Article Text

Abstract
Objective: To evaluate whether home safety education and safety equipment provision increases thermal injury prevention practices or reduces thermal injury rates and whether the effect of interventions differs by social group.
Methods: Systematic review and meta-analysis using individual participant data (IPD) evaluating home safety education with or without provision of free or discounted safety equipment provided to children or young people aged 0–19 years. Main outcome measures: possession of functional smoke alarm, fitted fireguard and fire extinguisher; keeping hot drinks or food and keeping matches or lighters out of reach; having a safe hot water temperature and rate of medically attended thermal injuries.
Results: Home safety interventions were effective in increasing the proportion of families with a functional smoke alarm (odds ratio (OR) 1.83, 95% CI 1.22 to 2.74) and with a safe hot tap water temperature (OR 1.35, 95% CI 1.01 to 1.80). There was some evidence they increased possession of fitted fireguards (OR 1.39, 95% CI 1.00 to 1.94), but there was a lack of evidence that interventions reduced medically attended thermal injury rates (incident rate ratio (IRR) 1.12, 95% CI 0.81 to 1.56). There was no consistent evidence that the effectiveness of interventions varied by social group.
Conclusions: Home safety education, especially with the provision of safety equipment, is effective in increasing some thermal injury prevention practices, but there is insufficient evidence to show whether this also reduces injury rates.
Statistics from Altmetric.com
Burns are a serious global public health problem.1 Worldwide more than 73 000 children die each year from burn related injuries, many injuries occurring in the home or while at play.2 Further deaths occur as a result of scalds, electricity and chemical burns. Children who survive severe burns can have considerable levels of trauma and disability. Their lives may be further complicated by the stigma and discrimination related to their disability and disfigurement.1
The burden of thermal injury varies across geographical location, age group, gender and social group.3 At least 95% of fire related burns occur in low or middle income countries, where they represent the sixth leading cause of death in children aged 5–14.3 Within countries there are steep social gradients in childhood thermal injury deaths. In the UK, the death rate for fires was 37.7 times higher in children from long term unemployed families than in children from families in higher managerial or professional occupations.4 A similar picture emerges for hospital admissions, with children living in most deprived areas being 3.5 times more likely to be admitted with a burn or scald injury than children living in least deprived areas.5 Similar relationships have been reported from other countries.67
Several approaches have been tried to reduce the incidence of thermal injuries or increase safety practices, including parental education programmes,89 community programmes10 and provision of free or discounted safety equipment.1112 In some cases legislation has been used to reduce the risk, in particular with regard to reducing hot tap water temperature in the home.13 Two recent meta-analyses have examined the effects of interventions to increase smoke alarm ownership, promote a safe hot water temperature and childproof the home.1415 The first found a significant effect of interventions delivered during child health surveillance on smoke alarm ownership but not alarm functionality.14 The second found that interventions delivered in a clinical setting were effective in promoting a safe hot tap water temperature and in increasing smoke alarm ownership.15 However, despite social inequalities in thermal injuries and concern that educational interventions may not address inequalities in childhood injury or may even widen existing inequalities,16–18 little is known about whether interventions to prevent thermal injuries vary in their effectiveness by social group,17 or about their effect on thermal injury rates.
We have therefore undertaken a systematic review and meta-analysis using individual participant data (IPD) where available to evaluate whether home safety education and the provision of safety equipment increased thermal injury prevention practices or reduced thermal injury rates. We also examined whether the effect of these interventions differed by social group.
METHODS
This paper reports selected findings from meta-analyses of thermal prevention practices and thermal injuries which comprise part of a larger Cochrane systematic review of home safety education and safety equipment for the prevention of all injuries in childhood. Readers are referred to the full report published by the Cochrane Library for findings of studies not included in these meta-analyses.19
Searching
A range of data sources were searched as shown in table 1 (available online). Bibliographic databases were searched from the date of inception to June 2004. We also contacted authors of included studies, and in the UK we surveyed Sure Start and Home Start schemes, Fire and Rescue Services, the Royal Society for the Prevention of Accidents, the National Children’s Homes charity and the Community Practitioners and Health Visitors Association to identify unpublished evaluations of local home safety interventions. No language restrictions were used. The search strategy is described in detail elsewhere.19
Selection and study characteristics
We included randomised controlled trials (RCTs), non-RCTs (eg, quasi-randomised controlled trials) and controlled before and after (CBA) studies, with participants aged 0–19 years, which provided home safety education (with or without free, low cost or discounted safety equipment) and reported medically attended thermal injuries or thermal injury prevention practices.
Home safety education could be provided by health or social care professionals, school teachers, lay workers or voluntary or other organisations, to (individual or groups of) children or families. Eligible settings included health care settings (eg, primary care practices, clinics, outpatient departments, emergency departments and hospital wards), schools and family homes. Interventions providing free, low cost or discounted safety equipment were included. Multi-faceted community interventions were only eligible for inclusion if they included individual or group education on home safety.
The specific thermal injury prevention practices selected as outcomes for analysis were: possession of a functional smoke alarm, possession of a fitted fireguard (a guard placed around the fireplace to prevent the child falling onto or touching an open, gas or electric fire), possession of a fire extinguisher, having a safe hot tap water temperature, keeping matches and lighters out of reach of children and keeping hot drinks or food out of reach of children. Thermal injury rates were also included as an outcome.
Validity assessment
Quality was assessed independently by two researchers, blind to author, institution and study results. Blinding of outcome assessment and follow-up of at least 80% of participants per arm were used as quality markers for all study designs, and allocation concealment was used for RCTs. For non-RCTs assessment of distribution of baseline sociodemographic or economic characteristics, prevention practices and injury rates was used, with arms considered to be “balanced” where there was less than 10% difference between the prevalence at baseline. Any disagreements between researchers on study quality were resolved by referral to a third researcher.
