxically higher in homes that have smoke alarms.11 Over the period from 2005 to 2009, the average cost per home fire with no smoke alarm was $18 411 compared with an average of $19 385 if a smoke alarm was present (Table A. Page 18).11 This may be due to socioeconomic confounding of smoke alarm ownership with higher socioeconomic status, however keeping socioeconomic status (SES) somewhat comparable by confining the analysis just to apartment fires the paradox remains—property damage in apartment fires with no smoke alarm averaged $11 314 compared with $11 460 in fires in apartments with smoke alarms (Table 11 p.56).11 Similarly with early warning, residents might be able to reduce the frequency and severity of non-lethal fire injuries, but we could find no evidence to support this. Averaged from 2005 to 2009 there were 29.8 injuries (as defined by the National Fire Incident Reporting System) per 1000 fires in residences with smoke alarms compared with 36.3 similarly defined injuries per 1000 fires in residences with no smoke alarms.11 There has been concern that with the early warning provided by smoke alarms homeowners may find more early fires, undertake more do-it-yourself firefighting for small fires and sustain more non-lethal injuries than they would in the absence of an early warning.12 Lacking evidential support that smoke alarms prevent non-lethal injuries and property damage we are forced to take a conservative approach and ignore any potential beneficial impact of smoke alarms on lowering property damage or non-lethal injury.
The benefits of smoke alarms to lower death rates have only been estimated on the basis of having any working smoke alarms in the dwelling. It is reasonable to hypothesise that having working smoke alarms on every level of a multistory dwelling is more protective than having only one working smoke alarm, and although this is the recommended best practice, we could find no literature that measures the added benefit of this best practice. The Baltimore intervention achieved improvements in rates of having any working smoke alarm and improvements in having working smoke alarms on every level of a dwelling, but lacking any literature to show the additional benefit of reaching the every level standard, our cost-effectiveness analysis will be conducted based on achievements in converting homes without any working smoke alarms to homes having at least one working smoke alarm. There may be readers whose experience convinces them of the existence of the omitted benefits (avoided property damage, avoided injuries and extra benefits from long-life battery operated smoke alarms on every level of the household), and we would caution them that our estimates do not include these benefits. This is a conservative approach and keeps the analysis on an evidence-based footing. In the baseline model, we base our estimates of benefit solely on the proven link of having any working smoke alarm to lower death rates compared with having no working smoke alarm.
The estimates on the probability of fire and death by smoke alarm status are based on post-fire investigations that classify homes as with and without any smoke alarms. After a fire has occurred it is difficult for investigators to know with certainty how many smoke alarms there were or whether they were maintained and whether they were on every level of the home. Investigators are able to say whether any smoke alarm was present and whether it was reported to have operated.
Our benefit calculation assumed a 10 year horizon of benefit from smoke alarm distribution. We assumed that the processes of alarm battery decline and battery replacement underlying baseline prevalence rates of working smoke alarms were in equilibrium. Thus, in an untreated population with an 86% prevalence in 2012, smoke alarm prevalence would remain at 86% in 2022. Based on recent surveillance data from Baltimore, we saw no reason to project an upward or downward secular trend of smoke alarm prevalence in the untreated population. We assumed a constant number of smoke alarms each year. Past literature has found evidence of early alarm failure with lithium batteries,13 therefore, this programme used tamper-resistant alarms and added a stronger educational component. Nevertheless if early failure occurred it would lower the benefits.
On average 2866 residential fires occur annually in Baltimore; with a population of 214 787 residential dwellings, the probability of having a fire per year per residential dwelling is 1.33%.8 The base number of dwellings in each group (ie, 10 000) was multiplied by the probability of having a fire for each year. Tables 1 and 2 contain the data from the Baltimore Program and existing literature (respectively) that were used in the models. See online supplementary appendix 1 for a detailed description of the models. In the hypothetical control group no new smoke alarms would be received.
