Article Text

Abstract
Background: Falls from balconies and windows are an important cause of childhood injury. This study investigated the circumstances around such falls and attempted to identify possible measures for their prevention.
Population: Children <15 years living in Dallas County, Texas.
Methods: Each child treated because of a fall from a building in 1997–99 had information about the injury collected, and a parent was contacted to obtain further information. For apartment related falls, an attempt was made to visit the apartment to measure windows and balcony rails.
Results: Ninety eight children were injured in falls from buildings during the three year period; 39 (40%) were admitted to hospital. Seventy five of the falls (77%) involved apartments, and most occurred around noon or evening meal times. Among apartment falls, 39 (52%) fell from windows, 34 (45%) from balconies, and two (3%) from unknown sites. For more than two thirds of balcony related falls, the child fell from between the balcony rails, all of which were spaced more than 4 inches (10 cm) apart. On-site measurement showed the rails were an average of 7.5 inches (19 cm) apart; all of these apartments were built before 1984. For more than two thirds of window related falls, the window was situated within 2 feet (61 cm) of the floor.
Conclusions: Two factors are important in falls from apartment windows and balconies: balcony rails more than 4 inches (10 cm) apart, and windows positioned low to the floor. Current building codes do not apply to older apartments, where most of these falls occurred. Nevertheless, these factors may be amenable to environmental modifications that may prevent most of these falls.
- falls
- balcony
- window
- child
Statistics from Altmetric.com
Falls account for significant morbidity and mortality among young children, and are one of the most common reasons for emergency department visits.1,2 Since the early 1970s, falls from buildings have been recognized as an important cause of injuries and deaths,1,3–6 and a program in New York City that installed window guards in tall apartment buildings led to a dramatic decline in childhood deaths from building falls.3 However, in many other parts of the United States, falls from windows and balconies of apartments are not as likely to result in death,7–10 possibly because apartments are less likely to be as tall in other parts of the country. Nevertheless, these fall related injuries might result in substantial morbidity, if not mortality.7 In addition, we could find no recent studies that included on-site visits and review of pertinent environmental aspects that may contribute to such a fall.10 We attempted to determine the circumstances around childhood falls from apartments in the Dallas County area, including inspection of the pertinent environment in order to identify whether interventions may be developed to prevent these injuries.
METHODS
Between 1 January 1997 and 31 December 1999, we asked the emergency department from each acute care hospital in the Dallas, Texas metropolitan area to report cases of injuries in children <15 years of age due to falls from heights associated with buildings. The Texas Department of Health provided support by requesting hospitals to participate in the investigation. Basic demographic data, diagnosis, and disposition were obtained from the emergency department log, and at least three attempts were made to contact by telephone the parents of each case to administer a standardized questionnaire. The questionnaire elicited specific information about the circumstances of the fall.
It became apparent early in the investigation that apartment balconies and windows were the main locations for the fall associated injuries in this population. Therefore, for cases for which a telephone questionnaire was completed, we also attempted to make a visit to the location of the fall. This allowed us to view the site of the fall and to obtain measurements of windows and balconies, including the height of the window sill or the distance between slats of the balcony railing.
Denominator data for rate calculations were obtained from the 2000 census data for Dallas County, Texas. Data were entered into a database and analyzed using Epi Info version 6.02b, from the Centers for Disease Control and Prevention. Dichotomous variables were compared using χ2 or Fisher’s exact test. To determine whether there had been any fall related deaths in children for the time period in question, we also reviewed log books of the Dallas County Medical Examiner for 1997–99.
RESULTS
Overview
For the three years of the investigation, 108 children <15 years of age were seen in emergency departments for injuries due to falls from buildings. Ninety eight of these were residents of Dallas County (annualized rate: 6.2 per 100 000 Dallas County children age 0–14 years). Ages were known for 97 injured children, and ranged from 1 to 12 years (mean 2.7 years). The highest rate of these fall related injuries occurred in children 0–4 years (15.6 per 100 000), and was considerable lower in 5–9 years (1.5 per 100 000) and 10–14 years (0.8 per 100 000) (table 1). Fifty seven children (58%) were male. Rates of injuries were not significantly different by race or ethnicity (table 1). Seventy four of the cases (76%) were seen at the Children’s Medical Center of Dallas, which had the only pediatric emergency department the Dallas area. Thirty nine (40%) were admitted to a hospital; 56 (57%) were treated in the emergency department and released, and three (3%) were treated in the emergency department but information about whether they were admitted was unknown. Hospital admissions ranged from one to nine days, with a mean and median of two days. Two children had rehabilitation treatment after discharge from a hospital. No child died.
