Article Text

Abstract
Background: The aim of the study was to describe the epidemiology of residential fire related deaths and injuries among children, and identify risk factors for these injuries through a linked dataset for the city of Dallas, Texas.
Methods: Data for all residential fires were linked with fire related injury data, using fire department records, ambulance transports, hospital admissions, and medical examiner records, for children 0–19 years of age. Causes of fires, including fireplay (children playing with fire or combustibles), arson and other causes, were determined by fire department investigation.
Results: From 1991–98, 76 children were injured in residential fires (39 deaths, 37 non-fatal). The highest rates occurred in the youngest children (<5 years) and in census tracts with lowest income. Fireplay accounted for 42% (32/76) of all injuries, 62% (15/24) of deaths in children 0–4 years, and 94% (13/14) of deaths from apartment and mobile home fires. Most of the fireplay related injuries (27/32, 84%) were from children playing with matches or lighters. Most started in a bedroom. Smoke alarms showed no protective efficacy in preventing deaths or injuries in fires started by fireplay or arson, but there was significant protective efficacy for a functional smoke alarm in fires started from all other causes (p<0.01).
Conclusions: Residential fire related injuries among children in Dallas occurred predominantly in the youngest ages (<5 years) and in poor neighborhoods. Most of the deaths, especially those in apartments and mobile homes, resulted from fireplay. Smoke alarms appeared to offer no protection against death or injury in fireplay associated fires, possibly from the nature of the child's behavior in these fires, or from the placement of the smoke alarm. Prevention of childhood residential fire related deaths may require interventions to prevent fireplay in order to be successful.
- residential fire
- burn
- fireplay
- epidemiology
- smoke alarm/detector
- CI, confidence interval
- OR, odds ratio
- residential fire
- burn
- fireplay
- epidemiology
- smoke alarm/detector
- CI, confidence interval
- OR, odds ratio
Statistics from Altmetric.com
Residential fires are a leading cause of unintentional injury deaths in children in the United States.1,2 Children playing with fire or combustible material (“fireplay”) account for about 5% of residential fires, but these fires are associated with a larger proportion of deaths.3,4 Nationally, fireplay accounts for about 40% of residential fire related deaths in children, but it may have a larger role in some subgroups or populations.5,6 We used a linked dataset of residential fires and related deaths and injuries in Dallas7 in order to review the role of fireplay in childhood fire deaths and injuries, with emphasis on possible prevention measures such as smoke alarms.
METHODS
Relevant datasets had been collected by four different agencies, and contained various information about residential fires and residential fire related injuries and deaths. Data from four sources were available for the years 1991–98: (1) emergency medical services for all ambulance transports in Dallas, (2) hospital admissions at Parkland Health and Hospital System, the only hospital with a burn unit in Dallas, (3) medical examiner reports of fatal injuries, and (4) Dallas Fire Department records of all residential fires in Dallas. The Dallas Fire Department data contained details about the nature of the fire, including information about the source and location of the fire, the age and type of structure, and the presence of a working or non-working smoke alarm. Smoke alarm status was determined by fire inspection specialists, based on interviews and inspection after the fire. Other datasets contained information about injured persons, and the nature of the injury. Medical examiner data included a narrative description about the event leading to death, for those injuries that were fatal.
An injured person was defined as any person who was: (1) transported by emergency medical services for a burn or smoke inhalation, or (2) admitted to Parkland Health and Hospital System for a burn or smoke inhalation, or (3) had been identified by the medical examiner as a death. In addition, the injury must have been related to a fire in a residential structure. Injuries that were not caused by flame, heat, or smoke (for example, falls, lacerations, etc) were not counted as fire related.
A house was defined as a non-mobile residential structure that contained one or two units (that is, single family structures and duplexes); an apartment had to contain three or more units. Mobile homes were defined as movable residential structures. Vacant structures were excluded.
Each case was linked to the record of the fire by matching the date, time, and location of the fire with the date, time, and site of the ambulance transport or death. Results of the overall review of fires and injuries have been previously reported.7 In this way, we developed a single dataset with all residential fires reported to the fire department, as well as information about persons who were injured or who died as a result of those fires. For the current study, we selected only those injuries that involved children <20 years of age, and the fires that resulted in those injuries.
