Article Text

Abstract
Objective—To compare risks for falls and their consequences among four major race/ethnic groups in California.
Methods—Cases are 104 902 hospital discharges of California residents with a same level fall injury as the principal external cause of injury. Included are all discharges for a first hospitalization for a given injury in any California non-federal hospital from 1995–97. Analysis includes crude and age standardized rates to describe risks, diagnoses, and consequences.
Results—Rates per 100 000 for same level hospitalized fall injuries for whites (161) are distinctively higher than for blacks (64), Hispanics (43), and Asian/Pacific Islanders (35). Whites are more likely to have a fracture diagnosis and to be discharged to long term care rather than home, suggesting a poorer outcome or greater severity. Same level falls absorb a large proportion of hospital resources directed to the treatment of injuries.
Conclusions—In a four way comparison among race/ethnic groups, whites are distinguished by their high incidence, rates of fracture, and unfavorable discharge status. Prevention, particularly aimed at whites, has potential to improve health and save treatment resources.
- falls
- race
Statistics from Altmetric.com
Falls are a major source of injury mortality and morbidity. In California in 1997, falls caused 7% of all injury deaths and, remarkably, 41% of all non-fatal injury hospitalizations. Falls have distinctive age and sex risk patterns. Unlike other common causes of injuries (traffic and violence, for example), fall rates climb steadily with age, reaching extremely high rates among the elderly. In these older groups, rates for women exceed those for men. These unusual age and sex patterns are well documented, both in the medical literature (which focuses mainly on osteoporosis and hip fractures)1–11 and in the epidemiologic literature.12–20
Falls also show race differentials unlike those of other injuries. In studies providing a comparison between whites and non-whites, whites appear to have higher rates of fall injuries. For example, in California, adult (age 20+) hospitalization rates for non-fatal falls among whites were two to five times higher than for other races (unpublished data, in press). In a study of persons 65+ years of age with fractures almost entirely from falls, white fracture rates were twice those of blacks.10 In another study of persons 65+ years, emergency medical transport rates for falls among whites were 1.4 times higher than for blacks. A predominately white population was also reported to have fall rates about twice those of Hawaiians of Japanese ancestry.1 A few researchers have studied falls among blacks21, 22 and Mexican Americans (with no race/ethnicity comparisons).23 One study of hip fractures went so far as to exclude non-whites and males to control for race/sex confounding because white females are the majority of the hip fractured clinical population.1 No studies have compared fall injury rates simultaneously among all the major race/ethnicity groups.
Race patterns for fall injuries appear to be large enough to warrant more detailed characterization than they have received thus far. In this report we take advantage of California's size and diversity to examine hospitalized fall patterns for whites, blacks, Hispanics, and Asian/Pacific Islanders, by age and sex. We describe race differences in the risk of hospitalized fall injuries and selected financial and medical consequences.
Methods
E CODED HOSPITAL DISCHARGE DATA
The California Office of Statewide Health Planning and Development (OSHPD) provided computerized hospital discharge summaries for 1995–97. All non-federal acute care hospitals in California are legally required to report discharges to OSHPD. Hospitals must report external cause of injury (E codes) from the International Classification of Diseases, Ninth Edition, Clinical Modification (ICD-9-CM). Only first admissions for an injury are E coded. By selecting only E coded records, we selected incident cases and avoided duplication of cases readmitted or transferred. Hospital discharge data are generally reliable, as demonstrated by OSHPD's studies. To ensure quality data, OSHPD performs both computerized edits and analyst reviews on every discharge record.
CASE DEFINITION
This California-wide study includes only falls from slipping, tripping, or stumbling on the same level (E885) among residents of all ages requiring hospitalization in 1995–97. This (E885) is the most common type of fall, accounting for 32% in people 20–54 years and 43% in those 55 years and older. As we have previously shown that fall risk factors and consequences differ by type of fall (unpublished data, in press), we did not aggregate different types of falls.
Study cases, therefore, consist of all first admissions of California residents where the principal external cause of injury is a same level fall (E885). We examined data for three years combined (1995–97) to increase the number of cases and permit a detailed examination of all major race/ethnicity groups.