Parameters from the study9
Parameters from the literature used
Based on existing literature, the death rate is 11.8 deaths per 1000 home structure fires with no working smoke alarm and 5.2 per 1000 home structure fires with a working smoke alarm.14
In summary, we assume smoke alarm prevalence, home vacancy, pass door rates and distribution efficiency as was found by Gielen et al in 2012.9 We assume that the untreated and treated arms maintain that same baseline smoke alarm prevalence over 10 years. We assume the benefits from working smoke alarm as per Ahrens, 2011.1 We assume the only benefits are in deaths averted, and there are no benefits from property loss prevention or injury prevention. Finally, we assume that the smoke alarm distribution can be done by on-duty firefighters at no additional salary cost.
This study received IRB approval from Johns Hopkins Bloomberg School of Public Health.
Costs
The programme cost data are based on how many days it took a team to handle a list of dwellings that included vacant and non-vacant properties. Determination that a dwelling is vacant does take time during field visits, so the proper denominator includes all dwellings regardless of occupancy.
Personnel costs included cost of BCFD firefighters, and CHWs for the enhanced smoke alarm distribution programme. Because firefighters did the smoke-alarm distribution programme while they were on duty and available to respond to fire calls, their labour time did not have an opportunity cost. Had they not been conducting the smoke alarm distribution programme, they would have been simply back at the station waiting for fires just like firefighters in cities that do not have outreach programmes. Therefore, the only personnel cost is for the CHWs in the enhanced programme, who were paid on an hourly basis.
All households who received a fire alarm were assumed to have received a $10 alarm that lasted for 10 years. A 20% overhead was added to take costs of other fire department personnel (such a supervisors and support staff), gasoline, rent and any other costs into account. Since we assume that homes are treated and costs were expended in the first year, we did not need to account for ongoing costs over the 10-year time frame. As discussed above there is inconclusive evidence for differences in injury rates between homes with and without smoke alarms. Consequently, no medical costs or quality of life calculations (for survivors living with injuries) were taken into account as these effects and costs would be the same between groups. Costs due to property damage were not included in this analysis, as discussed above.
To calculate the discounted life years lost, we subtracted the average age of those who died in fires from the life expectancy for someone at that age. We discounted that life expectancy at 3% per year and used that value as the discounted life years lost.
Results
Smoke alarms, fires and deaths
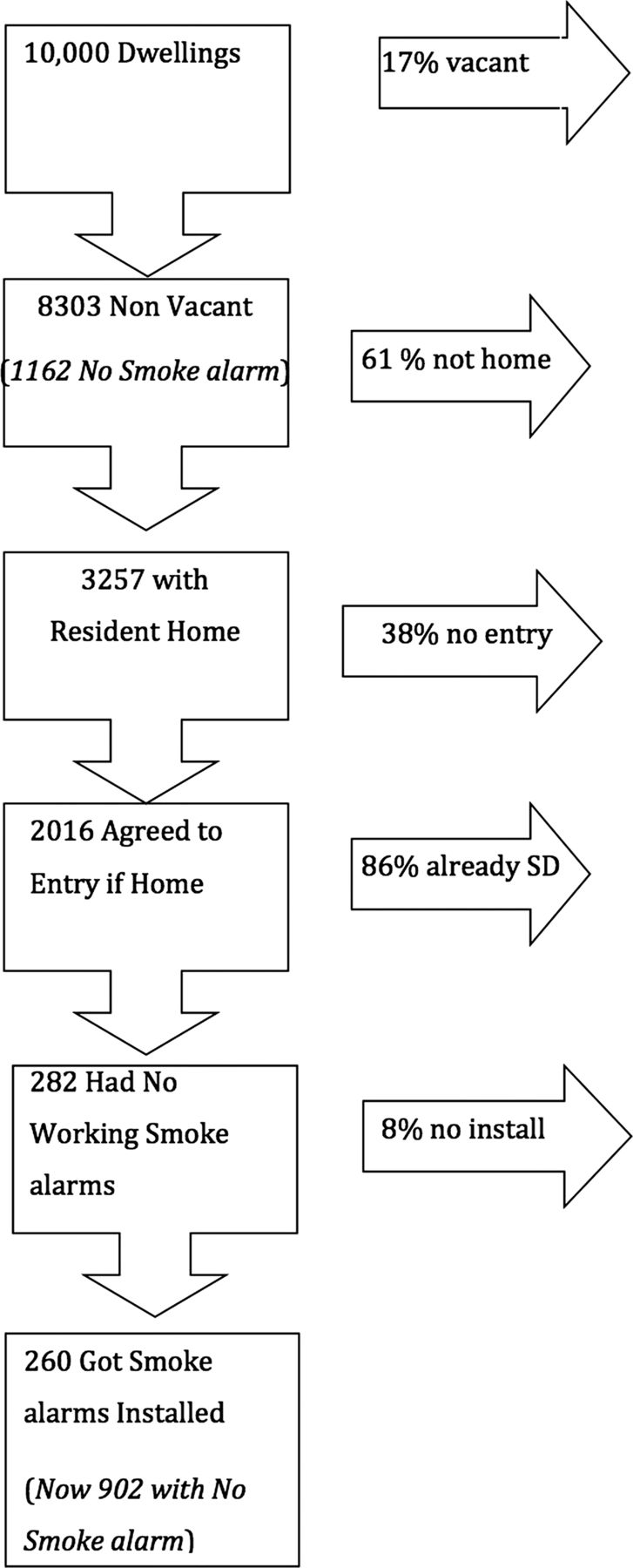
