Article Text

Abstract
Objective: To analyse the role of individual and contextual variables in injury mortality inequalities from a small area analysis perspective, looking at the data for the city of Barcelona (Spain) for 1992–98.
Setting: Barcelona (Spain).
Methods: All injury deaths in residents older than 19, which occurred in the period 1992–98 were included (n=4393). Age and sex specific mortality rates were calculated for each educational level and each cause of death (traffic injuries, falls, drug overdose, suicide, other injuries). The contextual variables included were the proportion of men unemployed, and the proportion of men in jail, in each neighbourhood. Multilevel Poisson regression models were fitted using data grouped by age, educational level, and neighbourhood for each sex.
Results: Death rates were higher in males, at the extremes of the age distribution (under 44 and over 74 years), and for lower educational levels. The results of the Poisson multilevel models indicate that inequalities by educational level follow a gradient, with higher risks for the population with no schooling, after having adjusted for the contextual variables of the neighbourhood. Such inequalities were more important in the youngest age group (20–34 years), as relative risk of 5.41 (95% confidence interval (CI) 3.9 to 7.4) for all injury causes in males and 4.38 (95% CI 2.3 to 8.4) in females. The highest relative risks were found for drug overdose. There was a contextual neighbourhood effect (the higher the deprivation, the higher the mortality) after having taken into account individual variables.
Conclusion: The findings underscore the need to implement injury prevention strategies not only at the individual level taking into account socioeconomic position, but also at the neighbourhood level.
- injury mortality
- socioeconomic position
- small area analysis
- contextual variables
- multilevel modelling
- CI, confidence interval
- ICD-9, International Classification of Diseases, ninth revision
- RR, relative risk
- injury mortality
- socioeconomic position
- small area analysis
- contextual variables
- multilevel modelling
- CI, confidence interval
- ICD-9, International Classification of Diseases, ninth revision
- RR, relative risk
Statistics from Altmetric.com
- injury mortality
- socioeconomic position
- small area analysis
- contextual variables
- multilevel modelling
- CI, confidence interval
- ICD-9, International Classification of Diseases, ninth revision
- RR, relative risk
- injury mortality
- socioeconomic position
- small area analysis
- contextual variables
- multilevel modelling
- CI, confidence interval
- ICD-9, International Classification of Diseases, ninth revision
- RR, relative risk
Although the study of social inequalities in health has been broadened since the 1980s, inequalities in injuries have been studied somewhat less,1 and most studies focus on children and the young. These show the existence of socioeconomic inequalities in injury mortality and morbidity, with the less privileged classes consistently showing higher injury rates.2–11
The study of social inequalities in health is not widespread in southern European countries, including Spain. Studies based on individuals are few due to the absence, or poor quality, of information on socioeconomic position in death certificates.12 Barcelona has a mortality register linked with the municipal census. This provides an opportunity to obtain the educational level of the deceased and therefore to study mortality inequalities by educational level.13,14
Urban areas often show important inequalities in health since some neighbourhoods have marginal populations.15 Recent research, using multilevel modelling, has emphasised the role of the residential environment: socioeconomic or deprivation characteristics of the neighbourhood influences health, independently of the socioeconomic position of its individuals.16–18 Nevertheless, to our knowledge, only a few studies have focused on inequalities in injuries taking into account individual as well as contextual variables, all finding independent contextual effects.19,20
The objective of our study was to analyse the role of individual and contextual variables in injury mortality socioeconomic inequalities from a small area analysis perspective, looking at the data for Barcelona for the period 1992–98.
METHODS
Design and study population
Barcelona, the second largest Spanish city (1 600 000 inhabitants), is located on the north eastern coast. The study used a cross sectional design, including all Barcelona residents older than 19, the age of completion of secondary studies. All deaths due to injuries, which occurred among these residents between 1992 and 1998, were included: traffic injuries (codes E810–829, International Classification of Diseases, ninth revision (ICD-9)21), falls (E880–888), drug overdose (E850–858), suicide (E950–959), other injuries (all other ICD-9 E codes), and all injuries (E800–999). In the group of other injuries, the most frequent causes were: injuries by foreign bodies (27%), surgical or medical complications (8.5%), homicides (8.4%), drowning (5.8%), and fire (5.1%).