We defined “fireplay” as any fire that was determined by fire inspection specialists to have been the result of children playing with fire or combustible material, which are coded as ignition factor 36 or 48, in accordance with the National Fire Incident Reporting System (NFIRS). For fireplay related fires, there was no information in the dataset about whether the injured person was the child who had started the fire. Arson was defined as any fire that was determined by fire inspection specialists to have been deliberately set by a person, but was not due to fireplay. The Dallas Fire Department coded the form of heat ignition with a code that combined matches and cigarette lighters in the same category; thus, those two sources could not be separated in the analysis.
Denominators for rate calculations (by age, ethnicity, etc) were taken from the 1990 census for Dallas, Texas. The population of Dallas in 1990 was 1 006 877; the number of children aged 0–19 years was 277 848. A breakdown of population by age, race, and ethnicity for Dallas was available through a special tabulation by the Bureau of Census.
Data were analyzed using Epi Info version 6.02b,8 from the Centers for Disease Control and Prevention. For most statistical calculations, rate ratios and odds ratios (OR) were used to estimate the relative risk, and 95% confidence intervals (CI) were calculated, as previously described.9–11 One way analysis of variance was tested using the Kruskal-Wallis test,12 and linear trend testing was performed using χ2 for trend.8 All reported p values are two sided.
RESULTS
Overview
From 1991–98, there were 13 676 residential fires in the city of Dallas. Fireplay was identified as the cause for 732 (5.4%), arson for 3325 (24.3%), and all other causes for 9619 (70.3%). A total of 401 persons were injured (140 deaths, 261 non-fatal injuries) in 321 fires; 76 (19 %) persons were under the age of 20 years.