Cases and rates of injuries due to falls from buildings, by various characteristics for children 0–14 years of age, Dallas County, Texas 1997–99
The falls occurred at the following types of buildings: apartments, 75 (77%); houses, 10 (10%); other types of buildings, two (2%); and unknown, 11 (11%). Because apartments comprised the majority of these sites, the rest of the analysis was limited to injuries due to falls from apartments.
Apartments
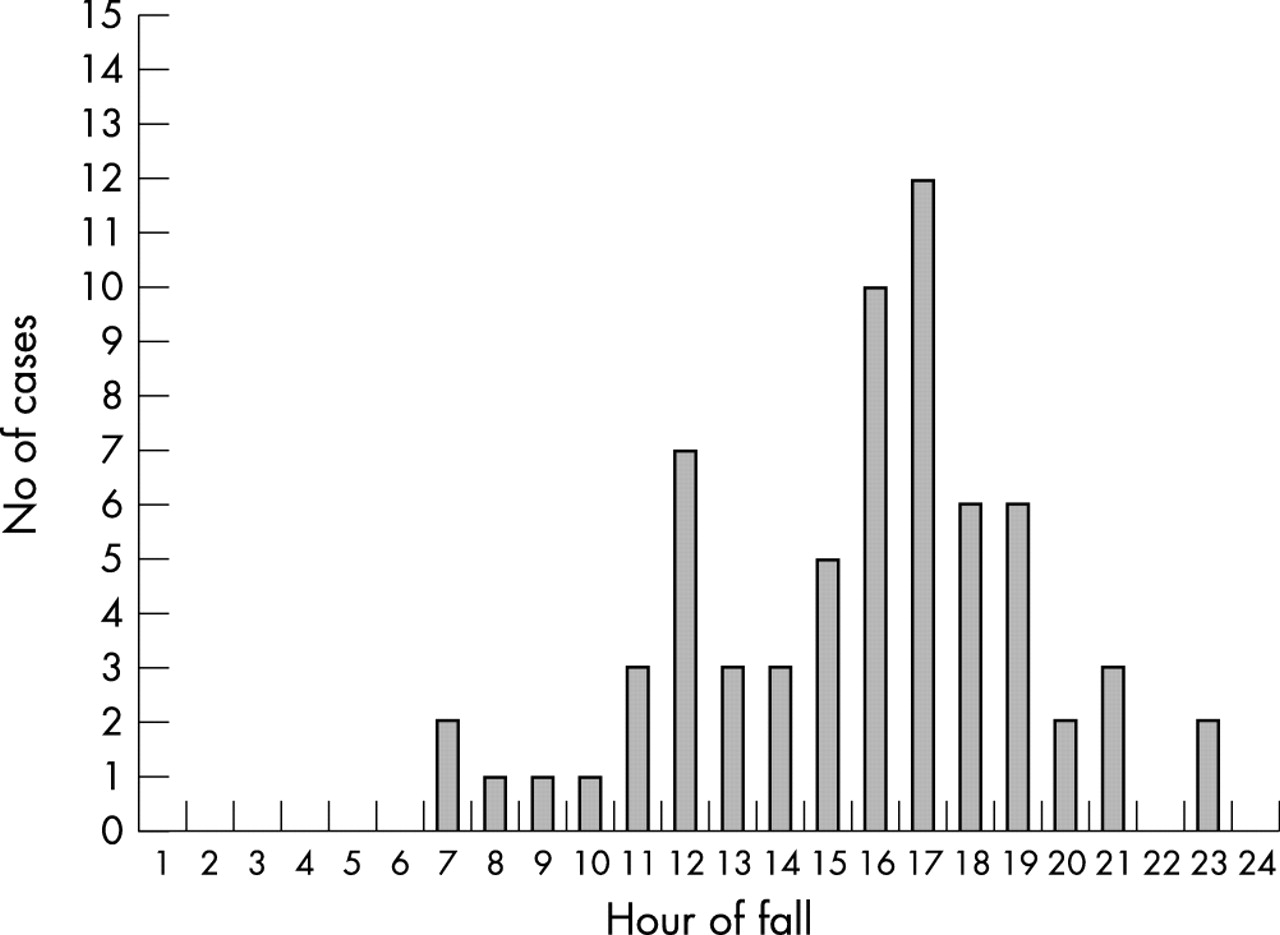
Injuries peaked in spring and autumn months; March, April, May, September, and October accounted for 53 (71%) cases (fig 1). Falls were clustered around meal times. Thirteen (17%) falls occurred between 11 am and 2 pm, and 34 (45%) occurred between 4 and 8 pm. No falls occurred between midnight and 7 am (fig 2). The most common primary diagnoses were related to head injuries, followed by extremity fractures (table 2).