Information on the population at risk, including age, sex, the highest completed level of education, and neighbourhood of residence comes from the 1996 municipal census. This census is continually updated to incorporate data on migration, births, and deaths. The educational level and neighbourhood of the deceased were obtained through an exact record linkage between the death register and the municipal census, based on the name, surname, and date of birth of the deceased. Educational level was successfully retrieved for 87.1% of the fatalities and neighbourhood for 97.6 %.
Variables and indicators analysed
The individual variables studied were age, sex, neighbourhood of residence, and highest completed level of studies (educational level). Educational level was categorised as: illiterate, no education and with 0–4 years of schooling (no schooling), primary studies (5–11 years of schooling), and secondary or higher studies (≥12 years). For rate estimation, age was grouped: 20–24, 25–34, 35–44, 45–54, 55–64, 65–74, ≥75, although for the multilevel models age was grouped into broader categories (following the pattern of age specific rates): 20–34, 35–74 and ≥75, and 20–34 and 35–49 for drug overdose related deaths.
Barcelona has 38 neighbourhoods, their populations varying between 1081 and 95 382 inhabitants (mean 39 705). As contextual variables to measure deprivation of the neighbourhood, we included the percentage of unemployed men, obtained through the municipal census of 1991, and the proportion of men in jail, defined as the proportion over 21 who had been in preventive jail per 100 000 inhabitants in 1995 (pre-trial admissions). We chose these indicators because they have been used before in ecological studies in Barcelona and have been related with health outcomes at an ecological level.22,23
Data analysis
Age and sex specific mortality rates were calculated for each educational level and each cause of death. Age standardised rates, standardised through the direct method, were estimated for each neighbourhood, using the 1996 population as the reference population.
Multilevel models allow the simultaneous examination of the effects of group level and individual level variables on individual level outcomes.24 Multilevel Poisson regression models were fitted using data grouped by age, educational level, and neighbourhood for each sex using the hierarchical linear and non-linear modelling statistical program25 and modelling a two level structure of individuals within neighbourhoods. The effect of the educational level was separated by age group because of the interactions observed in age specific death rates. Models were obtained for males and females.
