Article Text

Abstract
Objectives: To examine and discuss the implications on the incidence of hospitalised injuries of selecting cases from principal diagnosis field only compared with considering all diagnosis fields, the inclusion compared with the exclusion of medical injuries, and the impact of identifying multiple admissions.
Methods: Analysis of data from the 1999–2000 New South Wales Inpatient Statistics Collection, Australia, including an internal linkage of the same dataset.
Results: Approximately 27.5% of records with a non-injury primary diagnosis include a nature of injury diagnosis in a subsequent diagnostic field. This figure increased to more than half (53%) of discharges for medical injuries. The internal linkage showed that 6.5% of discharges were repeat admissions for the same International Classification of Diseases, 10th revision (ICD-10) injury code and that 13.8% were repeat admissions for any ICD-10 injury code. The proportions of repeat admissions varied according to the type and the mechanism of injury.
Conclusions: Selecting hospitalised injury cases from the principal diagnosis alone would underestimate medical injury cases as well as other injuries occurring in hospital. Repeat admissions should always be considered particularly in the case of thermal injuries, self harm, and medical injuries. Due to the limitations of data linkage, alternative methods need to be developed to identify repeat admissions. Other areas in which further research would be beneficial to a more uniform reporting of injury hospitalisations include better identification of injuries occurring in hospital, a review of ICD-10 injury codes, and the development an ICD-10 based severity measure which can be readily used with hospital discharge data.
- hospitalised injuries
- numerator issues
- CI, confidence interval
- ICD, International Classification of Diseases
- NSW, New South Wales
- hospitalised injuries
- numerator issues
- CI, confidence interval
- ICD, International Classification of Diseases
- NSW, New South Wales
Statistics from Altmetric.com
- hospitalised injuries
- numerator issues
- CI, confidence interval
- ICD, International Classification of Diseases
- NSW, New South Wales
- hospitalised injuries
- numerator issues
- CI, confidence interval
- ICD, International Classification of Diseases
- NSW, New South Wales
Although hospitalised injuries represent a relatively small proportion of all non-fatal injuries,1 they are generally more severe, are associated with higher medical and treatment costs than those treated in outpatient clinics, and are widely used to measure the burden of injury.2 Eleven injury indicators, identified by the Australian National Health Priority Area, are based on hospital separations data.3 However, methods of analysing and reporting the incidence of hospitalised injuries in the literature, that is injury incidence through the use of hospitalisation data, have been inconsistent. This has made it difficult to make meaningful comparisons between various reports. This inconsistency is mainly related to using different criteria when defining injury and different methods of dealing with multiple counting of some incident cases due to readmissions and transfers. Most reports define injury hospitalisations as those coded within the International Classification of Diseases, 10th revision (ICD-10) chapter XIX injury, poisoning ‘(S00–T98),2 or the corresponding ICD-9 nature of injury diagnosis codes (800–999). However, because hospital discharge collections allow for a number of diagnosis fields, some researchers define injury cases as those coded in the principal diagnosis field only,3–11 while others use additional secondary fields to select these cases.12–14 Similarly while some reports include injuries resulting from complications of medical interventions,10,14 others exclude them for various reasons.5,15 In addition, some researchers use different methods to distinguish first time admissions and subsequent readmissions and/or transfers,3,5,6,12,16–19 while others simply assume that each discharge refers to a single episode of injury.10,14
The current study sought to examine the effects of these approaches on the reporting of injury incidence using hospital discharge data in order to enhance the consistency of reporting. The specific aims of the study were to:
-
Investigate the effect of defining injury cases from the principal diagnosis field alone or from any diagnosis field on the number and nature of cases identified.
-
Examine the impact of including medical injuries on counts of injury cases.
-
Investigate the extent to which repeat admissions inflate estimates of the incidence of injury.
-
Identify other areas where further methodological research is needed to improve reporting of injury incidence.