Data abstraction
Two researchers independently assessed titles and abstracts for inclusion, with disagreements being resolved by referral to a third researcher. To maximise information available for analyses, we contacted authors of included studies to obtain individual participant data. Where IPD was unavailable, data were extracted from articles, using standard extraction forms independently by two researchers, blind to author and institution. Data extraction was compared between researchers for the first 53 studies covering all home safety and injury outcomes (ie, not just those studies reporting thermal injury prevention outcomes), and as a high level of agreement was found (see results section) one researcher extracted data for the remaining studies.
Quantitative data synthesis
Meta-analyses were undertaken where three or more studies reported the same outcome. Pooled odds ratios (OR) were estimated from summary binary data using a random effects model, or where there were fewer than five studies without significant heterogeneity between studies we used a fixed effect model. Where zeros were present in the 2×2 table for any study, 0.5 was added to each cell before meta-analysis. For rate outcomes, study specific effect sizes and standard errors were estimated from summary data using Poisson regression and entered into the meta-analysis. Where studies had used a cluster design but such clustering had not been accounted for in the analysis, we adjusted outcomes by dividing the number of participants with and without an outcome by the design effect, and the number of events and person-years by the variance inflation factor. Intra-class correlation coefficients (ICC) and coefficients of variation were calculated from IPD20 or obtained from published data. Where coefficients of variation were unavailable we used a value of 0.25.21 These analyses were undertaken using Stata V.8.
We used meta-regression to examine the effect of interventions by child age, gender, ethnic group, family type (single or two parent family) and parental unemployment (as an indicator of deprivation). The effect of binary covariates was assessed using IPD and study summary level data simultaneously, using a novel statistical model we developed.22 The effect of age was assessed using only IPD. These analyses were undertaken using WinBUGS V.1.4.1.
Cases with missing values were excluded from all analyses. Heterogeneity was assessed by χ2 tests and the I2 statistic, and explored by meta-regression as described above and by a priori specified subgroup analyses (the provision of safety equipment, follow-up period, setting, study design and study quality). Where meta-analyses included seven or more studies, publication bias was assessed using funnel plots and Egger’s test. Sensitivity analyses assessed the robustness of the findings with respect to the individual contribution of each study and the size of the ICC for clustered studies.
RESULTS
Study selection and study characteristics
Figure 1 shows the process of study identification and selection. Twenty-four studies were included in at least one of the meta-analyses,810–1223–42 10 of which provided IPD.8111223–26282938Table 2 (available online) shows the characteristics of included studies. Seventeen (71%) studies were RCTs, three (13%) were non-RCTs and four (17%) were CBAs. Thirteen studies came from the USA, six from the UK, and one each from France, New Zealand, Mexico, Norway and Greece.
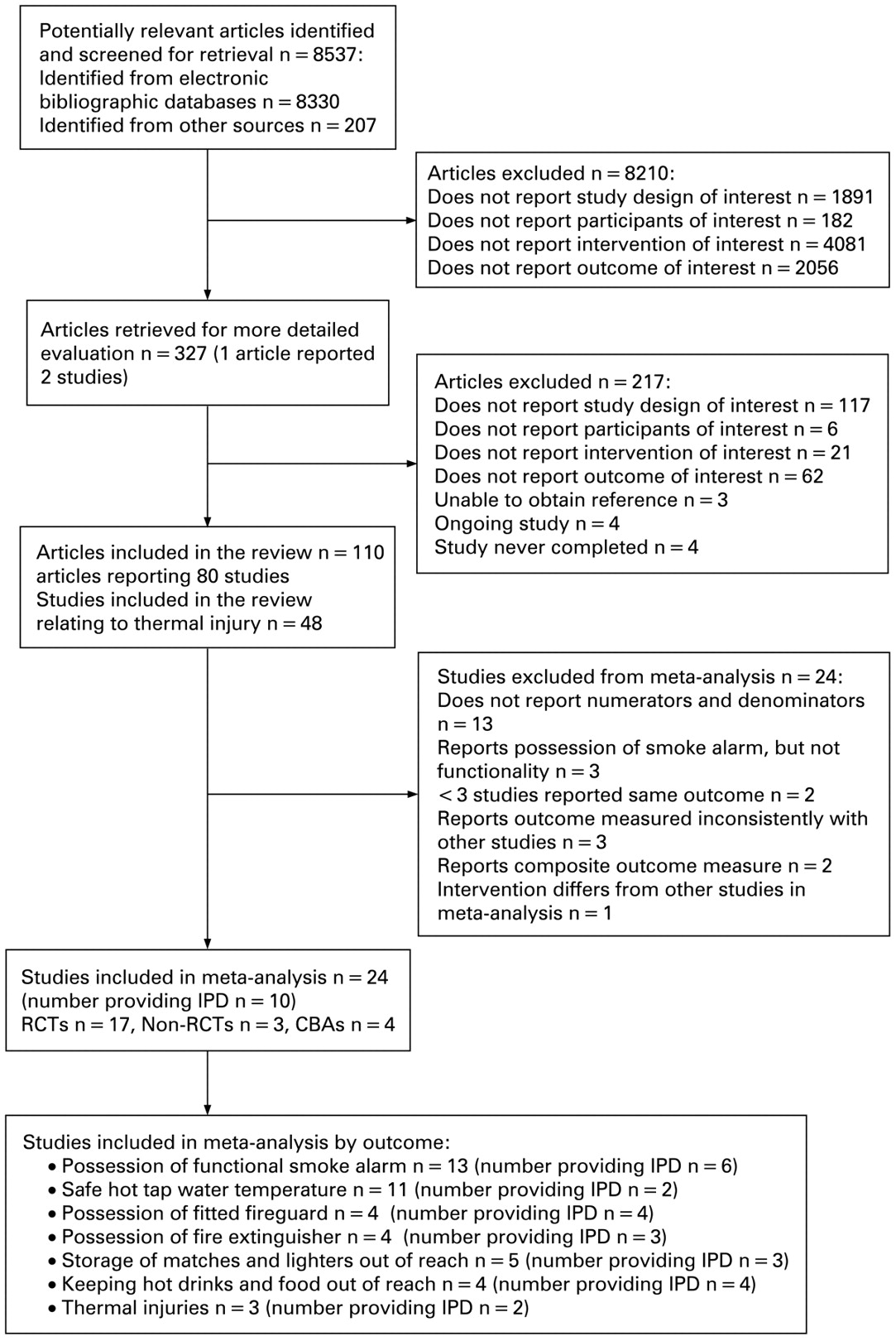
Flow chart detailing process of study selection.