Primary diagnoses* for children injured due to apartment falls, Dallas County, Texas, 1997–99
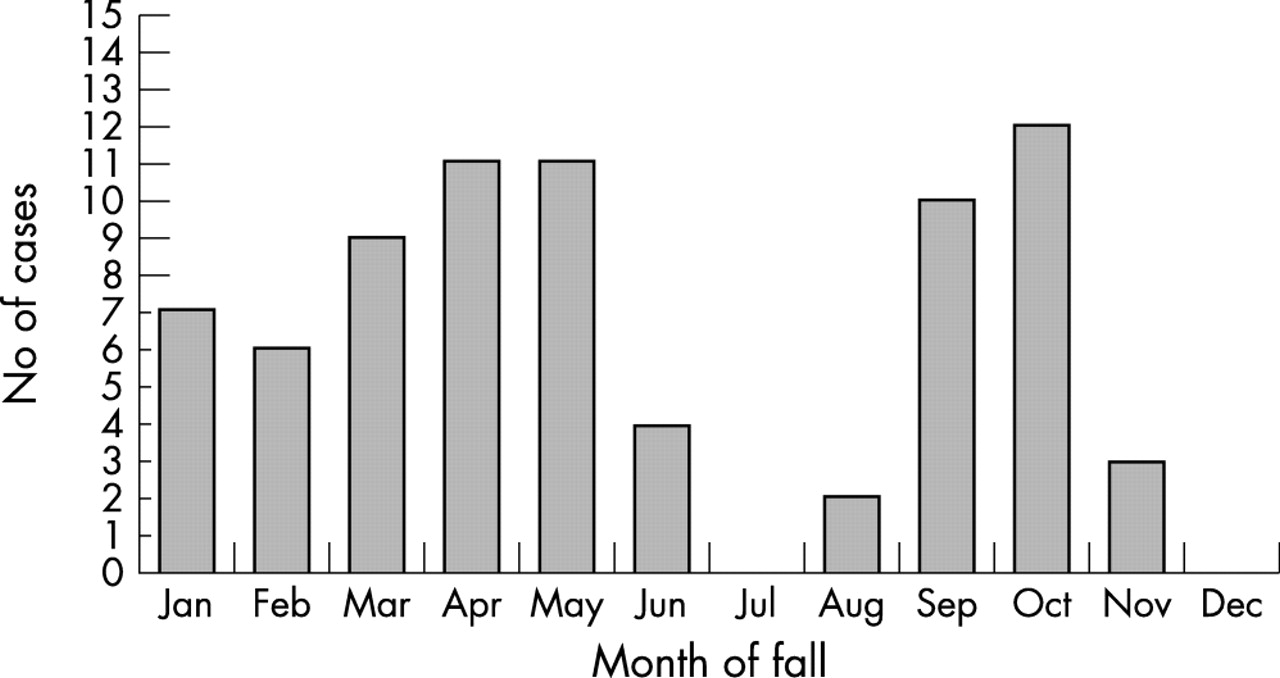
Cases of injuries due to falls from apartments, by month of occurrence, children 0–14 years, Dallas County, Texas, 1997–99.