A flow diagram of levels of participation, and smoke alarm distribution is shown in figures 1 and 2. Given vacancy rates in the study area, 1702 homes would be vacant for every 10 000 houses.9 As can be seen in the flow diagram, given rates of entry in the study, if study personnel visited 10 000 homes, they would find someone at home who agreed to be in the study in 3257 homes in the smoke alarm distribution programme and 3353 homes in the enhanced smoke alarm distribution programme groups. Eliminating the 86% of homes that already had at least one working smoke alarm, this would lead to 260 and 331 new smoke alarms being installed for the smoke alarm distribution programme and enhanced smoke alarm distribution programme, respectively for every 10 000 homes visited, conservatively assuming at least one smoke alarm installed per home. We assumed that the homes that were not visited would have the same rates of currently working smoke alarms as the population as a whole. Summing the number of working smoke alarms already in the population with those added by the programme, the standard group would have an estimated 7401 dwellings and the enhanced group would have an estimated 7472 dwellings with at least one working smoke alarm in an at-risk population of 8303 non-vacant homes in a set of 10 000 dwellings that needed to be treated. The untreated population would have 7141 dwellings with at least one working smoke alarm. Based on the increased probability of successfully entering a home during the home visit programme, the respective probabilities of having at least one working smoke alarm per non-vacant dwelling would be 86% in the untreated population, 89% in the standard programme population, and 90% in the enhanced programme population.

Flow chart for enhanced programme.

{kind=link}
{kind=link}
Flow chart for standard programme.
From these rates of homes with and without at least one working smoke alarm, we calculated the number of fires in each treatment group over a 10-year period. All treatment groups would have the same hypothetical number of fires since there is no difference in the rate of fires between homes with and without smoke alarms (1334 per 10 000 per year).9
Guidelines for cost=effectiveness analysis suggest discounting lives at 3% a year.10 As can be seen in table 3, the control group would be estimated to have a total of 8.17 undiscounted (7.18 discounted at 3%) deaths per 10 000 households over 10 years. The smoke alarm distribution programme group would have a total of 7.90 undiscounted deaths (6.93 discounted at 3%) over 10 years per 10 000 homes. Finally, the enhanced sweep group would have a total of 7.82 deaths (6.87 discounted at 3%) per 10 000 homes over a 10-year period. The respective estimates are 0.24 lives saved by the smoke alarm distribution programme and an additional 0.31 lives saved over that time period by the enhanced group compared with the no treatment group (0.07 more than the smoke alarm distribution programme over 10 years). This comes to 5.21 life years saved between the control and sweeps, and an additional 1.42 life years saved between the enhanced and sweeps.