These models estimate the relationship between individual (age and educational level) and neighbourhood variables and injury mortality. The steps in the construction of the models were: (1) study the differences in mortality rates among neighbourhoods (a multilevel model with only a random parameter and a constant); (2) include individual variables (age and educational level); and (3) include unemployment and/or the proportion of men in jail for the neighbourhood.
RESULTS
Description of the population
This study included 2763 injury deaths in men and 1630 in women (table 1). In men, the majority of injury deaths involved young people (under 44 years), most often due to traffic injuries and to drug overdose. In women, the majority of deaths were among the elderly population (≥75 years old), mostly due to falls. Male unemployment in the neighbourhoods ranged from 8% to 22.9% and the proportion of men in jail ranged from 24.9 to 1679.9 per 100 000 men older than 21 years.
Number of injury deaths and percentage by age, underlying cause of death, and educational level; Barcelona 1992–98
Mortality rates
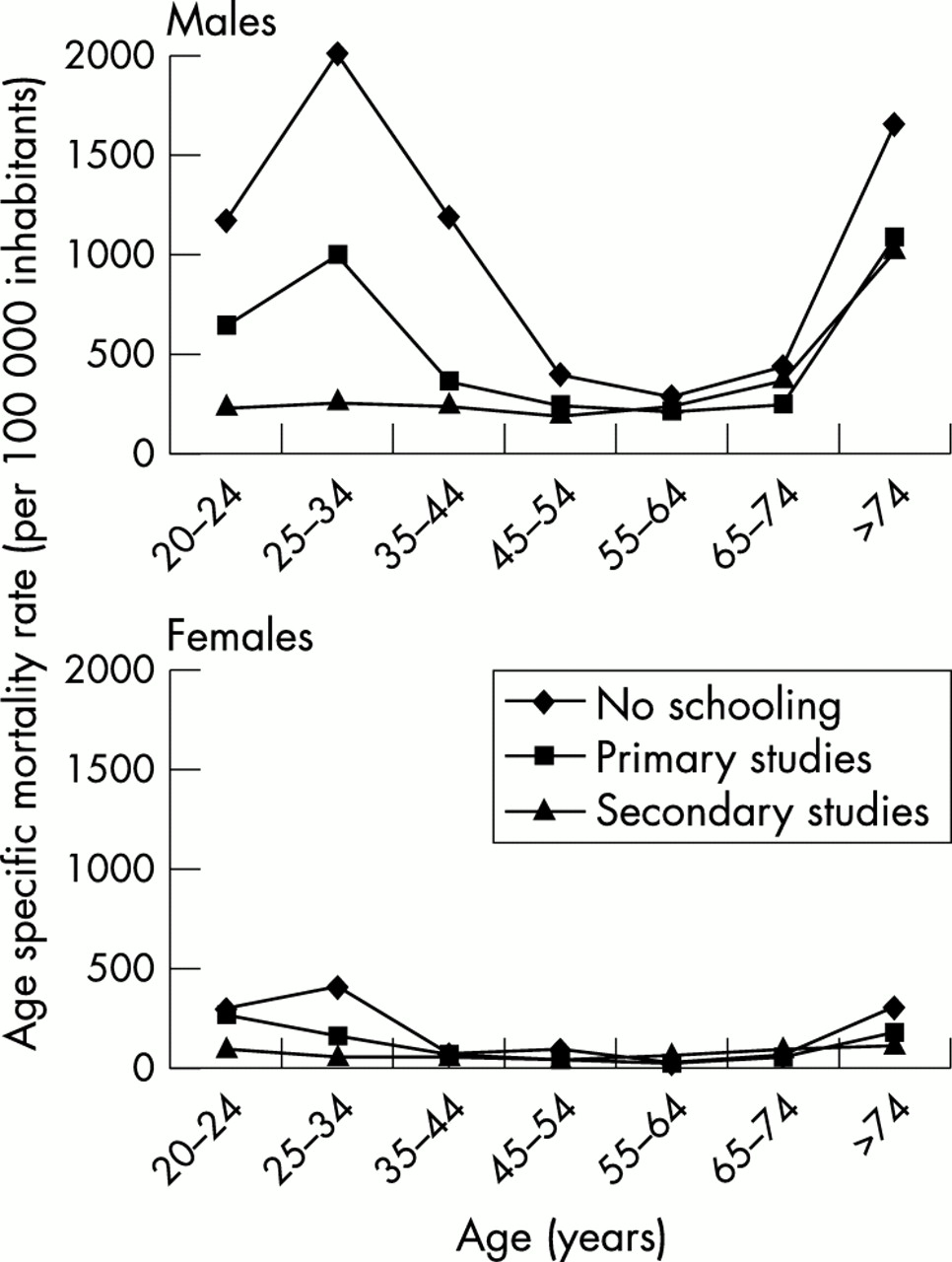
As shown in fig 1, death rates were higher in males at the extremes of the age distribution (under 44 and over 74 years), and for lower educational levels. For example, in males aged 25–34 death rates were 2016.7 per 100 000 inhabitants in the population with no schooling, 1003.6 in those with only primary education, and 270.7 in the more educated group. For females, the corresponding rates were 417.2, 170.2, and 64.0, respectively. In both sexes, inequalities by educational level decreased in the intermediate age categories.
{kind=link}
Age specific mortality rates due to injuries (per 100 000 inhabitants) by educational level; males and females, Barcelona 1992–98.
The distribution for the main causes of injury death in males and females shows an inverse relationship between educational level and injury mortality. This relationship seems to be more important in the younger ages than in the elderly. The distribution by age group changed by cause of death: traffic injuries were more important under 35 and at older ages, while falls and other injuries increased importantly at older ages; drug overdose mortality was important mainly in the young population, while suicide mortality showed a less characteristic age profile. Men had higher rates of traffic injuries and drug overdose.
Neighbourhood injury mortality increases with increased male unemployment. This relation is maintained for mortality due to falls and drug overdose in both sexes and for suicide in men, although this is not the case for traffic crashes and suicide in women.
Multilevel models
The results of the Poisson multilevel models are presented in table 2. Inequalities in injury mortality by educational level follow a gradient, with higher risks for the population with no schooling, after having adjusted for the contextual variables. In the following three paragraphs we present the results by age group, and for each age group for the different educational levels.
