Article Text

Abstract
Background—It is argued that use of the term “accident” has a negative effect on prevention efforts as the term implies that such events are due to chance.
Aim—To test the hypothesis that use of “injury” in place of “accident” can influence professional attitudes towards “accident/injury” prevention.
Setting—Leeds Health Authority area serving the population (n=740 000) of the city of Leeds in the Yorkshire region of England.
Method—A randomised comparative study. Altogether 183 health visiting staff in the Leeds area were randomised (by place of work) to one of two groups. Each group received a similar postal questionnaire assessing attitudes relating to accident/injury prevention. One group received a questionnaire using only accident terminology while the other used injury terminology throughout.
Results—Fifty responses in the accident group were received and 39 in the injury group. Analysis by Mann-Whitney U tests showed little difference in group responses. The only significant finding was that respondents in the “accident” group were more likely to rank “accident prevention” of higher importance relative to respondents in the “injury” group (median 2, 25%–75% quartiles 1.8–4.0 compared with median 4, 25%–75% quartiles 2.0–5.0, p=0.04). However, this may have been a chance finding due to the multiple comparisons made.
Conclusions—This study has shown little difference in health visitor responses when “accident” is replaced with “injury”. It is possible that the effect of changing terminology is more nebulous—influencing society at large. However, it would be as well to recognise the lack of evidence and clarity relating to the terminology debate. Otherwise, there is a danger that the “injury” believers may become alienated from the “accident” diehards.
- terminology
- professional attitudes
Statistics from Altmetric.com
For many in “injury prevention” circles, the use of the term “accident” has become unacceptable. Arguments against using “accident” are that the term implies that such events are unpredictable or random and therefore can not be prevented.1 Professionals and public may be less inclined towards “accident prevention” if they believe that such events are simply random acts of fate. Use of the alternative term “injury” implies no indication of the cause, intent, or predictability of the event. Some countries and leading prevention organisations have stopped using “accident” terminology referring instead to “injuries” and “injury control”.
However, not everyone accepts the need for change, pointing to the continued widespread use of “accident” and “accident prevention” by both the public and professionals. Furthermore, it has been argued that the term “injury” can not fully replace “accident” because the two terms describe different things.2 For example, an “accident” may occur without anyone being injured, “injuries” may be intentionally inflicted while “accidents” are not.
At present, there is some confusion and a lack of consistency in the terminology adopted by different countries, organisations, and groups. While “injury” is widely used by academics and specialists in “injury control”, the public and many professional groups working directly with the public still refer to “accident” and “accident prevention”. Surprisingly, in this evidence based world, there appears to be little published literature as to the impact of the two alternative terminologies.
In other areas of health and social care, altered terminology has been shown to have an impact on public perceptions. For example, Eayrs et al studied the use of three alternative terms: “mentally subnormal”, “mentally handicapped”, and “people with learning difficulties”.3 Using an attitude questionnaire to assess public perception, the authors reported more positive attitudes were associated with the term “learning difficulties”. However, people with learning difficulties were also perceived to be less deserving of special provision.
In the accident/injury debate, most work has focused on understanding the public perception of the word “accident”. Most recently, Girasek undertook a national telephone survey of 943 adults in the United States.4 The majority (71%) of respondents did indeed report that they believed that “accidents” were unpredictable. However, respondents also reported that “accidents” were preventable (83%). Most associated “accident” with something that was not done on purpose—that is, unintentional. In another national telephone survey in the US, Eichelberger et al reported that parents' beliefs in the avoidability of injuries were equally strong regardless of whether “accident” or “injury” was used.5
Many professional groups have a part to play in accident/injury control. These include specialist injury prevention workers and those who incorporate injury prevention as part of their general duties. The degree to which these professionals' perceive accidents/injuries to be predictable and preventable is likely to be an important factor in how they approach accident/injury prevention activities. If the arguments concerning the two terminologies are accepted, use of the term “accident” may have a negative effect promoting the belief that “accident prevention” activities are futile because such events are due to chance. There is little evidence on the effect of the alternative terminology on professional attitudes. This paper describes the result of a randomised comparative study of professional responses to the two terms.