Absolute numbers of fires and deaths in 10 000 households comparing houses with and without smoke alarms in the three groups, over 10 years
The average age at death in fire deaths in Baltimore from 2008 to 2010 is 45 years.15 According to the most recent National Vital Statistics Report (published in 2012), the average life expectancy at age 45 years in the USA is 35.5 years.16 Using a discount rate of 0.3%, this gives us a discounted life years lost of 21.5 years.
Costs
The smoke alarm distribution programme would cost a total of $6845 with all costs occurring in the first year, including the costs of overhead, and the enhanced sweep would cost $25 700 (table 4).
Costs in the intervention year per 10 000 homes
The incremental cost of each additional life saved comparing the smoke alarm distribution programme with the control group is estimated at $1314 per life year saved.i The cost per life saved is calculated by dividing the cost of the programme by the number of lives saved. The incremental cost effectiveness ratio (ICER) is calculated by dividing the difference in the cost between two programmes by the difference in number of lives saved between those two programmes. It is the cost per additional life saved. The incremental cost for the enhanced programme, compared with the standard programme, was $13 232 per additional life year saved (table 5).
Incremental cost-effectiveness ratio (ICER)
Sensitivity analyses
Five different sensitivity analyses were conducted to take into account the fact that there are ranges of parameters found in the published literature for these indicators, and we chose conservative estimates for our baseline model. We first tested the sensitivity of the model to changes in the conditional probability of death if there is no smoke alarm in the house. Increasing the conditional probability of death by 20% for people in residential fires with no smoke alarms increased the number of deaths by 4% in the smoke alarm distribution programme and enhanced smoke alarm distribution programme populations. Decreasing the risk of residential fires in general by 20% decreased the number of lives saved by 16% in the smoke alarm distribution programme and enhanced smoke alarm distribution programme populations. Increasing the proportion of houses entered in the enhanced smoke alarm distribution programme population by 20% relative to regular smoke alarm distribution programme increased the number of lives saved in enhanced smoke alarm distribution programme by about 1% (table 6).
Fire and deaths in sensitivity analysis
Finally, we looked at the impact of increasing the overhead by 5% on the cost of the programme. Since this was an estimated value to take into account a number of additional costs, it was important to test the effect of this value being higher or lower. If the overhead were 5% more (25% of all costs), the overall ICER would be 4% more, and decreasing the overhead by 5% (to 15% of all costs) decreased the ICER by about 4% (table 7). All in all, small changes to the assumptions made in our model would not dramatically alter the overall estimates of the cost effectiveness of the standard and enhanced programmes relative to the control condition and relative to each other. Although we do not formally model this scenario, it is possible that the 10 year lithium batteries do not last 10 years.13 The smoke alarm distribution education by fire-fighters and health educators in this programme stressed the importance of regularly testing the batteries of smoke alarms and replacing batteries if needed, but long-term follow-up is not available. Assuming failed batteries are not replaced, any reduction in battery life would linearly reduce the number of lives saved, that is, if batteries only last 5 years and are not replaced, half as many lives would be saved.
ICERs for sensitivity analysis of cost assumptions
Discussion
Under very conservative assumptions in which survival gains accrue only from increasing the rate of having any working smoke alarm we find that the smoke alarm distribution programme and the enhanced smoke alarm distribution programme were cost-effective with incremental costs of $1314 and $13 232 per life year saved, respectively. Applying the smoke alarm distribution programme to 50 000 dwellings in 2010 would be estimated to save approximately one life over the subsequent 10 years. The high rate of cost effectiveness occurs because of the efficiency of using onduty firefighters’ time to conduct the programme. Because the firefighters are simultaneously distributing smoke alarms in their precinct while they are on call for firefighting duty, the programme makes effective use of the city's labour resources. It should be noted that should a programme not have the opportunity to use firefighters’ surplus time, and therefore have to pay individuals to go door-to-door, then costs would be much higher.