{kind=link}
{kind=link}
Cases of injuries due to falls from apartments, by time of day, children 0–14 years, Dallas County, Texas, 1997–99.
For 39 (52%) of the cases, windows were the site from which the child fell. Balconies were the site from which 34 (45%) fell, and for two (3%), the site was unknown. Fifty six (75%) fell from a second floor height, 14 (19%) fell from a third floor, one (1%) fell from a fourth floor; for four (5%) the height of the fall was unknown.
Because windows and balconies were the sites of nearly all of the falls at apartments, we attempted to obtain more information about the circumstances of falls from these sites, with a telephone questionnaire to parents of injured children. We were able to complete questionnaires for 34 (45%) of the injured children, including 17 who fell from a balcony and 17 who fell from a window. To obtain further information about the balconies and windows involved in the fall, an inspection of the apartment was attempted, so that various measurements could be taken. These on-site inspections were accomplished for 13 of the balcony related falls and eight of the window related falls for which telephone questionnaires were completed. There was close agreement between information obtained from the telephone surveys and measurements (balcony rail distance, window distance from floor, etc) obtained during the on-site visits.
For 33 (97%) of the 34 injured children for whom the telephone questionnaire was completed, an adult was reported to have been supervising the child before the fall occurred. However, for 29 (85%), the supervising adult had been distracted before the fall occurred. Twenty five (74%) children were reported to have been playing at the time of the fall.
Balconies
There were 17 children who had fallen from a balcony and whose parents completed the telephone survey. For 13 children (76%), the falls occurred on common balconies, which were connected to other apartments; only four (24%) were private balconies, which were only accessible from the inside of the apartment. All children had fallen directly off the balcony onto the ground; none had fallen down stairs. For 11 falls (65%), the child had fallen between the rails of the balcony; in five (29%), the child had climbed over the rails, and for one the parent was unsure. In only one case did the railing have a missing slat. In 15 cases (88%), the rails were made of metal. On-site measurements were obtained for eight of the 11 actual balconies where children had fallen between the balcony rails; all had a distance of at least 5 inches (13 cm) between balcony rails (mean 7.5 inches, or 19 cm), and five of the eight were more that 7 inches (18 cm) apart. All eight of these apartments were built before 1984, when building code allowed balcony rail spacing of up to 9 inches (23 cm).
Windows
There were 17 children who had fallen from a window and whose parents completed a telephone survey. For 10 children (59%), the falls occurred from bedroom windows and seven (41%) occurred from living room windows. In all cases, the window was open at the time; for 13 (76%) a screen was present, but came off as the child fell. None had a window guard. For three (18%), the child fell from furniture on which the child had climbed, but for 13 (76%), the child fell directly out of a window which was situated low to the floor; this information was unknown for one child. In each case in which the child fell directly from the window (that is, without climbing onto furniture or an object), the window sill was situated 2 feet (61 cm) or less from the floor. On-site measurements were obtained for six of the 13 windows where children had fallen without climbing; the window sills ranged from 9–22 inches (23–56 cm) from the floor (mean 13 inches, or 33 cm).
DISCUSSION
A common pattern emerged from the analysis of apartment related falls among children in Dallas County. Most were preschool age boys who were engaged in play and were being supervised by an adult just before the fall. About half fell from a window and half from a balcony and most occurred around the noon or evening meal times. These findings were consistent with previous studies in other parts of the United States.1–10 These mealtime events may reflect a change in the level of supervision at these times, with family members more likely to be preoccupied with meal preparation then.
We found that most of the falls occurred in the spring or autumn seasons, whereas in previous reports, most had occurred in summer.2,4,7–11 This difference may be related to the weather in Dallas, with spring and autumn being mild and the seasons when people are more likely to leave windows open. By contrast, summer in our area is hot and there is almost universal use of air conditioning, with windows kept closed.