Children
For the eight years of the study, 76 children age 0–19 years were injured in residential fires (average annual rate: 3.4 per 100 000 persons age 0–19 years); 39 died as a result of the injury, and 37 had a non-fatal injury. Injuries peaked in 2 and 3 year olds (fig 1). More than half (40/76) of the injuries, and 61% of the deaths (24/39), occurred in children age 0–4 years, for whom the average annual rate was 6.2 per 100 000 population. This was twice the rate of 5–9 year olds, and four times the rate for children 10 or more years of age (table 1). The average annual rate of residential fire related injuries was higher in children who were black (5.4 per 100 000), Hispanic (3.1 per 100 000), or other races (3.2 per 100 000), compared with children who were white (1.2 per 100 000) (table 1). Although the injury rate was higher for children who lived in mobile homes and apartments compared with houses, this difference was not statistically significant.
Childhood residential fire related injuries, injury rates, and number due to fireplay, by various characteristics, Dallas, Texas, 1991–98
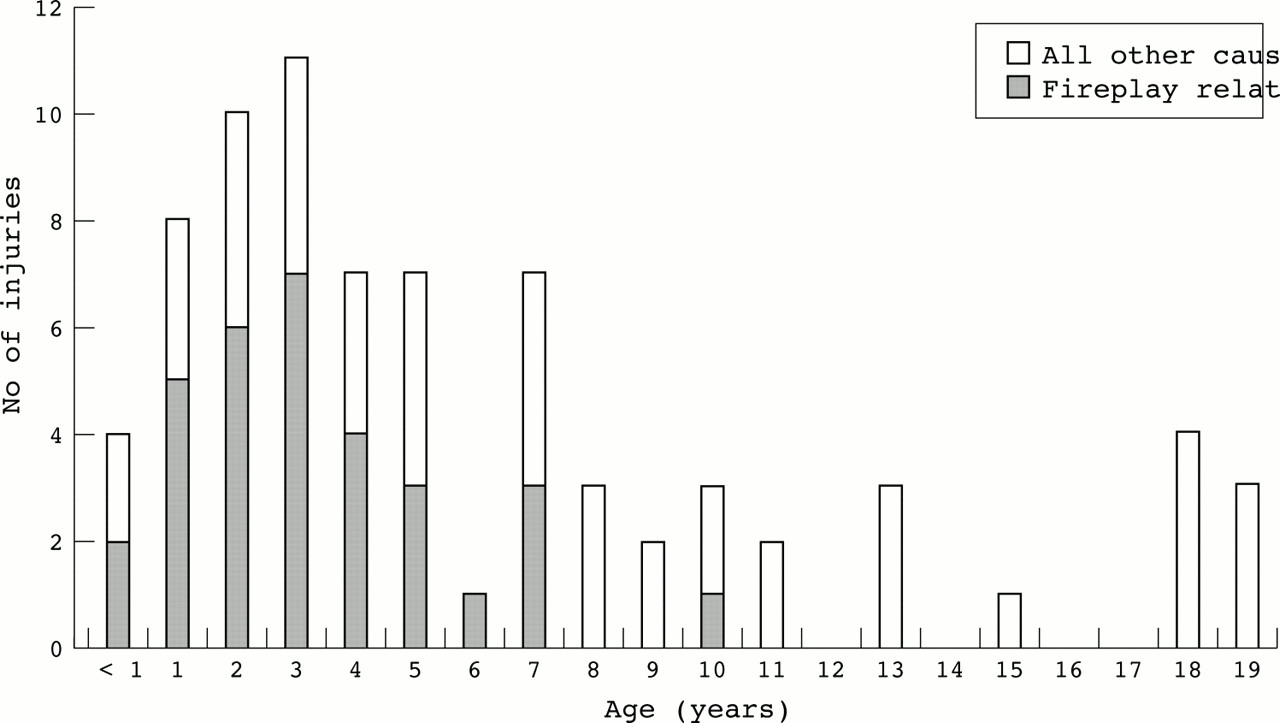
Residential fire related injuries in children, by age and fireplay status, Dallas, Texas, 1991–98.
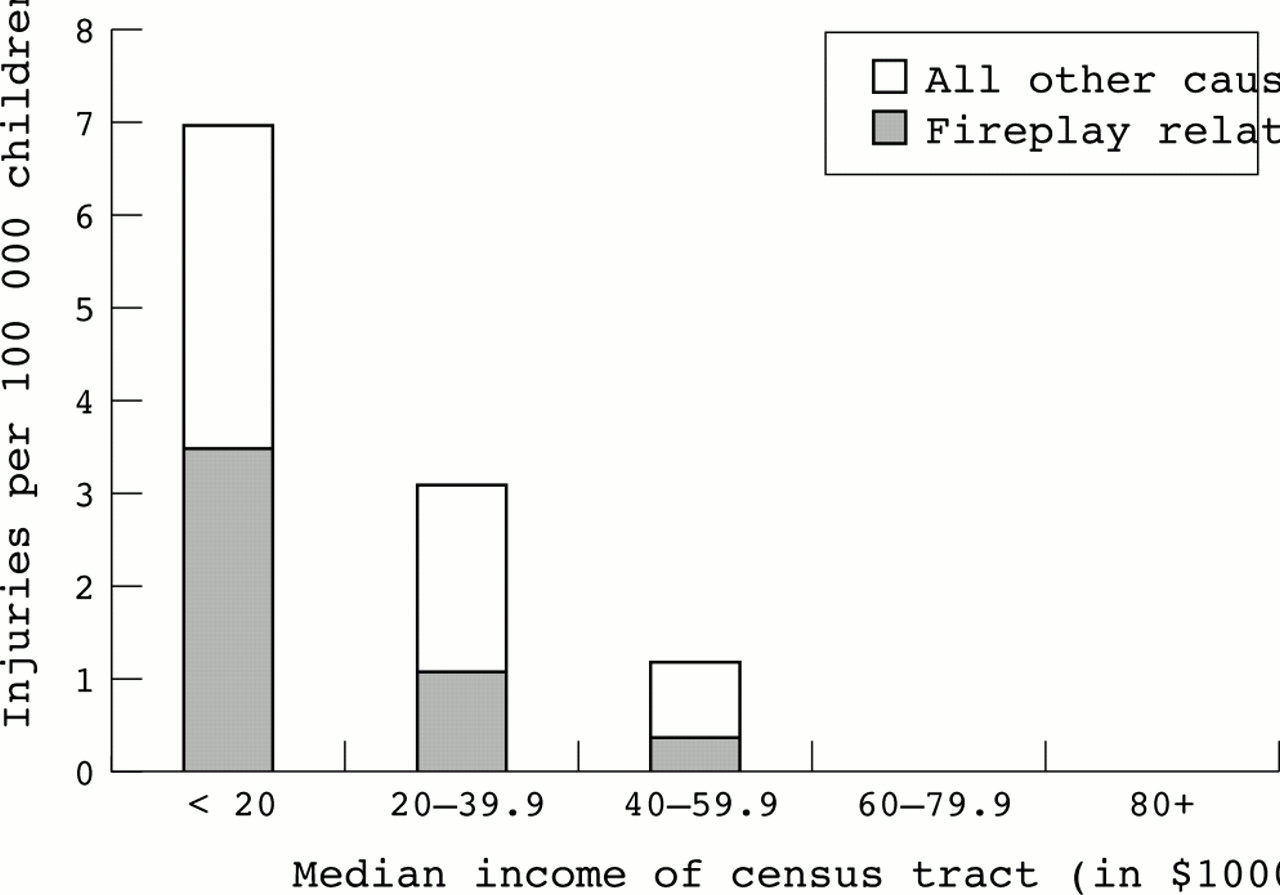
There was a marked gradient in the rate of residential fire related injuries by median income of census tract. For the lowest income census tract group (<$20 000 median income), the average annual childhood injury rate was 7.0, compared with 3.1, 1.2, 0, and 0 for each successively higher median income grouping (fig 2; p<0.01 by χ2 for trend).

{kind=link}
{kind=link}