Multilevel association among educational level and injury mortality (Poisson regression), individual and neighborhood effects by cause of death and age group; Barcelona 1992–98
Inequalities were more important in the youngest age group (20–34 years), as shown by the relative risk (RR) of the population with no schooling of 5.41 (95% confidence interval (CI) 3.9 to 7.4) for all injury causes in males and 4.38 (95% CI 2.3 to 8.4) in females. The highest RRs were found for drug overdose (RR 11.7, 95% CI 7.2 to 19.0 in men and RR 4.5, 95% CI 1.3 to 15.4 in women). Traffic injuries, falls, and suicides also had higher RRs at lower educational levels. In this age group, the RR of the population with primary studies was 3.17 (95% CI 2.7 to 3.7) in males and 2.48 (95% CI 1.9 to 3.3) in females for all injuries. The highest RR was for drug overdose and falls in males and for drug overdose and traffic injuries in females.
The second age group was 35–74 (35–49 for drug overdose). For all causes of injury mortality, the RR of the population with no schooling was similar for both sexes. In this age group RR were statistically significant for drug overdose and suicide in males and for falls in females. The RR for the population with primary studies was only significant for drug overdose in males.
Relative risks in the ≥75 age group were smaller, with the exception of suicide. It is noteworthy that RRs in traffic injuries in women were in the opposite direction (RR 0.47, 95% CI 0.25 to 0.87 for the population with no schooling and RR 0.37, 95% CI 0.19 to 0.71 for the population with primary studies).
Even after controlling for individual educational level, the percentage of neighbourhood unemployment was statistically significant for falls and total injury deaths, and the proportion of men in jail was statistically significant for drug overdose, pointing to a contextual neighbourhood effect (the higher the deprivation, the higher the mortality) after having taken into account all variables included in the model. For example, the RR of unemployment in death for falls was 1.05 in males and 1.03 in females, implying that for each point of increase in the unemployment percentage, the death rate increases 5% in males and 3% in females. No such relationship was observed for traffic injuries or suicides.
DISCUSSION
Main findings
Inequalities in injury mortality by educational level follow a gradient, with highest risks for those with no schooling. Such inequalities were more important in the youngest age group and in men. Due to the higher rates in males, the rate difference (attributable risks) of educational level was much higher in men, although RR was similar in both sexes. For example, in the 25–34 age group it was 1746 deaths per 100 000 inhabitants for the population with no schooling in men and 353.2 in women. The same pattern applied to other age groups. The higher rates in men may be due to differences in exposure to traffic and drug use.
This study also shows, for the first time in the European context, that besides individual factors, contextual effects independently influence the unequal social distribution of injury mortality. For Barcelona, we show that when using a multilevel analysis approach in a small area urban context there is a neighbourhood effect, besides individual educational level, explained by deprivation.
We tried to include two indicators related to material and social deprivation. Unemployment has been used as an indicator of material deprivation because it reflects lack of income and insecurity.26 The proportion of men in jail has been used before in Barcelona as a social deprivation indicator23 because it may reflect isolation or exclusion. Therefore, material deprivation would be related with mortality due to falls and total injury mortality and social deprivation to drug overdose. Conversely, although social inequalities are also present in traffic injuries and suicide mortality, no contextual effects seem to influence this distribution, probably because inequalities by such causes of death among neighbourhoods were better explained by individual characteristics.
Some results regarding overall inequalities in injuries are consistent with previous reports. For example, traffic injuries have been related to individual educational level or occupational social class mainly during childhood and youth.3,5,7,19,27 These injuries include all drivers (cycle, moped, motorcycle, and car) and pedestrians. The data available in the present study do not allow us to determine whether such inequalities reflect differences in exposure to traffic, in type of vehicle involved, in injury severity, or in use of protective devices. In fact, several of these factors could explain some of the differences found: people with a low educational level may own older vehicles, use protective devices less often, or drive at higher speeds. On the other hand, the observation of no neighbourhood effect for traffic injury mortality could be related to the fact that mobility gained through the use of a vehicle may result in people being involved in crashes occurring outside the neighbourhood of residence. Other studies have found that persons living in urban areas are at decreased risk of motor vehicle mortality than those living in rural areas, reflecting decreased exposure to traffic.19,28
In our study, mortality due to falls was related to educational level, mainly in the young population. We have not found any other studies that analyse falls separately from other unintentional injuries or other external causes1; thus we have nothing with which to compare our results. Also, deprivation of the neighbourhood has been associated with mortality. Possible explanations of the relation between socioeconomic status and unintentional injuries are material resources, such as decent housing.1 From our point of view, differences among neighbourhoods of Barcelona, related to material deprivation such as the physical environment, including the quality of the houses as well as of public spaces, could explain the contextual influence found.