METHODS
The data analysed in this study (Inpatient Statistics Collection) covers all inpatient separations, also referred to as hospital discharges, from public and private hospitals in New South Wales (NSW, Australia) during a one year period from 1 July 1999 to 30 June 2000. The collection enumerates periods of stay in hospital which end with either a discharge, transfer, or death of a patient. If a patient was admitted to hospital five times in a year, at least five separate records are included in the collection.20
Internal linkage of Inpatient Statistics Collection data from 1999–2000 was performed by the NSW Health Department, using AUTOMATCH linkage software.21 Records were divided into blocks based on hospital code, medical record number, date of birth, year of birth, month of birth, day of birth, sex, postcode as well as soundex (phonetic algorithm) of locality, and street names. Probabilistic matching techniques were then applied to each block. Weights were assigned based on the level of agreement on each matching criterion and thresholds were set to select “true” links. Matching variables used comprise date of birth, country of birth, sex, insurance status, language spoken at home, marital status, aboriginality, postcode, hospital code, address, medical record number, and admission and separation dates.22
For the period of the study (1999–2000), the nature (diagnosis) and the circumstances of injury (external causes) were coded according the 10th revision of the ICD, Australian modification.2 In addition to the principal diagnosis field, the collection contains up to 20 other diagnosis fields. For the purpose of this study, injuries coded in the principal diagnosis field will be referred to as “primary injuries” and those coded in the other diagnosis fields, with primary diagnosis as non-injury, will be referred to as “secondary injuries”. In addition injuries coded as complications of surgical and medical care not elsewhere classified (T80–T88), also known as iatrogenic conditions, are called “medical injuries” in this paper.5 The rest (S00–T79 and T89–T98) are referred to as “non-medical injuries”.
When analysing the linked data, we examined repeat admissions for hospital separations with a principal diagnosis of injury and poisoning. “Repeat admission rates” refer to proportions of separations identified by the data linkage as links to the first admission and include both readmissions and transfers. The rates of repeat admissions for both the same ICD-10 (up to the fifth character) injury code as well as for any ICD-10 injury code were analysed across age, gender, mechanism, and type of injury. These criteria were field specific. That is only codes appearing in the principal diagnosis field were examined for both first admission and potential repeat admissions. For all repeat admission rates, 95% confidence intervals (CI) were calculated, assuming the binomial distribution. The analysis was carried out using SAS Statistical software.23
We have chosen to identify injury and repeat admission cases by using diagnosis rather than external cause codes because the data show that while all injury cases had external cause codes, having an external cause code did not necessarily mean that the patient had an injury. In addition, unlike diagnosis codes, the quality of data in the external mechanism fields is practically unknown and needs to be assessed.3
RESULTS