ANALYSIS
To determine risk, we calculated average race/ethnicity crude incidence rates per 100 000 California population per year (rate = mean falls for 1995–97/California population, 1 July 1996 × 100 000). Non-overlapping confidence intervals (CI) define statistical significance at the 95% level. California population estimates for 1996, provided by the California Department of Finance, include white, black, Hispanic, Asian, and Native American, a small category (n=162 same level falls for 1995–97) not included in our analyses. Among Californians age 55 years and older, age composition varies by race/ethnic group. For example, the proportion of white females age 85+ (2.7%) was 2.5 to 4 times greater than in the other race/ethnicity categories. Because age is strongly associated with fall incidence, compositional difference could make white women spuriously appear to be at greater risk. Rate comparisons are either shown as age specific rates or are directly standardized to the year 2000 standard million established by the National Center for Health Statistics.24
Costs include only hospital charges for first admission (excluding professional fees, which are not included in the discharge dataset) and thus underestimate total medical costs (which would include the costs of pre-hospital care, professional fees, and treatments after the first acute care discharge).
Fractures, particularly in seniors, are often associated with osteoporosis, prompting us to look for osteoporosis diagnoses. Only 8.3% of our fall cases 55 years or older had osteoporosis listed as a comorbidity on the discharge record. Other studies suggest this prevalence is low.25–28 Therefore, we did not try to determine whether osteoporosis could account for race differentials in hospitalized fall injuries.
Results
SEX, RACE, AND AGE
A total of 104 902 residents of California suffered serious falls on the same level (“same level falls,” hereafter) requiring hospitalization, an average rate of 108 per 100 000. These same level falls were the leading hospitalized injury, accounting for 16% of all hospitalized injuries during the study period. Although this study does not examine trends, same level fall injuries increased significantly over the study period:
• 1995—32 928 falls, rate 103 (95% CI 102 to 104)
• 1996—35 123 falls, rate 109 (95% CI 107 to 110)
• 1997—36 851 falls, rate 112 (95% CI 111 to 113)
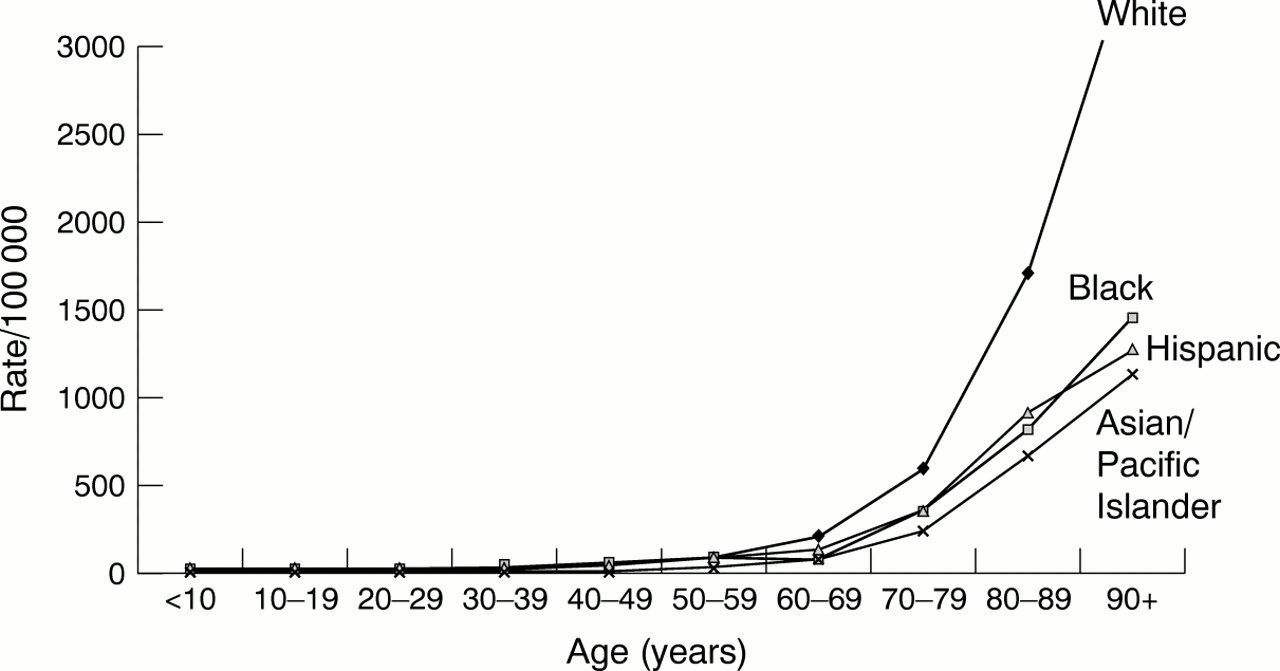
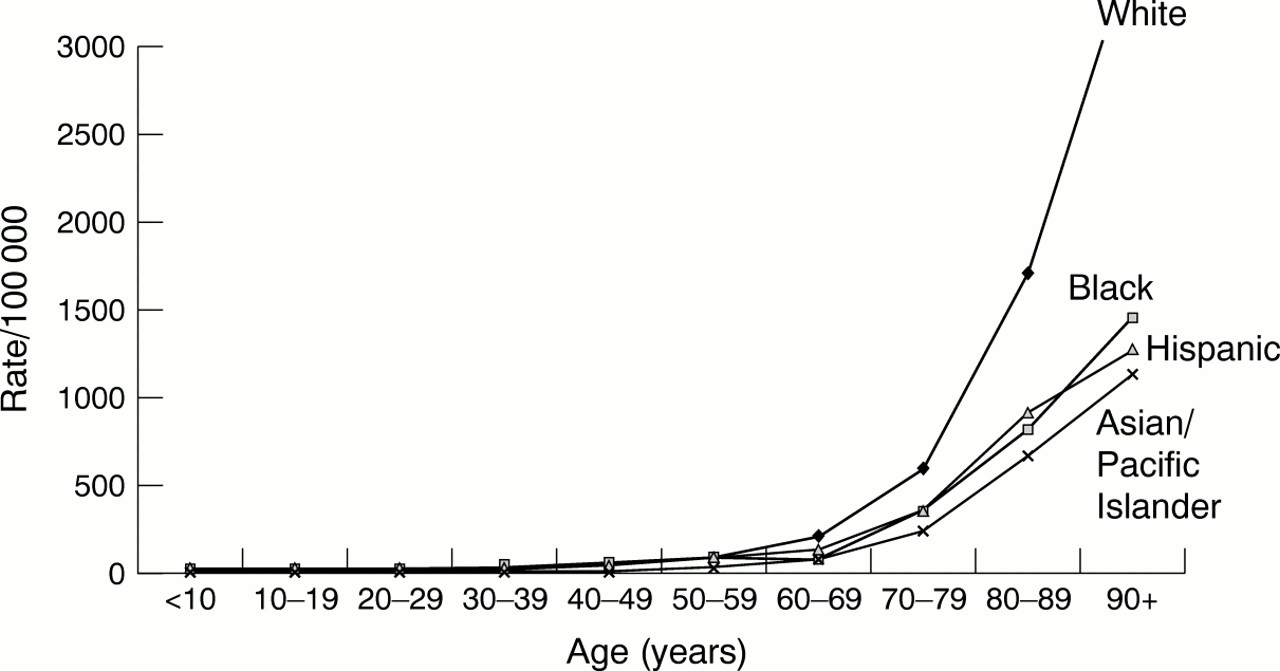