Annual rate of residential fire related injuries in children 0–19 years of age, by median income of census tract and cause of fire, Dallas, Texas, 1991–98.
Fireplay
Among children, fireplay accounted for 42% (32/76) of the injuries, arson associated fires accounted for six (8%) injuries, and fires from all other causes accounted for 38 injuries (50%). Fireplay associated injuries were more common among younger children (0–4 years), for whom it accounted for 60% (24/40) of injuries (table 1). The proportion of injuries due to fireplay decreased with age (p<0.01, χ2 for trend). In addition, a larger proportion of injuries to children in apartment fires (21/31) or mobile home fires (3/4) were due to fireplay, than for injuries from house fires (8/41) (p<0.001). In fact, 94% (13/14) of childhood deaths in apartment and mobile home fires were due to fireplay. Most of the fireplay related injuries (27/32, 84%) were from children playing with matches or lighters.
From the overall dataset of residential fires, it was apparent that fireplay associated fires were more likely to result in injuries (6.7 per 100 fires) than fires due to arson (1.7 per 100 fires) or fires due to all other causes (3.1 per 100 fires) (p<0.01 by Kruskal-Wallis one way analysis of variance) (table 2). In addition, the proportion of injured persons who were children (<20 years) was highest for fireplay associated fires (32 of 49, 65%) compared with arson related (six of 57, 11%) or fires of other causes (38 of 295, 13%) (OR 13.2, 95% CI 6.4 to 27.2, p<0.001, for fireplay v non-fireplay). Furthermore, fireplay associated fires were more likely to have started in a bedroom (52% v 21% and 16%, for fireplay v arson and all other causes; p<0.001) and to have begun between 8:00 am and 8:00 pm (79% v 45% and 60% for fireplay v arson and all other causes; p<0.001).