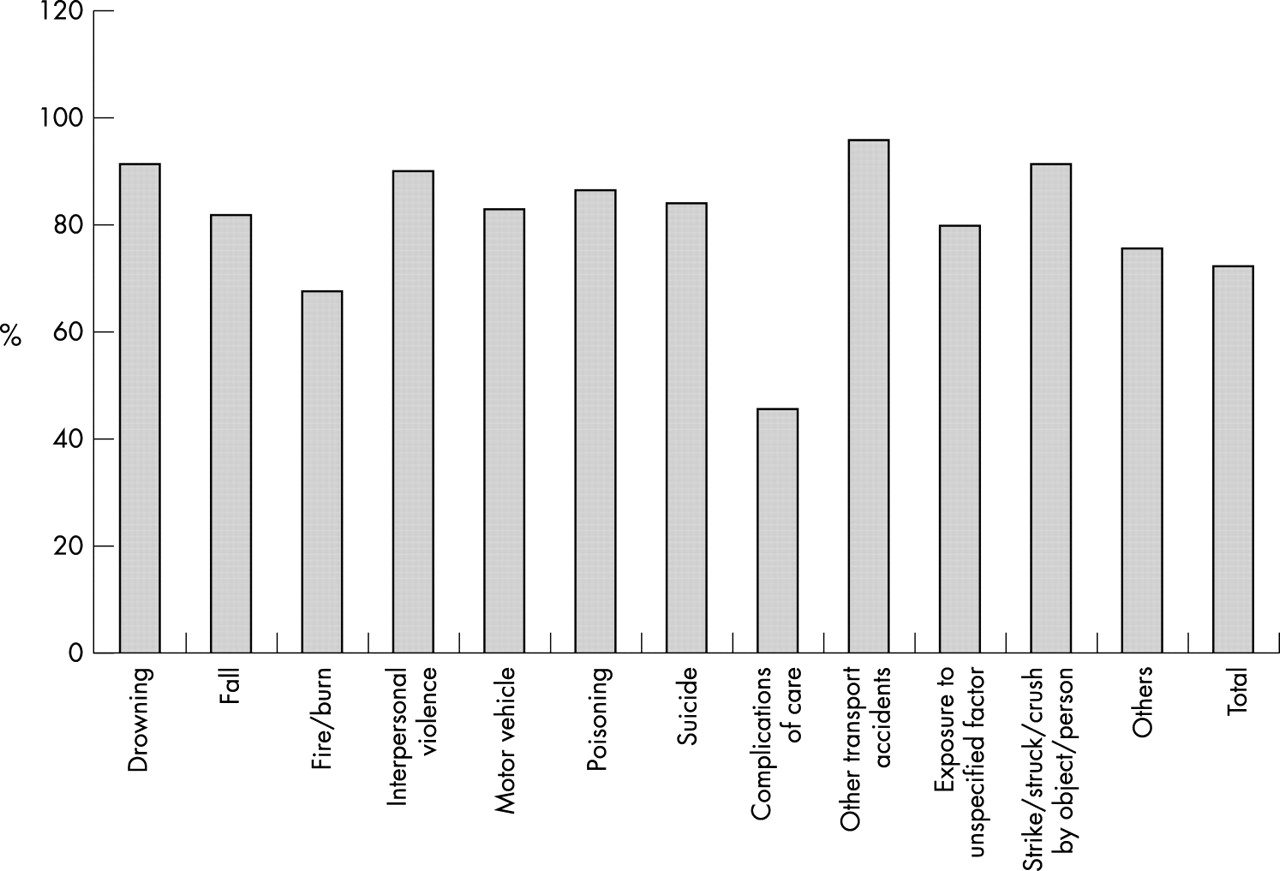
During the period of the study, there were 178 594 hospital separations of NSW residents for injury and poisoning. Selecting injury cases from primary diagnosis field only, reduces the overall number of these cases by approximately a quarter (27.5%) (table 1). This varied according to the type of injury, with 81% of non-medical injury separations identified from the principal diagnosis field compared with less than half (47%) for separations for medical injuries. The proportion of injury cases coded in the principal diagnosis field also varied by mechanism of injury; the highest being other transport accidents (96%). Complications of medical care (46%) and thermal injuries (68%) had the lowest rates of primary injuries (fig 1). Excluding medical injury also reduces the number of discharges identified by all injury codes by 25.1% and the number of those recoded in the principal diagnosis field by 16.2%.
Hospital separations for injury and poisoning by type of injury and ICD-10 diagnosis field; NSW, 1999–00

{kind=link}
Proportions of injury separations and poisoning coded in the primary diagnosis field by mechanism; NSW, 1999–2000.
The internal linkage showed that 6.5% (95% CI 6.3% to 6.6%) of separations were repeat admissions for the same ICD-10 injury code and 13.8% (95% CI 13.6% to 14.0%) were repeat admissions for any ICD-10 injury code. While in both cases, repeat admissions were highest among those aged from 40–44 years, repeat admissions for any ICD-10 injury code generally increased with age while repeat admissions for the same injury code seem to show little variation across age with the exception the 40–44 years age group (table 2). The rates of repeat admissions for the same ICD-10 injury code as well as those for any injury code were slightly higher among females than male. This gender difference was not, however, significant. On the other hand, the rates of repeat admissions were significantly higher for medical injuries compared to non-medical injuries (table 3). These rates varied also according to the mechanism of injury with complications of care having the highest rates of repeat admissions for the same ICD-10 injury code (12.0, 95% CI 11.5 to 12.4) and of repeat admissions for any ICD-10 injury code (23.0, 95% CI 22.4 to 23.6) (table 4).
Number and percentage of repeat hospital admissions, for separations with a principal diagnosis of injury and poisoning for injury, by age; NSW, 1999–2000
Number and percentage of repeat hospital admissions, for separations with a principal diagnosis of injury and poisoning for injury, by type of injury; NSW, 1999–2000
Number and percentage of repeat hospital admissions, for separations with a principal diagnosis of injury and poisoning, by mechanism of injury; NSW, 1999–2000
DISCUSSION
Selection of injury cases based on principal diagnosis
The results showed that the majority of cases, over 80% of non-medical injuries and 73% of all injury separations, were coded in the primary diagnosis field. Similar results have been found elsewhere.5 It has been argued that when examining injury incidence using hospital data, only the principal diagnosis code should be considered because it represents the condition to which the episode in hospital is most attributable.3 Taking into account secondary diagnosis fields would consequently include injuries which may not have been serious enough to be admitted to hospital.