Table 1 shows detailed age-sex-race patterns. The major findings are: (1) in all race groups, rates increased rapidly after age 50–59; (2) the rates for whites were very high (161 for all ages), compared with blacks (64), Hispanics (43), and Asian/Pacific Islander (35) (all statistically significant at p <0.05); and (3) women consistently had higher rates than men after age 50–59. Figure 1 vividly illustrates that older whites had distinctively high rates, despite statistically significant differences in rates among the other race/ethnic groups.
Annualized injury hospitalization rates (per 100 000) for same level falls by race/ethnicity, sex, and age, California residents, 1995–97
{kind=link}
Annualized injury hospitalization rate (per 100 000) for same level falls by race/ethnicity, California residents, 1995–97.
Most same level fall injuries (70%) resulted in hospitalization because of a fracture. Table 2 shows significant differences in age adjusted admission rates for any fracture for both sexes. The largest race differential was for hip fracture, the predominant fracture, with the white rate about twice that of Hispanics and blacks and 3 times as large as the rate for Asians/Pacific Islanders. The ratio of female to male admission rates because of hip fracture was 1.4:1 for blacks and 2:1 for the other major race/ethnicity categories.
Principal diagnosis of hospital admission rates (per 100 000) and 95% confidence intervals (CI) for patients hospitalized for same level fall injuries, by sex, California residents, 1995–97
RACE/ETHNICITY AND OUTCOMES OF FALLS
Table 3 shows age adjusted disposition at discharge rates for same level fall injuries by race/ethnicity category. Although transfers to long term care and a routine discharge home were the major discharge destinations for all race/ethnicity categories, here, too, rates differed greatly by race/ethnicity. White females and males were transferred to long term nursing home care at a significantly higher rate, and Asian/Pacific Islanders at a significantly lower rate, than the other categories. This was also the pattern for a routine discharge home. However, within race/ethnicity categories, females (particularly whites and Hispanics) had the highest rates and were more at risk of being discharged to a long term care facility than males. But males, except whites, were significantly more likely to be discharged home than to long term care than females. Although the rate of males and females dying in hospital after being admitted because of same level fall injuries was low, whites of both sexes had significantly higher rates than their non-white counterparts.