In 14 (58%) studies the intervention provided free or subsidised equipment to prevent thermal injury or information on accessing subsidised equipment.810–1225262831333437–40 One study providing a home safety inspection and information on preventing thermal injuries also provided discount coupons for safety equipment, but it is unclear whether this included equipment to prevent thermal injury.30 One study referred parents to a child safety centre which offered a range of discounted safety equipment, including smoke alarms.27 Thirteen (54%) studies provided the intervention mainly in a clinical setting.81123252933–384041 In terms of outcomes, 13 studies (54%) reported possession of a functional smoke alarm,8111226–2830313438–41 four (17%) reported fitted fireguards,8112338 four (17%) reported fire extinguishers,24262830 11 (46%) reported having a safe hot tap water temperature,1027293032–3638 five (21%) reported keeping matches and lighters out of reach of children,2628303638 four (17%) reported keeping hot drinks or food out of reach of children,25282938 and three (13%) reported rates of medically attended thermal injuries.113842 The definition of a safe hot tap temperature varied between studies from <49°C to <60°C, and was unspecified in two studies.3435
Allocation concealment was adequate in eight (47%) of the RCTs,8111223–2629 four (17%) studies had blinded assessment of outcomes,12253036 in 13 (54%) studies all outcomes were assessed on more than 80% of participants,823242628–3237394042 and in a further two (8%) studies injury outcomes were assessed on more than 80% of participants but prevention practices were not.1138 In three (43%) of the seven non-randomised studies, confounding factors appeared to be balanced between treatment arms at baseline.243840
Reliability of data extraction
In the comparison of data extraction between the two researchers, 1386/1424 (97.3%) items extracted for the first 53 studies covering all home safety and injury outcomes were identical.
Quantitative data synthesis
Effect of home safety interventions
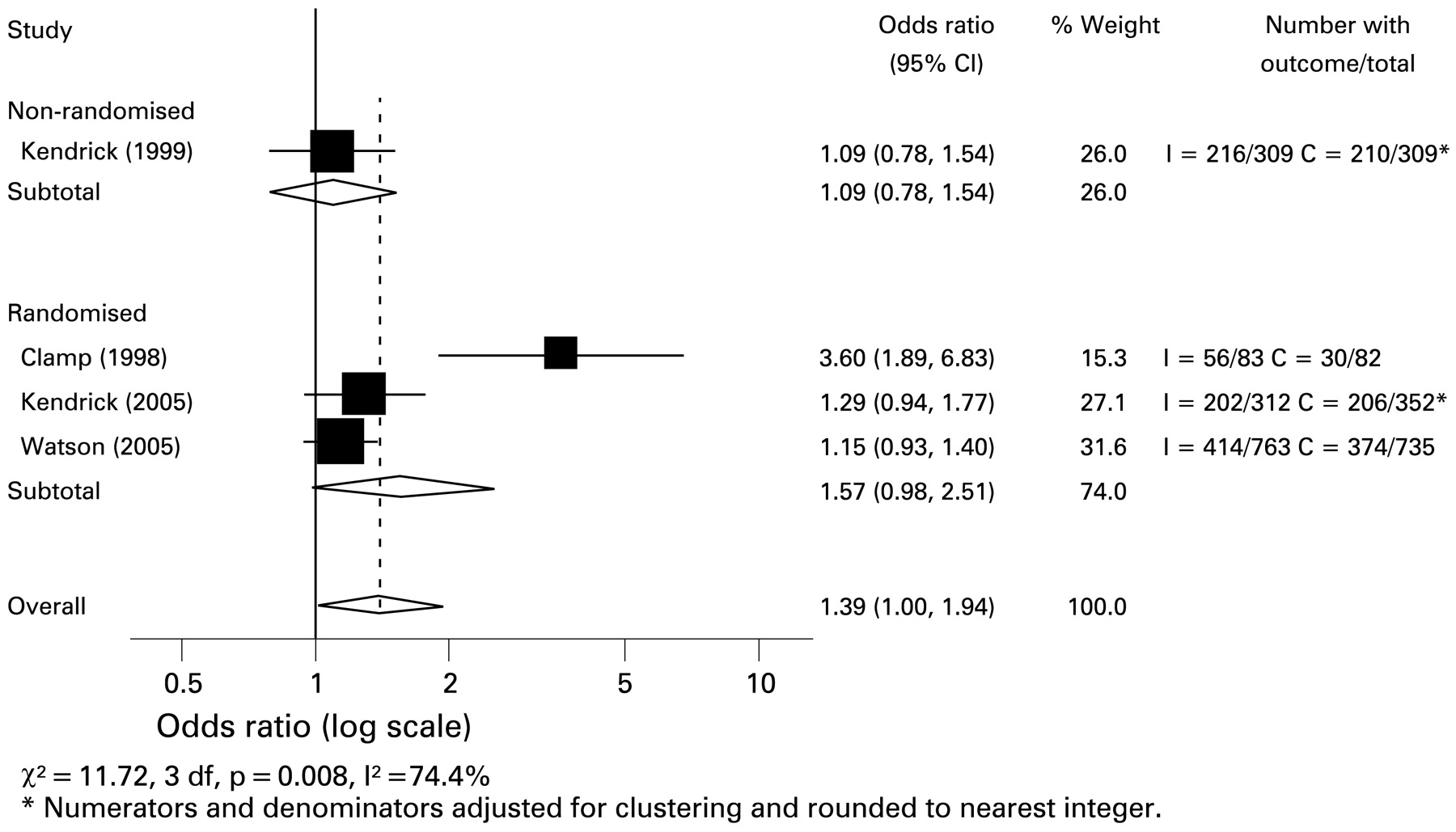