Another argument against the use of secondary diagnosis fields is the variation in the number of diagnosis fields provided in hospital discharge data between places and particularly over time.3 For instance before July 1999, the Inpatient Statistics Collection contained only 10 diagnosis fields compared with the current 21 fields. Inclusion of all diagnosis fields would consequently introduce biased estimates when examining trends of hospitalised injuries over time.
On the other hand, not taking into consideration secondary diagnosis fields, would exclude more than half of medical injuries (53%) and all injuries which occur in hospital (that is, falls from hospital beds) and are not coded as the main reason for admission. Unfortunately, in this study, it was not possible to determine the number of these injuries because the ICD-10 “place of occurrence of injury” code does not indicate specifically whether the injury has occurred in hospital.
Alternative methods of selecting injury cases
Various approaches have been suggested to deal with this issue such as considering all diagnosis fields when dealing with medical injuries and injuries that arose during hospital stay, while examining only primary diagnosis for the rest of the injuries.24 Another alternative is to consider all diagnosis fields for all injuries with a severity level deemed high enough to require hospitalisation. This will allow filtering out secondary injuries which may not, on their own, have been serious enough to require hospitalisation. In fact a case definition of injury based on some severity threshold would allow more comparable incidence rates that are less influenced by factors such as accessibility to facilities and variations in clinical and administrative criteria governing the decision to admit.3,25,26 Length of stay has been increasingly used as a proxy of severity, with a number of studies excluding one day admission cases for injury.6,27,28 However, length of stay is also influenced by factors such as admission policies and availability of hospital beds. It might therefore be useful to develop an injury severity scale, such as the ICD injury severity score,29 based on the ICD-10 classification and which can be readily used with the current hospital discharge databases.
Medical injuries
The results of this analysis showed that more than half of hospital separations for medical injuries were secondary injuries. As discussed above, ignoring secondary diagnosis fields would therefore underestimate the magnitude of medical injuries. Some researchers, however, advocate the exclusion of these injuries from studies examining the incidence of hospitalised injuries because they have different aetiology and means of prevention to other types of injury.5,30 We do not believe that this argument is compelling enough to exclude medical injuries because various types of injury contained in the hospital data also have different risk factors and means of prevention.
Others argue that the ground for exclusion should be based on whether medical injuries meet the theoretical definition of injury and that many medical injuries appear not to.31 To support this argument, ICD codes relating to “Mechanical complication of medical devices” are advanced to typify these cases. While it can be argued that these cases might not be considered injuries in the theoretical sense of the term, our data show that they only make up 13% of medical injuries. In our view, while many medical injuries coded in chapter XIX of the ICD-10 might not be described as traumatic injuries, they nevertheless meet the theoretical definition of injury as “damage to cells and organs from energy exposures that have relatively sudden and discernible effect”.32 In addition, codes for some conditions associated with medical care that might be perceived as falling within the scope of injury or poisoning are not included in the injury chapter and are placed elsewhere in the classification (for example, complications of surgical procedures during pregnancy, childbirth, and the puerperium, ICD-10: O00–O99).
Cases of injuries and poisoning resulting from medical interventions are increasingly becoming a major public health issue.33 In our view, the reasons for excluding or including them should be explicit and supported by empirical evidence, if necessary. We also believe that there is a case for reviewing ICD-10 medical injury codes.
Repeat admissions
The results indicated that 6.7% and 13.8% of all hospitalised injuries were repeat admissions in the same year for the same ICD-10 injury code and for any ICD-10 injury code respectively. These estimates varied according to age and mechanism of injury indicating that repeat admissions should be particularly considered in the case of admissions for thermal injuries, self harm, and medical injuries. The higher repeat admissions rates for these injuries are likely to be due to readmissions for follow up treatment or ongoing rehabilitation (for example, skin grafting after thermal injury).