Method
The aim of the study was to test the hypothesis that use of the term “injury” in place of “accident” can influence professional attitudes towards “accident/injury” occurrence and prevention.
SETTING
Leeds Health Authority serves the population (n=740 000) of the city of Leeds in the Yorkshire region of England. Despite an upturn in prosperity in recent years, the city still has areas of considerable deprivation particularly in the inner city.6 Ten per cent of the population are from ethnic minority backgrounds.7
SUBJECTS
The study was directed at health visitors working within the Leeds area of the UK. Health visitors form part of the National Health Service (NHS) community health services and have a remit to promote health and wellbeing in the community. With a nursing background with further specialist training, health visitors work closely with other members of the primary healthcare team. Although their remit covers all ages and groups, they have a particular role in the care of children aged under 5 years advising on a range of issues concerning healthy growth and development. Health visitors also advise parents on child safety inside and outside the home.
All health visitors (n=183) included on the central database of the Leeds Community and Mental Health Services were included in the survey. The database included details of the health visitor's name and base location. The majority of health visitors work as part of a general practice or are based at an NHS health centre (where several general practices together with a range of community health services work from one premises). In addition, 16 health visitors also worked as “bank” staff who could be called on to fill in particular areas as required. Six health visitors were not attached to a particular area or practice but had remits covering specific vulnerable groups. In order to minimise cross contamination between different arms of the study, health visitors were grouped according to their main place of work (health centre, general practice, “specific remit”, or bank). These locations were then stratified according to size (defined by number of health visitors located at the base), and randomised to two groups using a random number generator. All health visitors included in the database were female.
Data collection was by postal questionnaire. Two identical questionnaires were prepared—one using only “accident” terminology, the other using only “injury” terminology. The “accident” questionnaire defined accidents as “unwanted events that are expected or unplanned” while the “injury” questionnaire defined unintentional injuries as “injuries which are not deliberately caused by another person”. The questionnaires were designed to see if any difference in response between the two arms of the study could be detected using the alternative terminology. The questionnaire included a series of statements or scenarios relating to accidents/injuries with visual analogue scales for respondents to express whether they agreed or disagreed. Finally, respondents were presented with a number of public health problems and asked to rank them according to importance. Key issues addressed within the questionnaire were attitudes relating to the preventability of the accidents/injuries, victim blaming, and the relative importance of accident/injury prevention compared to other areas of the health visitor remit.
The questionnaires were piloted with the assistance of health visiting staff based outside the Leeds area. The pilot study assessed the ease of completion and comprehension of the questionnaire. No modifications were made to the questionnaires as a result of the pilot study.
Health visitors working at bases randomised to the “accident” or the “injury” group received the appropriate questionnaire. Both groups also received a covering letter—using appropriate terminology for their group—that explained that the study was “investigating the impact of presentation and terminology in injury prevention work” but did not elaborate on what kind of terminology was being assessed. Respondents were asked to complete the questionnaire on their own without consulting colleagues.
Allowing for a 50% response rate, the study was designed to identify approximately a 25% difference in group means at p=0.05 with power = 0.8, assuming a typical visual analogue response of 5, with a standard deviation of 2. All data received were entered into a SPSS database.8 Given the skewed distribution of responses, analysis was by Mann-Whitney U tests (using the 5% significance level).
Results
Altogether 183 health visitors were included in the sampling frame. After randomisation, 94 were randomised to receive the accident questionnaire and 89 were randomised to receive the injury questionnaire. Eighty nine questionnaires were completed and returned, 50 in the “accident”group (53% response) and 39 in the “injury” group (44% response) (95% confidence interval for difference –0.05 to 0.23).