Disposition at discharge rates (per 100 000) and 95% confidence intervals (CI) for patients hospitalized for same level fall injuries, by sex, California residents, 1995–97
Same level fall injuries constituted a large proportion of hospital charges billed for the treatment of injuries. For whites, same level falls amounted to nearly one fourth of the charges for all injuries (24%), almost twice as high as the proportion for Asian/Pacific Islanders (13%), and about three times as high as the proportion for blacks (7%) and Hispanics (8%) (data not shown). Falls, while consuming a minor proportion of charges for injuries among children and young adults, became a significant contributor after age 50. By age 80, a majority of charges for injuries were attributed to same level falls. Patterns for the race/ethnicity groups (data not shown) were similar up to age 59. From age 60 and over, the percentage of fall related charges for whites rises greatly compared to the other race/ethnicity groups.
Discussion
This is the first published population based study of hospitalized fall injuries comparing four major race/ethnic groups. The findings strongly confirm what other research had suggested—that whites have a distinctively high fall injury rate.13–29 To control somewhat for possible differences in behavior that might affect risk of falling, we limited our analysis to falls on the same level.
A main limitation of this study is our inability to study some known risk factors (for example, environmental hazards and medication use) that are not included in California hospital discharge records. Furthermore, hospital records for 1995–97 did not identify type of fall for 89 841 (or 37%) of all cases. To the degree that unidentified fall injuries include same level falls, we underestimate incidence and costs. Unidentified fall injuries have age and race/ethnicity patterns similar to fall injuries on the same level.
Other research has documented strong differences in fall injury rates by age, sex, and race/ethnicity. Our study found that these differences appear to be independent. That is, rates within each of the four major race/ethnic groups have a distinctive age curve for males and females. Among older people, rates for white women are roughly twice that of women in other race/ethnic groups. Although not part of this analysis, we also found that older whites have the highest fall death rates of the major race/ethnic groups.
In exploring these race/ethnic differences, we found hip and leg fractures to be the most common principal diagnosis, particularly among whites. This pattern could implicate bone differences (osteoporosis) as an explanation for the race/ethnic differences we found. Some research certainly points in this direction. Nevitt et al found, as did we, that fractures result from falls most often in whites.13 Compared with blacks, whites have been found to have higher fracture rates in general,10, 13, 30, 31 which is consistent with a body of research showing that bone mass density is lower in whites.11, 32–34 All this suggests that the distinctive pattern we found for older whites may have its etiology in bone density, although other explanations, such as a greater tendency to fall or to report falling, cannot be ruled out.13 One possibility is that whites are more readily able to access medical services than non-whites, because whites have higher socioeconomic status. Using expected payer as a socioeconomic status surrogate, we found that non-whites were nearly four times as likely to have their hospitalization paid for by a public assistance program than whites (28% v 5%).
Implications for prevention
This study certainly supports the notion that falls are worthy of a great deal of attention by public health professionals. Even limiting ourselves to falls on the same level, the rate, number, and costs of these injuries are extremely large. The proportion and number of people in the older age groups are projected to grow, exacerbating the strain on resources.35
Our study, and a recent one by Gill et al focusing on injury and non-injury falls,36 suggest that falls among older people are less a matter of environmental hazards than of physical factors, such as bone mass and physical condition. This would argue for fall prevention based on strategies such as osteoporosis prophylaxis, balance training, and other physical conditioning. Therefore, for public health policy, it is prudent to consider Gill and colleagues' recommendation to use sparse fall prevention resources to modify known intrinsic risk factors.36
The distinctive pattern of fall injuries and outcomes for whites requires a closer look at factors affecting this group. White rates are so raised that they become an attractive target for intervention. In our study, whites were only 29% of the population but accounted for over 53% of all same level fall injuries. Moreover, there is some evidence that prevention strategies may work differently among the race/ethnic groups. For example, research has found race differences in exercise preferences37 and in lactase deficiency and dietary intake of calcium from dairy products.38 There may be other systematic differences between whites and other race/ethnic groups that need greater elucidation.
Acknowledgments
The California Department of Health Services supported this research.