It is important to note that the record linkage method used in this study relied heavily on the person’s address, date of birth, sex, and medical record number. While linkage rates of persons admitted to the same hospital are likely to be good, admissions to other hospitals may not be as reliable. Data linkage of injury events using variables such as unique personal identification and date of injury are more likely to produce more reliable estimates of readmissions.34 Unfortunately, the NSW Inpatient Statistics Collection does not have such identifiers. Their introduction would, therefore, be useful in identifying repeat admissions cases.
However, even when using identifiers with high discriminative power such as unique personal identifiers, record linkage has a number of limitations as a method to determine first hospital admissions for injury. First, the principal diagnosis for a particular hospitalised injury case might change for subsequent readmission(s) especially in the case of multiple injuries. Australian coding guidelines indicate that in the case of multiple injuries, the injury which presents the most serious threat to life should be assigned as the principal diagnosis; the “multiple injuries” code should only be used where the number of injuries to be coded exceeds that of diagnosis fields available.35 However, the severity of an injury as well as the likelihood of using the “multiple injuries” code might change for subsequent readmissions leading to an underestimation of the number of repeat admissions.
It is also possible that a repeat admission, as identified by record linkage, for the same ICD-10 injury code and the same mechanism could actually be related to a new injury resulting in underestimation of incident cases. For example, an admission of a new suicide attempt using the same means and resulting in the same injury or a fracture of the hip on the opposite side from a new fall. Another limitation of record linkage is that readmission for an initial injury, which might have occurred and resulted in a hospital admission and discharge, outside the period of the linked data, in this case before 1 July 1999, would not be identified. Further, record linkage, as a method of identifying repeat admissions, is far from being practical as the linkage process itself is lengthy and relatively expensive.
Other methods of identifying incident cases
In order to identify first time admissions, some researchers have also excluded discharges with sequelae of injuries and poisoning codes (T90–T98), viewed as unlikely to be incident cases.3,5,12 The impact of excluding these cases is likely to be minimal as our data show that they represent only 0.38% of injuries coded in the primary diagnosis field (results not shown). While one could presume that most of these separations would have been hospitalised previously and should be excluded, it is possible that an injury is first hospitalised because of a complication.
Other studies have also used admission, separation, and readmission variables to deal with the issue of repeat admissions. When examining these variables, our data show that 11.2% of separations with principal diagnostic as injury were transferred to another hospital, 7% were transferred from a hospital, and 11.35% were readmitted to hospital within 28 days of the previous admission (results not shown). While these variables are readily available in most hospital discharge datasets, they lack the ability to specifically identify repeat admissions for the same injury and are likely to include transfers and readmissions for a number of conditions other than injury. In addition the variable “readmitted to hospital within 28 days” is likely to miss readmissions for long term complications of injury.
Perhaps the most practical and straightforward method of determining repeat admissions is the inclusion of a “first admission” variable. As Smith et al suggested, the discharge sheet should include a box in which the coder indicates “Is this the first admission to a hospital for this condition? Yes/No/Unknown”.5 A similar strategy was used in New Zealand with the introduction of the “readmission indicator”. It has become apparent, however, that this field was not well reported and the indicator was no longer mandatory.36 Thus, the “first admission” variable needs to be introduced in close collaboration with health information stakeholders in order to ensure the appropriate training of coders regarding its use. After its introduction validity/follow up study(s) would be useful to evaluate its performance in indicating repeat admissions.
CONCLUSIONS
While we have not addressed all the issues related to what are commonly referred to as “numerator problems” in injury epidemiology,37 this study focused on areas considered to be the origin of inconsistencies between studies reporting the incidence of hospitalised injuries. These areas include repeat admissions for injury, number of diagnosis fields from which the cases are selected, and the inclusion or otherwise of medical injuries. Discussion on how to deal with medical injuries is currently developing among injury prevention researchers through the International Collaborative Effort on Injury Statistics.38 A decision on this issue is important, since it has implications for the number of diagnosis fields to be considered when selecting incident injury cases. The aim of the current study was to primarily stimulate debate rather than to provide “prescriptive” methods of reporting hospitalised injuries. The study identified areas in which further research would be beneficial to a more uniform reporting of injury hospitalisations. These include better identification of repeat admissions for injury, a review of ICD injury codes, especially for medical injury, as well as the development of an ICD-10 based severity measure which can be readily used with hospital discharge data.