The smoke alarm distribution programmes in 2010 in East Baltimore encountered a population where 86% had any working smoke alarm and roughly 40% had a working smoke alarm on every level of the dwelling. For dwellings occupied by residents who answered the door, the rate of smoke alarm installation was quite high and 78% of these dwellings obtained a working smoke alarm on every level of the dwelling. However the majority (75–80%) of dwellings in East Baltimore were either vacant, not home, or refused to participate and overall we estimate that the programme increased the population average rate of have any working smoke alarm from 86% to 89% in the smoke alarm distribution programme and to 90% in the enhanced smoke alarm distribution programme. We estimate that the programme increased the population average of having a working smoke alarm on every level from 40% to 53% in the smoke alarm distribution programme and to 57% in the enhanced smoke alarm distribution programme.
The study is limited by the absence in the literature of a reliable way to estimate the additional benefit achieved by raising the proportion of households with a smoke alarm on every level. Although having any smoke alarm is known to cut the death rate in half in a fire compared with no smoke alarm,1 it is unknown how much having a smoke alarm on every level of the house lowers the death rate beyond just having any working smoke alarm. The degree of benefit would depend on the number of multilevel homes and the nature and timing of the fire risk in each home (eg, furnace-related, kitchen-related, smoking, etc). An extensive review of the literature also found inconclusive evidence that smoke alarms lowered the amount of property damage or lowered the rates of fire injury so these potential benefits were not included as potential offsets to the cost of the programme. We are also limited in that we only have data on risk of fire for all of Baltimore City, and risks of fire and of death from a fire could have been higher in the low-income area in which the intervention took place. Therefore, we could be underestimating the impact of the programme.
Most of the households entered received a long-life battery operated smoke alarm on every level of their home, consistent with the overall goal of the programme to ensure that best practice recommendations are implemented in all homes. As mentioned previously, the only available evidence on mortality risk reduction compares no working smoke alarm to any working smoke alarm, which is how we are calculating the cost-effectiveness model. However, all of the costs of multiple additional smoke alarms are included as operating costs because it would not be acceptable to only install a single smoke alarm when best practice requires a working alarm on every level. Again, this makes for a conservative estimate of the cost effectiveness of the programme under study.
The small size of the benefits—one life over 10 years among 50 000 dwellings—makes our estimates sensitive to the parameters used and sensitivity analysis showed that the estimated benefits are linearly related to the parameters. If fire death rates, programme coverage rates or smoke alarm efficacy rates change by 10% then the benefits change by roughly the same percentage.
The CHWs in the enhanced smoke alarm distribution programme also provided many educational messages about health and safety, but our model of benefits based on proven effects of smoke alarms is unable to assess how many lives were saved by these health messages. Another limitation in our analysis is that we assumed that the prevalence of smoke alarms would remain constant over the 10 years after they were installed. It is possible that residential mobility, landlord turnover and intentionally disabled smoke alarms could depreciate the smoke alarm prevalence rate among households accepting a new smoke alarm; therefore we might be overestimating the number of lives saved over time. However, preliminary data from the Baltimore study show that 90% of the alarms that were installed remained in place 6 months later.