Residential fire related injuries by smoke alarm (SA) status and by cause of fire, Dallas, Texas, 1991–98
Smoke alarms
Smoke alarm status was known for 68 (89.5%) of the 76 children who were injured in residential fires. Smoke alarms showed no protective efficacy in preventing deaths among children injured in fires started by fireplay or arson. For this analysis, the smoke alarm status of the fires in which children died was compared with the smoke alarm status of the fires in which children were non-fatally injured. If smoke alarms were effective in preventing deaths, one would expect that children who had a non-fatal injury in a fire would have been more likely to have a functional smoke alarm in the residence than children who died. This was not true for fireplay associated or arson associated deaths and injuries. Among fireplay associated non-fatal injuries, none of 11 had a functional smoke alarm in the residence; among fireplay associated deaths, six of 18 (33%) had a functional smoke alarm (OR indeterminate; 95% CI 0.8 to indeterminate; p = 0.057). Among arson associated non-fatal injuries, none of three had a functional smoke alarm; among arson associated deaths, one of two had a functional smoke alarm (OR indeterminate; 95% CI 0.1 to indeterminate; p = 0.4). However, there was significant protective effect for a functional smoke alarm in fires started from all other causes (that is, non-fireplay, non-arson): seven of 16 (44%) non-fatally injured children had a working smoke alarm, but only one of 18 (6%) of deaths had a working smoke alarm (OR 0.1; 95% CI 0.0 to 0.8; p = 0.02).
For the entire dataset of residential fires, similar results were found for the analysis of smoke alarm efficacy. Information about smoke alarm function was determined for 661 (90%) of the 732 fireplay associated residential fires, 2512 (76%) of the 3325 arson associated fires, and 8595 (89%) of the 9619 fires of all other causes. For this analysis, we compared the proportion of fires that resulted in at least one injury or death, for fires with a functional smoke alarm versus fires without a functional smoke alarm. If smoke alarms were effective in preventing injuries (fatal or non-fatal), then one would expect that fires that occurred in the presence of a functional smoke alarm would be less likely to result in an injury or death than fires that occurred without a functional smoke alarm. For fires associated with fireplay or arson, there was no difference in the proportion of fires that resulted in injury or death, with regard to the presence or absence of a functional smoke alarm, indicating no effect of smoke alarms (table 2, p = NS). However, for fires associated with all other causes, smoke alarms showed significant protection, with fires in the presence of a functional smoke alarm having a significantly lower proportion that resulted in an injury or death than fires without a functional smoke alarm (OR 0.6; 95% CI 0.4 to 0.8; p<0.01) (table 2).
To further evaluate the efficacy of smoke alarms, we calculated the number of injuries per 100 fires for those fires with a working smoke alarm compared with those fires without a working smoke alarm. For fires associated with fireplay or arson, there was no difference in the rate of injuries per 100 fires where a working smoke alarm was present, compared with fires without a working smoke alarm. However, for fires associated with all other causes (that is, non-fireplay, non-arson), there were significantly fewer injuries in fires where there was a working smoke alarm compared with fires where there was no working smoke alarm (2.1 v 3.3 injuries per 100 fires; p = 0.02 by Kruskal-Wallis one way analysis of variance; rate ratio 0.6; 95% CI 0.4 to 0.9) (table 2).
DISCUSSION
While fireplay is a relatively small part of the overall fire problem in the United States, it looms as the predominant cause of residential fire related injuries and deaths among young children.13 In the present study, fireplay accounted for most of the injuries and almost all of the deaths from apartment and mobile home fires among children in Dallas, and occurred disproportionately among the poor. Our data could not distinguish whether the injured child was the same child who started the fire, but others have found that as many as two thirds of the victims of fireplay related fires were not the children who were playing with fire.13–15 Nevertheless, other studies have shown that the majority of children involved in fireplay in these settings were under age 6 years.13,14 In addition, our study found that fireplay associated fires and injuries were more likely to have begun in a bedroom and to have started between the hours of 8:00 am and 8:00 pm.
Almost all of the fireplay associated fires and injuries in the present study were due to children playing with matches or lighters. Our data could not distinguish between these different sources. Hall also found that more than 80% of injuries in fireplay associated fires were due to lighters or matches.13 Nationally, the number of injuries from these fires has decreased since the adoption of a child resistant lighter standard by the Consumer Product Safety Commission, which went into effect in 1994,13,14 but the present study did not find any decrease in fireplay related fires or injuries in Dallas from 1991–98 (data not shown).