We were most surprised by two findings: most of the balcony related falls occurred as the child fell between the balcony rails, and most of the window related falls occurred from low lying windows. We had expected that most balcony related falls would have involved children climbing over or under the railings, but this was true in only a small proportion of the injuries. Most occurred when children fell between balcony rails, which were spaced an average of more than 7 inches (18 cm) apart, based on measurements from on-site visits of some of the apartments. Those apartments all were built before 1984, when the building code allowed balcony rail spacing of up to 9 inches (23 cm). Likewise, we had expected that most window related falls would have involved children climbing onto furniture (for example, beds, dressers, etc) or rolling off beds, but this was true only in a small proportion of injuries. Most of the falls occurred through windows that were within 2 feet (61 cm) of the floor, and the child fell from the floor through the window. Although most of the windows had screens, the screens were not sufficient to prevent the falls.
Two measures have potential to prevent most of these falls. For balconies, adherence to the currently recommended spacing of 4 inches (10 cm) or less could prevent almost any child from slipping between rails.12 For windows, since most of the falls were through low lying windows, either window guards3,11–13 or modification of the window to limit its opening or keep it closed, could prevent most of these falls. Alternatively, “child safety” window screens may provide protection against these falls.12 Current building codes in Dallas require that apartments built after November 1993 have balcony rails that are no more than 4 inches (10 cm) apart. However, there is no retroactive requirement for apartments built before 1993. Apartments built before 1984 were allowed to have balcony rails spaced up to 9 inches (23 cm), and before 1968 there was no code addressing rail spacing. To our knowledge, there is no requirement regarding placement of windows or the use of window guards in apartments in Dallas.
Several caveats are in order, with respect to the findings of this investigation. It is likely that the numbers and rates of injuries detailed in this survey underestimate the actual numbers of cases. We have no way of knowing how many children were seen in emergency departments in the Dallas area and not identified as injured due to a fall from a building, or for other reasons not reported to us, and thereby not included in the survey. It is also possible that less severely injured children were less likely to have been reported, which would have the effect of skewing the results toward the more severe injuries. We tried to minimize this effect by working with the Texas Department of Health for this investigation, but such effort does not guarantee reporting.14 In addition, we were able to contact only about 45% of parents of children who were seen in emergency departments for these injuries. In most cases, the telephone numbers were not functional, implying that the parent had either given incorrect information to the emergency department, or that they had moved from the apartment before we attempted to reach them. We do not know how this response rate might have influenced the results. And finally, we were able to visit the apartment of about two thirds of those for whom we completed telephone questionnaires for measurements to verify balcony rail distance and window height, etc. It is possible that the cases that we could not visit were different from those who were visited; however, the measurements obtained from the on-site visits were close to the estimates given by parents during the telephone surveys.
Nevertheless, among the cases where we had detailed information, 70% of the apartment fall related injuries among children may have been prevented by the two measures listed above. These measures would involve a one time modification of the environment. Such one time preventive interventions have been shown to be more effective in preventing injuries than those that require behavior changes or frequent implementation.15,16 If the findings from this investigation are confirmed through other studies, then more effort may be warranted to try to implement measures to prevent childhood falls at older apartments.
Key points
-
Previous studies have demonstrated the importance of childhood falls from windows in high rise apartment buildings, and the usefulness of window guards in this setting. However, there are no studies, to our knowledge, that have evaluated the circumstance of such falls in the setting of two and three story apartments, which are more common in parts of the United States outside of the northeast.
-
This report identified two sites as the source for most apartment related fall injuries: balconies in older apartments with rails spaced more than 4 inches (10 cm) apart and low lying windows.
-
Current building codes that require balcony rail spacing of no more than 4 inches (10 cm) do not apply to apartments in our area built before 1993; children who live in these apartments are at risk of fall related injuries.
-
One time environmental changes to these balcony rails and low lying windows could substantially reduce the number of these injuries.
Acknowledgments
We thank Carole Rush, RN for her help in coordinating the emergency department surveillance; Santiago Pedraza for his help with interviews and site visits; Dr Cub Culbertson, Dr Compton Broders, and the staff of participating emergency departments for assistance with surveillance; Allen Bolton, Dr Paul Boumbulian and Dr Dennis M Perrotta, for their advice and support throughout the project; Marcia Fries for her review of the manuscript; and Baylor Health Care System, Methodist Hospitals of Dallas, Presbyterian Hospital of Dallas, Children’s Medical Center of Dallas, Parkland Health and Hospital System, Texas Health Resources, and Texas Instruments for their ongoing support of the work of this project.