As regards drug abuse, Barcelona has a high prevalence of heroin users29 and drug overdose was one of the main causes of death in the 15–34 age group in the previous decade.30 In this study we found inequalities by educational level and also that neighbourhood variability was explained by the proportion of men in jail, after having taken into account individual educational level. Other studies in Barcelona have described individual as well as neighbourhood socioeconomic inequalities in drug overdose mortality.13,22,31 Authors from Europe and the United States have also found relationships between social disintegration, social disorganisation, substance abuse, and crime.32,33
Finally, the findings regarding inequalities in suicide mortality at an individual level and mostly in men are consistent with other reports,5,34 although some did not find this relationship.7,19 Cubbin and Smith also report mixed results in their review.1 We did not find a neighbourhood influence on suicide mortality. Ecological studies have found a relationship between the deprivation of the area (using Townsend and Carstairs deprivation scores) and suicide,35,36 but the design used (ecological) is not comparable with ours (multilevel analysis). Suicide rates and type of suicide vary across countries and among different socioeconomic groups in particular countries, which may reflect the existence of different social, cultural, and psychological factors.1,37,38
The higher RR for death among persons in disadvantaged social classes at younger ages has also been reported previously.39,40 Various explanations have been offered, from the survival advantage of the privileged social classes becoming a mortality disadvantage at older ages,39,40 to the fact that illiteracy denotes a worse socioeconomic situation in young people than in older people, since nowadays access to basic education is far greater.41
Key points
-
Inequalities in injury mortality by educational level follow a gradient, with highest risks for those with no schooling. Such inequalities were more important in the youngest age group and in men.
-
Besides individual factors, contextual effects independently influence the unequal social distribution of injury mortality.
-
The existence of these social inequalities in injury mortality underscore the need to tailor injury prevention strategies to the socioeconomic position of the population they are aiming to protect and also to focus them at the neighbourhood level.
-
Such efforts could be strengthened if an equity dimension was added within the Haddon matrix approach for interventions directed to traffic injuries.
Limitations
Although one of the potential limitations of this study could have been the under-reporting of drug overdose29,42,43 or suicide,44 in Barcelona, this is not the case since external causes of death include forensic data.42,45 In a study on improvement of the quality and comparability of causes-of-death statistics in the European Union, suicide, unintentional deaths, and drug related deaths were considered as causes of death requiring special attention.46 Another limitation is the measure of the socioeconomic position used (educational level) because we were not able to include social class based on occupation.12 Several limitations of educational level are: first, its inability to refer to social groups arising from interdependent economic relationships; second, it is less predictive than class position of ownership of capital assets; and third, it does not have a universal meaning because its implications are related to age, gender, race, birth cohort, and class position.47
Death cases that had the educational level missing were younger and more frequently died of traffic injuries or drug overdose. We do not know if missing data were related to educational level but recognise that this could introduce a small bias in our results. Nevertheless, the associations found were too strong to be explained by such a bias.
RECOMMENDATIONS AND CONCLUSION
The existence of social inequalities in injury mortality both at the individual and contextual levels, underscore the need to implement injury prevention strategies not only at the individual level, but also to tailor them to the socioeconomic position of the population they are aiming to protect. It would also be necessary for injury prevention actions to be focused at the neighbourhood level, to modify adverse environmental conditions of deprived areas, such as urban renovations, improved, and public spaces, as well as reinforcing social networks in deprived communities. Such efforts could be strengthened if, as has been recently suggested, an equity dimension was added within the Haddon matrix approach for interventions directed to traffic injuries. This modification could also be extended in support of prevention policies for a wider number of injury causes.48,49
Acknowledgments
Our thanks to Ana Diez-Roux for her help in multilevel modelling, and to the editor and the three reviewers for their suggestions. This study was done with the support of grant 99/0977 of the Fondo de Investigaciones Sanitarias.
REFERENCES
Linked Articles
- Correction