Home safety interventions were effective in increasing the proportion of families with a functional smoke alarm (fig 2: OR 1.83, 95% CI 1.22 to 2.74; χ2 = 32.16, 12 df, p = 0.001; I2 = 62.7%), particularly when smoke alarms were provided (OR 2.64, 95% CI 1.43 to 4.88 in studies providing alarms and OR 1.09, 95% CI 0.81 to 1.47 in studies not providing alarms) and over a shorter follow-up period (OR 4.45, 95% CI 1.66 to 11.88 in studies with follow-up of ⩽3 months and OR 1.33, 95% CI 1.02 to 1.74 in studies with ⩾4 months follow-up). The interventions were also effective in increasing the proportion of families with a safe hot tap water temperature (fig 3: OR 1.35, 95% CI 1.01 to 1.80; χ2 = 20.01, 10 df, p = 0.03, I2 = 50.0%). Some evidence was found that home safety interventions increased possession of fitted fireguards (fig 4: OR 1.39, 95% CI 1.00 to 1.94; χ2 = 11.72, 3 df, p = 0.008, I2 = 74.4%), and a greater effect over a shorter follow-up period was found (OR 3.60, 95% CI 1.89 to 6.84 in the one study with follow-up of ⩽3 months and OR 1.17, 95% CI 1.00 to 1.36 in studies with ⩾4 months follow-up). We found a lack of evidence that home safety interventions were effective in increasing possession of fire extinguishers (OR 0.96, 95% CI 0.41 to 2.23; χ2 = 14.82, 3 df, p = 0.002, I2 = 79.8%), although the single study that provided free fire extinguishers did find a positive effect (OR 4.67, 95% CI 1.78 to 12.25). There was a lack of evidence that home safety interventions were effective in helping parents keep matches or lighters (OR 1.23, 95% CI 0.56 to 2.68; χ2 = 7.01, 4 df, p = 0.135, I2 = 43.0%) or hot drinks or food out of reach of children (OR 0.89, 95% CI 0.66 to 1.18, χ2 = 2.34, 3 df, p = 0.504, I2 = 0.0%). The combined number of participants in the intervention and control arms for these latter three outcomes were small (fire extinguishers: intervention arms = 664, control arms = 657; matches and lighters: intervention arms = 987, control arms = 979; hot drinks or food: intervention arms = 487, control arms = 496).
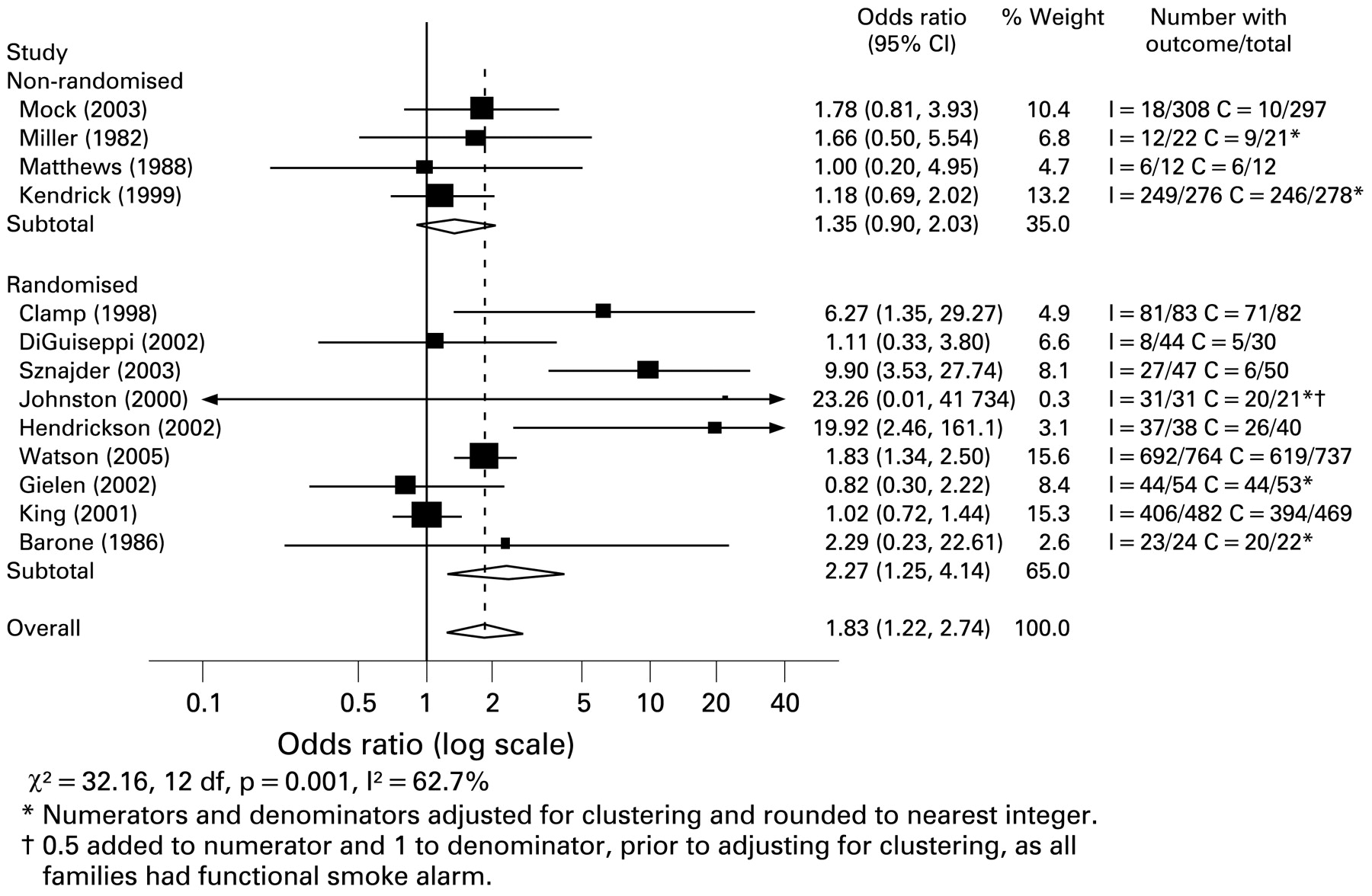
Odds ratios for possessing a functional smoke alarm, by study design.