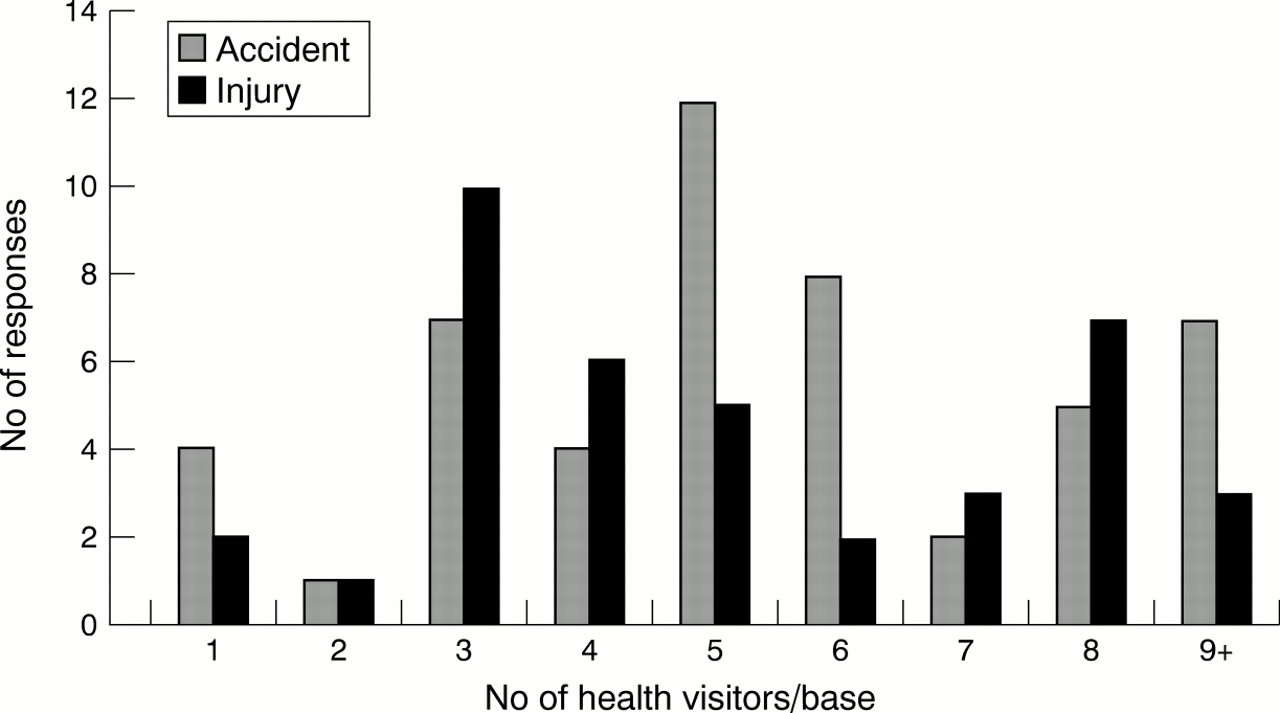
Health visitor response by base location (grouped according to number of health visitors at base) is shown in fig 1. The “accident” group shows a greater number of responses for bases with five or six health visitors, while the “injury” group shows a greater response for bases with three or four health visitors. No bank staff returned completed questionnaires. However, there is nothing to suggest any systematic bias between the groups in the type of base represented amongst the responses.
{kind=link}
Health visitor response by base location.
The mean responses in each group shown in table 1 are very similar. Only when asked to rank eight different public health priorities did any significant difference emerge. The “accident” group A ranked “accident prevention” more highly than the “injury” group ranked “injury prevention”. This finding was just significant at p=0.04. Adjustment for the clustering effect caused by the sampling procedure had negligible effect on the findings.
Questionnaire responses of the “accident” and “injury” groups
Discussion
This study has shown little difference in health visitor responses when “accident” is replaced with “injury”. No evidence was found that replacing “accident” with “injury” could favourably influence professional responses in relation to issues such as the preventability of accident/injuries, victim blaming, or the relative importance of accident/injury prevention compared to other public health priorities. Indeed, the only finding where group responses differed suggested a more positive effect for the term “accident”. The “accident” group ranked “accident prevention” as being of greater relative importance than the “injury” group. This finding was just statistically significant at p=0.04. However, this may have been a chance finding due to the multiple comparisons made. The “accident” group also had a higher response rate than the “injury” group. This could again suggest that “accident” was more likely to stimulate a response than “injury” among this group of professionals. The difference in responses was, however, not statistically significant.