We do not include the potential savings of lost productivity from the lives saved. It would be straightforward to invoke an estimated lost productivity of $764 000 per life saved as was done by Haddix (2001) as an offset to programme costs and state that from a societal perspective the smoke alarm distribution programme saves money and lives.5
The enhanced distribution programme, despite its extra personnel and awareness raising, only added an additional 71 homes with any working smoke alarm compared with the regular smoke alarm distribution programme. Consequently, the additional funds spent to improve the participation rate of households, although cost-effective, are not as cost-effective as doing ordinary smoke alarm distribution using onduty firefighters. The cost per death averted for upgrading from the no distribution to the standard smoke alarm distribution programme was $28 252, and an additional $284 501 to upgrade to the enhanced programme. If we follow US government estimates that the value of a statistical life is $5 million, then the smoke alarm distribution programme and the enhanced smoke alarm distribution programme are cost-effective, but regular smoke alarm distribution with using duty firefighters offers a better value in terms of dollars per life saved.17
Compared with the prior estimates from Oklahoma City in 1990 smoke alarm distribution programmes in Baltimore in 2010 are less cost-effective primarily due to a much higher prevalence of owning at least one smoke alarm (34% in Oklahoma City target area vs 86% in Baltimore City study area).5 The Oklahoma City population received an extensive educational campaign and also experienced improvements in factors other than just the prevalence of smoke alarms. The incidence of fires in the Oklahoma City target area went down by 23.66% and the rate of non-fatal fire related injuries went down by 77.14%. Our more conservative assumptions based on the literature on the impact of smoke alarms do not include changes in the rate of fires or non-fatal injuries.
Ceiling effects are typical of programmes that attempt to scale up health behaviours that are already relatively prevalent in a population. The experience in Baltimore also highlighted a growing obstacle to programmes based on home visitation in modern cities. Many people are not home even when visited multiple times and when they are home they are often unwilling to open the door. Past programmes in the UK have struggled with similar issues of refusal to participate.18 Although we found that the CHWs in the enhanced programme decreased refusal rates among families who were at home, their prepromotion of the programme did not increase the likelihood of residents being at home.8 However, despite ceiling effects and low rates of penetration, this study demonstrates that the standard and enhanced programmes are cost-effective and add smoke alarms to the homes in Baltimore, which will save lives.
Conclusions
Extrapolating our results to the entire population of 214 787 residences in Baltimore, the basic smoke alarm distribution programme could save, on average 4.5 lives over a 10-year period compared with no programme at all. In a population that would have, on average, somewhere around 200 deaths in that time period, this represents roughly 2% of fire deaths being averted. The cost at $1312 averted per life year lost over 10 years is substantially below US government's estimate that the value of a statistical life is $5 million. Smoke alarm distribution campaigns remain a cost-effective option to save lives despite ceiling effects provided that the personnel distributing the smoke alarms consist of onduty firefighters or other labour sources that have zero costs.
What is already known on this subject
-
Smoke alarms save lives in fires, and a large proportion of homes in the USA already have smoke alarms.
-
Analyses of programmes that distribute smoke alarms to homes have shown mixed results about their cost effectiveness.
What this study adds
-
This study updates the literature on the cost effectiveness of a smoke alarm distribution programme in an urban setting, comparing a basic programme with firefighters distributing smoke alarms to no programme and to a more involved programme that included community outreach.
-
Following the US guidelines on the cost of a life, the basic programme analysed and the more involved programme (with community outreach) were cost-effective; however, the standard programme had more impact in terms of lives saved per dollar spent.
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Files in this Data Supplement:
- Data supplement 1 - Online appendix
Footnotes
-
Contributors ND-S: Conducted data analysis, literature review and wrote the paper. DB: Responsible for the overall content as guarantor; advised on analysis and helped with writing the paper. EP: Planning, conduct, and reporting of the intervention and data collection, also advised on analysis, write-up, and read all drafts. WS: Planning, conduct, and reporting of the intervention and data collection, also advised on analysis, write-up, and read all drafts. AG: Planning, conduct, and reporting of the intervention and data collection, also advised on analysis, write-up, and read all drafts.
-
Funding Funding for this research was provided to the Johns Hopkins Center for Injury Research and Policy by: Centers for Disease Control and Prevention (1R18CE001339): Dissemination of Research in Child Safety; and NIH/National Institute for Child Health and Human Development (1R01 H059216): Community Partnerships for Child Safety.
-
Competing interests None.
-
Ethics approval Johns Hopkins School of Public Health.
-
Provenance and peer review Not commissioned; externally peer reviewed.
-
Data sharing statement For access to data, please contact the corresponding author.
-
↵i By ‘incremental’ we mean the additional cost comparing one program with another.