Odds ratios for having a safe hot tap water temperature, by temperature.
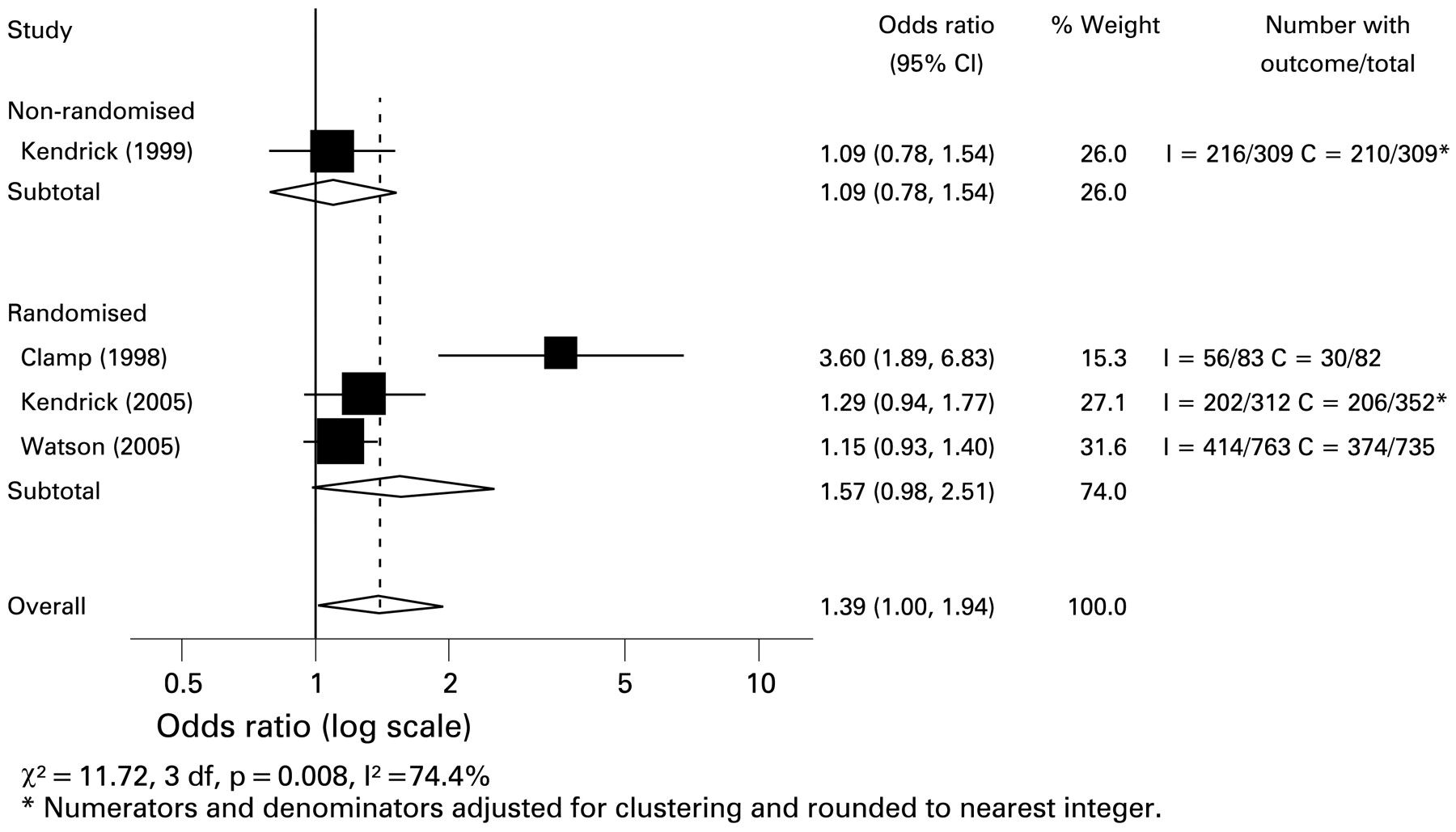
Odds ratios for possession of fitted fireguard, by study design.
Does the effect of home safety interventions vary by child age, gender or social group?
Table 3 shows the effects of home safety interventions by child age, gender and social group. We found no consistent evidence that the effectiveness of interventions varied by child age, gender or social group, with only interventions to increase fireguard use being found to be more effective in families with female than male children (ratio of odds ratios for effect in boys vs effect in girls: 0.61, 95% credible interval 0.43 to 0.85). We were unable to assess variations in effectiveness of interventions to increase fire extinguisher possession and safe storage of matches and lighters for some groups due to small number of studies or small subgroup numbers.