There are a number of possible explanations for this apparent lack of effect. Firstly, the finding may be a true finding. This explanation is consistent with the findings of previous work in this area. For example, Eichelberger et al reported no difference in public responses whether accident or injury was used,5 while others have reported that “accident” is associated in public responses with notions of predictability and preventability.9–11 The finding that professionals who communicate with the public on a daily basis share similar attitudes is, perhaps, not surprising.
However, other possible explanations must also be considered. Firstly, the questionnaire may have been too insensitive to detect a true difference. The questionnaires were made up of a series of statements and scenarios using visual analogue scales for responses. These may have been too simple to detect subtle differences. The scenarios themselves were deliberately designed to interest the respondents and stimulate a response. The scenarios chosen were thus fairly emotive—concerning issues such as child injury, blame, and responsibility. It is possible that the emotive nature of the scenarios may have masked any subtle effect that might have been produced by the change of terminology. However, there is little in the field of accident/injury prevention that is not emotive. If changing the terminology produces so little an effect, is such a change warranted?
Secondly, the difference between the two groups may have been too small to be detected by a sample of this size. The samples were sufficient to detect a difference of just over 25% in group means at p=0.05, power = 0.8, assuming a typical visual analogue response of 5, with a standard deviation of 2. This equates to around a 1.3 cm difference between the group means on a 10 cm visual analogue scale. Any difference below this figure would not have been detected.
Thirdly, there is the possibility of crossover contamination, where respondents in one group saw the questionnaires from the other group. However, randomisation by place of work should have minimised this possibility. The randomisation process itself was a pragmatic approach designed to adjust for the health visiting staff's different working environments. Comparison of group responses by base location did not suggest any systematic bias in the type of responses received. A desire to keep the questionnaire as brief as possible meant that additional demographic data was not collected from the respondents. However, all respondents were female and obviously of similar professional background. No information is available on respondents' age.
There is also the question of whether the wording of the covering letter may have alerted respondents to the nature of the study. The covering letter stated that the study was investigating “the impact of presentation and terminology in “accident” (or “injury”) prevention work”. No further details were given as to the nature of the study. It could be argued that the phrase “terminology” should not have been mentioned. However, not to have done so would have raised ethical concerns about the study participants understanding of the investigation.
Fourthly, it is possible that the professional group studied was “too sophisticated”. Professionals working in the accident/injury prevention field are familiar with the alternative terminologies and likely to use them interchangeably. Health visitors were identified as the study group to represent “frontline health professionals” who include accident/injury prevention as part of a much wider remit, as opposed to “injury specialists”.
Much further study would be required to elucidate which, if any, of the above explanations is the true one. It may be that the effect of changing terminology is more nebulous—influencing society at large—similar to the gradual shift in attitudes to tobacco smoking. Such a change would be difficult to quantify. It is possible that no impact of any terminology change will be seen until it is accepted by the wider society. However, it would be as well to recognise the lack of evidence and clarity relating to the terminology debate. Otherwise, there is a danger that the “injury” believers may become alienated from the “accident” diehards.
Acknowledgments
The author wishes to acknowledge the help and support of Mr Peter McGinnis and staff at Department of Nursing and Quality, Leeds Community and Mental Health Services, as well as staff at the Primary Care Development Unit, York who assisted with the pilot study. I also thank all those who took part in the survey. At the Nuffield Institute for Health, Leeds, Darren Greenwood provided valuable statistical advice and Rhys Williams and Mike Robinson gave helpful comments on earlier drafts of the paper. I also acknowledge the helpful comments made by both the editor of the journal, Professor Barry Pless, and by the reviewers of the original draft of the manuscript.