We could find no evidence of protective efficacy for smoke alarms for those children who were injured in fires caused by fireplay or arson, whereas smoke alarms appeared to offer significant protection against death from fires started from other causes. This finding was consistent across three different analyses in the current study. Reasons for this lack of efficacy of smoke alarms in fireplay related fires may be due to a number of factors, including the location of the fire, the rapidity of spread, the placement of smoke alarms, the behavior of the child after the fire starts, and the lack of supervision associated with fireplay.4–6,13,16 To our knowledge, only one previous study has evaluated the issue of smoke alarm effectiveness in fireplay associated fires.14 It found a trend toward efficacy, with more deaths and injuries in fires that had no functional smoke alarm.14
IMPLICATIONS FOR PREVENTION
The fact that fireplay associated fires were most likely to begin in a bedroom probably reflects where children played with matches or lighters. If a child did so with a bedroom door closed, then a smoke alarm that was located outside of a bedroom (for example, in a hallway), may not have sounded in time to prevent death. We could not determine the exact placement of the smoke alarm from our dataset. This may be important information in explaining the lack of efficacy of smoke alarms in the current study. The finding may have represented ineffective placement, rather than lack of efficacy of the alarm itself. If this finding is confirmed in other studies, it would reinforce the recommendation to place smoke alarms inside bedrooms,17 especially bedrooms where children sleep.
Key points
-
Preschool age and minority children living in low income census tracts had highest rates of residential fire related injuries.
-
Fireplay accounted for most of the injuries in the youngest children, and for almost all of the deaths among children in apartment and mobile home fires.
-
Most fireplay associated fires were started by children playing with matches or lighters in bedrooms.
-
In this study, smoke alarms appeared to have no protective effect in fires started by fireplay.
-
Preventive measures probably will need to include measures other than smoke alarms
-
A linked dataset of fires, deaths, and injuries was effective in describing the epidemiology of residential fire related injuries.
Smoke alarms were clearly effective in preventing deaths and injuries from residential fires due to all causes other than arson or fireplay. The finding that smoke alarms are not sufficient to prevent fireplay related deaths and injuries, if confirmed, indicates that prevention of this subset of childhood deaths will be difficult, and will require much more than a smoke alarm installation program. Possible means of preventing fireplay related injuries include educational programs aimed at children and parents to decrease access by children to flame sources,13 implementation of childproof lighters and matches,2,4,13,14 and labeling of matches.13 It is clear from the data from the current study and others2,4,13,14 that programs to prevent fireplay related injuries must be oriented toward the preschool age population and their families.
The data from this study of residential fire related injuries among children in Dallas reinforces the importance of fireplay as the predominant cause of these injuries, especially among preschool children and among children who are injured in apartment and mobile home fires. Since smoke alarms appear to be ineffective in preventing deaths in these circumstances, other means of preventing fireplay and its resulting injuries need to be developed and implemented.
Acknowledgments
We are indebted to Don Myatt and Vivian Zheng of Emergency Medical Services; Jeffrey Barnard, MD, and Bill Lene of the Dallas County Medical Examiners Office; Peggy Kacka, and Kim McCloud, RN, of Parkland Health and Hospital System; John Hunt, MD, Gary Purdue, MD, and James Carrico of UT Southwestern Medical Center; Bob O'Brien, Linda Osborn, Joe Pierce, and the firefighters and staff of the Education and Inspection Division of the Dallas Fire Department; and the staff of the Texas State Fire Marshall's Office, all of whom provided assistance with data and support for the project. We also thank the many workers and volunteers of the Dallas Chapter of the American Red Cross for their ongoing support of Operation Installation and support of families involved in house fires. We are indebted to Ron Anderson, MD, and Paul Boumbulian, DPA, of Parkland Health and Hospital System, and Martha Stowe, MSW, director, and Allen Bolton, MPH, former director of the Injury Prevention Center of Greater Dallas, for their advice and support throughout the project; to Kristen Howell, LMSW, for her review and suggestions on the manuscript; and to Baylor Health Care System, Methodist Hospitals of Dallas, Presbyterian Hospital of Dallas, Children's Medical Center of Dallas, Texas Health Resources, and Texas Instruments for their ongoing support of the work of this project.