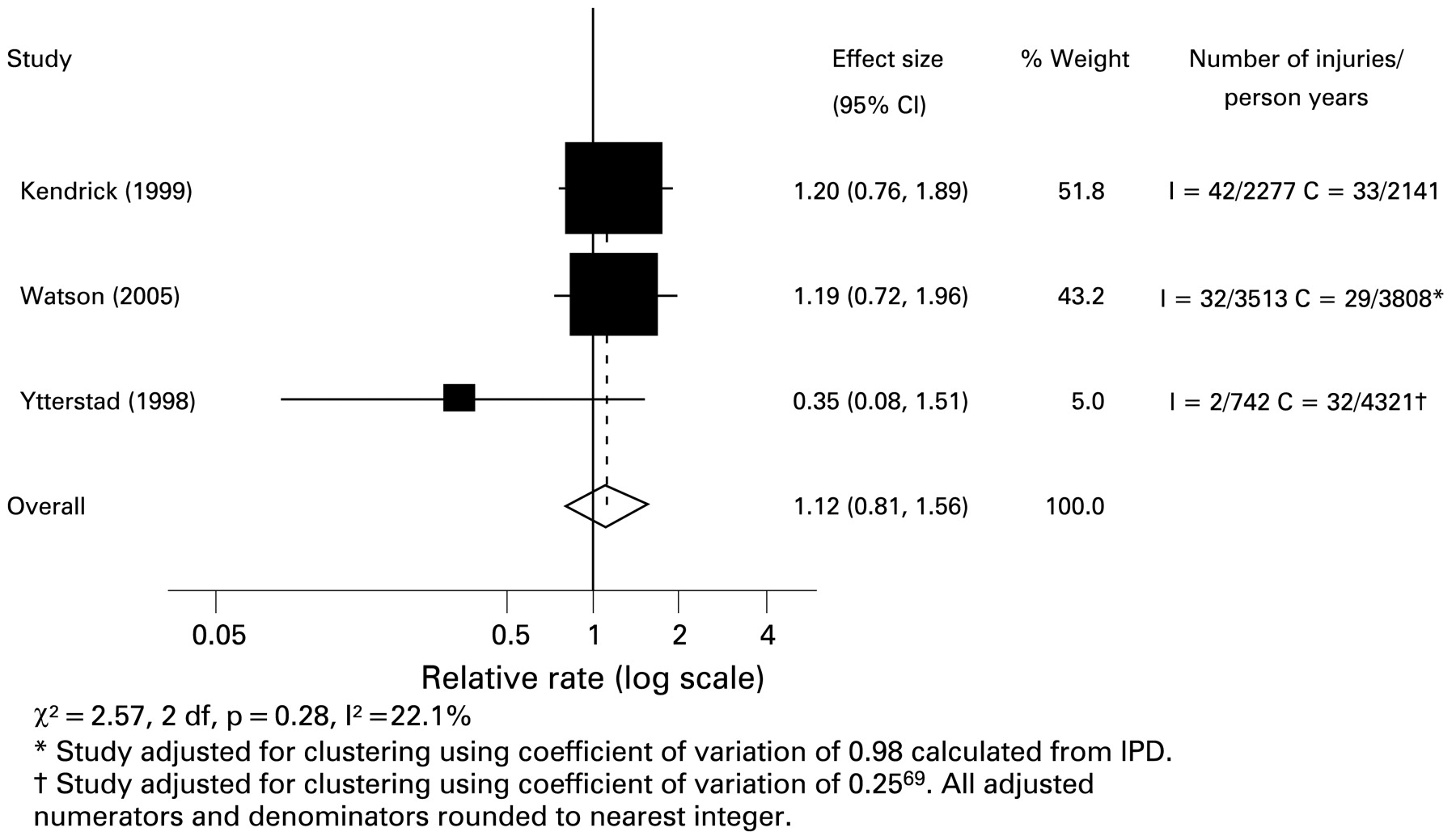
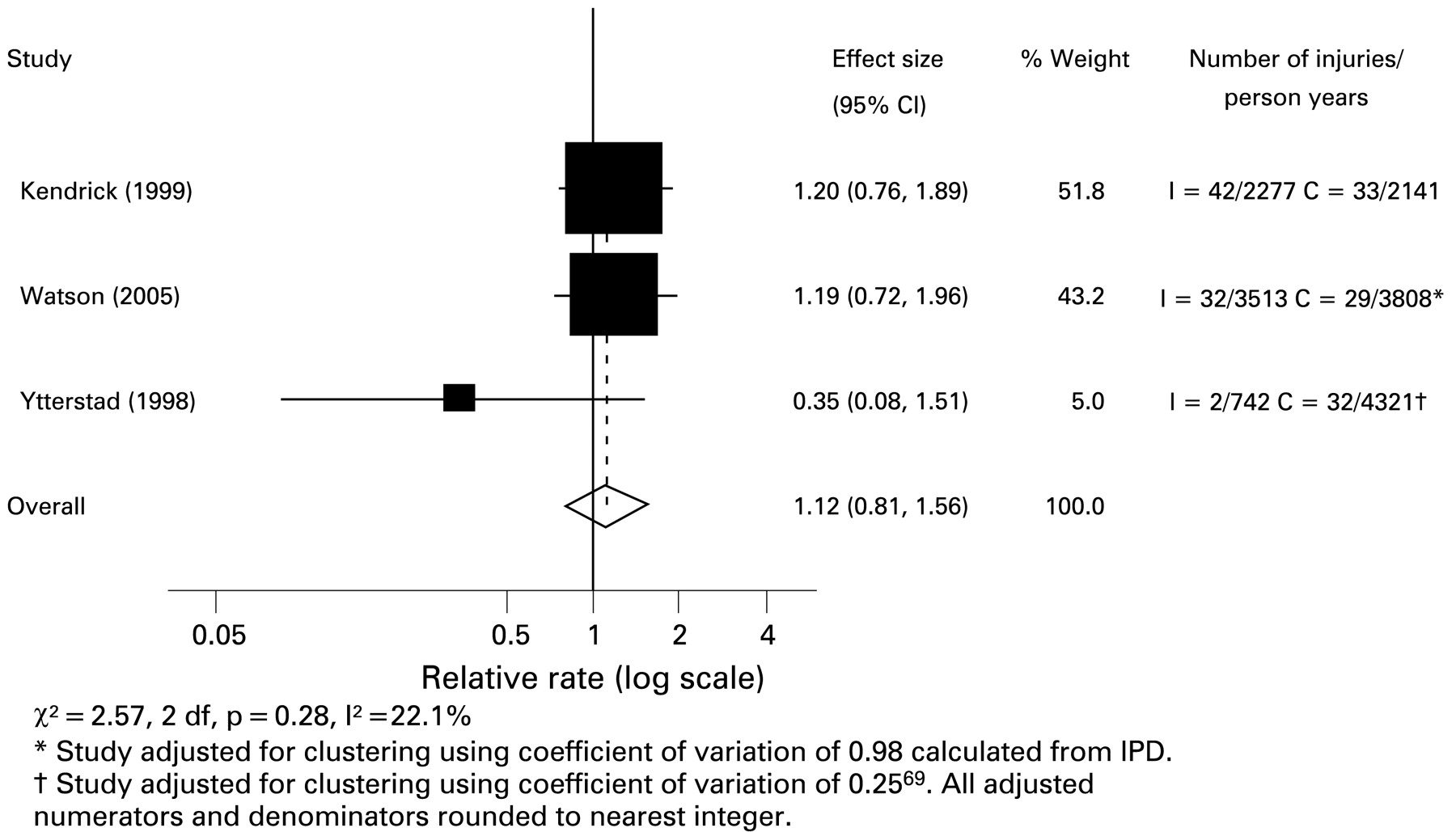
There was a lack of evidence that home safety interventions reduced medically attended thermal injury rates (fig 5: IRR 1.12, 95% CI 0.81 to 1.56; χ2 = 2.57, 2 df, p = 0.28, I2 = 22.1%). The combined number of person-years was 6532 and 10 270 in the intervention and control arms, respectively.
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Incidence rate ratios for medically attended thermal injury.
DISCUSSION
Main findings
Our meta-analyses have found that home safety education was effective in increasing the proportion of families having a safe hot tap water temperature and a functional smoke alarm, and there was some evidence that it may be effective in increasing the use of fireguards. Effect sizes appeared to be larger where safety equipment was provided in addition to education and over shorter rather than longer time periods for some outcomes. However, significant effects were found for follow-up periods of 4 months or more for having a safe hot tap water temperature, a functional smoke alarm and a fitted fireguard. Overall there was a lack of evidence that home safety education increased possession of fire extinguishers, helped parents keep matches and lighters or hot food and drinks out of reach, or reduced rates of thermal injuries. We were also unable to find consistent evidence that effectiveness of interventions varied by social group, with a significant difference being found only for interventions in increasing fireguard use by child gender.
The findings were robust to study quality except that effect sizes were smaller among the two studies reporting having a functional smoke alarm with blinding of outcome assessment (OR 1.02, 95% CI 0.73 to 1.43) than among those without blinded outcome assessment (OR 3.50, 95% CI 1.47 to 8.36).
Strengths and weaknesses of the review and meta-analysis
Our review and meta-analysis comprises the largest and most comprehensive published evaluation of the effect of home safety education, with or without the provision of safety equipment to date. It is also the first meta-analysis to obtain IPD and to use this, via a novel statistical model, to examine the effect of home safety interventions by child age, gender and social variables. Our inclusion of non-randomised designs increased the power of the analyses and did not appear to bias the results, as we found similar effect sizes in meta-analyses of randomised and non-randomised designs.
The majority of studies included in the meta-analyses were RCTs; the findings were robust to study design and quality except that effect sizes were smaller among studies reporting having a functional smoke alarm with, than without blinding of outcome assessment. However only two studies used blinded assessment of outcomes, so caution must be exercised in interpreting this finding.
We found significant heterogeneity in effect sizes for three outcomes. Factors including the provision of safety equipment and follow-up period explained some of the heterogeneity for some outcomes and the meta-regression analyses suggest that some heterogeneity in the fireguard analysis may also be explained by child gender. It is also possible that differences in the content and delivery of the interventions may explain some of the observed heterogeneity.
Our findings in relation to a safe hot tap water temperature must be considered in the context of more recent recommendations about the temperature that can be considered “safe”. The lowest temperature defined as “safe” by authors of the studies included in our review was 49°C, but 46°C is the temperature currently recommended by the Child Accident Prevention Trust.43 It is therefore possible that home safety education, although effective in reducing hot tap water temperatures, may not do this sufficiently to reduce the incidence of scalding.
The small number of studies containing a relatively small number of participants for the analyses for fire extinguishers, keeping hot food and drinks or matches and lighters out of reach and for thermal injuries is likely to have resulted in insufficient power to detect moderate or small effect sizes.
Although the vast majority of thermal injury deaths occur in low and middle income countries,3 all but one of the studies41 included in our review report interventions implemented in higher income countries. This study, set in Mexico had a similar odds ratio for functional smoke alarms to other studies which did not provide smoke alarms. The transferability of such interventions to low and middle income countries remains to be evaluated, as do interventions targeting the specific thermal injury problems faced by these countries.
Comparisons with previous research
Our findings build on those of the two reviews and meta-analyses by DiGuiseppi and colleagues.1415 In relation to functional smoke alarm ownership our findings are more positive than those in the first review,14 which found a significant effect only where safety advice was provided as part of routine child health surveillance and only on ownership not functioning of smoke alarms. Our finding of significant effects of home safety education on smoke alarm function are likely to reflect the inclusion of a larger number of studies and the inclusion of at least one recent large study with positive findings in our meta-analyses. In addition our analyses included a greater number of studies that provided smoke alarms, and as we found larger effects among studies providing smoke alarms than among those not providing alarms, this is also likely to help explain our more positive findings.
The second review and meta-analysis by DiGuiseppi and Roberts examined the effect of interventions delivered in a clinical setting to increase smoke alarm ownership, promote a safe hot tap water temperature and to “childproof” the home.15 They found that interventions delivered in a clinical setting were effective in promoting a safe hot tap water temperature and in increasing smoke alarm ownership. Only two of the studies included in this review reported injury outcomes, neither finding a significant reduction in injury occurrence, leading to the conclusion that clinical counselling had little effect on most home safety practices designed to childproof the home and that the evidence about the impact of counselling on childhood injuries was limited.15 Again our more positive findings are likely to reflect our examination of a wider range of outcomes and, as more studies had been published, our inclusion of a larger number of studies, including some with a large number of participants1130 and some demonstrating very positive effects for some outcomes.252628 Our findings regarding injury outcomes are consistent with those of DiGuiseppi and colleagues, as despite recent larger studies that have measured injury outcomes,11 there remains a lack of evidence that home safety education can reduce childhood injury rates.
Ours is the first meta-regression examining the effect of home safety education by child age, gender and social group. However, our findings are consistent with those from four primary studies. Two RCTs found that the effect of home safety education plus provision of safety equipment did not differ in effect by social variables,811 while one RCT found that it appeared to be more effective among single parent families and those with low levels of education, but less effective among families with two or more children.26 One CBA found no evidence of a differential effect of home safety education by socioeconomic status.41
Interpretation of our findings
Although the interventions we reviewed improved thermal injury prevention practices, we were unable to demonstrate a reduction in injury rates. Several possible explanations exist. First, the analyses are likely to have been underpowered to detect anything other than a large treatment effect on thermal injury rates. Second, a large treatment effect may be implausible, especially given the relatively small increase in the percentage of families with particular thermal injury prevention practices we observed. Third, safety equipment may not be effective in reducing thermal injury rates. While this is possible, and acknowledging the potential for bias in observational studies, this is inconsistent with the body of observational evidence available to date.44–48 Finally, thermal injury encompasses a diverse group of injuries and injury mechanisms, and the interventions tested in the studies included in our review could prevent only a proportion of thermal injuries; for example, lowering tap water temperature would reduce the risk of scalds while bathing but not while cooking.
While our failure to demonstrate consistent variations in the effect of interventions by child age, gender or social variables is encouraging, many of our meta-regression analyses will have been underpowered to detect anything other than large differences between groups, so smaller variations in the effect of interventions by age, gender or social group may exist.
Implications for injury prevention research and practice
Our findings suggest that home safety education, especially with the provision of safety equipment, is effective in increasing some thermal injury prevention practices, but the evidence to show whether this also reduces thermal injury rates is insufficient. Further trials measuring and recording injury outcomes would help to answer this question. Such trials would need to be extremely large, would be very expensive, logistically difficult and in today’s research funding climate are unlikely to be funded. Furthermore, the point of clinical equipoise may well have passed in many countries. In England for example, the government has announced funding for a national safety equipment scheme,49 so persuading families and health professionals that the effectiveness of safety education and equipment still requires testing, and that equipment should be withheld from some families would be difficult. Under these conditions an alternative is to carry out observational studies that measure and adjust appropriately for a wide range of confounding factors. Further examination of variations in effectiveness by age, gender and social variables is required; hence future studies need to collect and report data on these variables, preferably in a standardised way. As meta-regression using IPD is much more powerful than that using summary data, it is also important that the community of injury researchers is willing to share their individual participant data for future analyses.
It is vital to address thermal injury prevention in low and middle income countries where thermal injury rates are high.3 This should include an evaluation of the appropriateness of the interventions we studied in low and middle income countries.
Our findings suggest that home safety education and the provision of safety equipment for the prevention of thermal injuries should continue to be provided while further evidence relating to the effect of such interventions on injury rates is sought. However, education and the provision of safety equipment are only one approach to preventing thermal injuries, and a comprehensive thermal injury prevention strategy should include other approaches such as legislation (eg, pre-setting of hot water heater thermostats, child resistant cigarette lighters) and modification of the environment (eg, thermostatic mixer valves).
Key points
What is already known on this topic
Previous systematic reviews and meta-analyses have found some interventions to be effective at increasing parental thermal injury prevention practices.
Little is known about whether interventions to prevent thermal injuries vary in their effectiveness by age, gender and social group or about their effect on thermal injury rates.
What this study adds
This meta-analysis includes several large studies not included in prior meta-analyses.
As a result, it is the first to find that education programmes may be effective in increasing the use of fireguards.
Home safety education did not increase possession of fire extinguishers, help parents keep matches and lighters or hot food and drinks out of reach or reduce rates of thermal injuries.
Meta-analysis suggests that home safety education was not effective in reducing rates of thermal injuries.
Acknowledgments
DK conceived this review and coordinated its preparation. DK, AS, CC and MW contributed to discussions about core ideas and design of the study. DK, AS and CC undertook the statistical analysis. CM, AW and SS collected and extracted the data and carried out quality scoring. DK and SS wrote the paper, with all contributors assisting in drafting the manuscript.
REFERENCES
Supplementary materials
Web only appendices 15;3:197
Files in this Data Supplement:
Footnotes
▸ Tables 1 and 2 are available online only at http://injuryprevention.bmj.com/content/vol15/issue3
Competing interests: None.