
Abstract
Summary
Chronic stroke survivors with low hip bone density are particularly prone to fractures. This study shows that fear of falling is independently associated with falls in this population. Thus, fear of falling should not be overlooked in the prevention of fragility fractures in these patients.
Introduction
Chronic stroke survivors with low bone mineral density (BMD) are particularly prone to fragility fractures. The purpose of this study was to identify the determinants of balance, mobility and falls in this sub-group of stroke patients.
Methods
Thirty-nine chronic stroke survivors with low hip BMD (T-score <−1.0) were studied. Each subject was evaluated for the following: balance, mobility, leg muscle strength, spasticity, and fall-related self-efficacy. Any falls in the past 12 months were also recorded. Multiple regression analysis was used to identify the determinants of balance and mobility performance, whereas logistic regression was used to identify the determinants of falls.
Results
Multiple regression analysis revealed that after adjusting for basic demographics, fall-related self-efficacy remained independently associated with balance/mobility performance (R2 = 0.494, P < 0.001). Logistic regression showed that fall-related self-efficacy, but not balance and mobility performance, was a significant determinant of falls (odds ratio: 0.18, P = 0.04).
Conclusions
Fall-related self-efficacy, but not mobility and balance performance, was the most important determinant of accidental falls. This psychological factor should not be overlooked in the prevention of fragility fractures among chronic stroke survivors with low hip BMD.
Similar content being viewed by others

Introduction
Individuals with stroke sustain more than a twofold increase in fall risk when compared with the reference population [1]. Fall incidence values ranging from 2.0 to 15.9 per 1,000 person-days have been reported [2, 3]. Falls in the chronic stroke population have been associated with poor balance and mobility [4–6]. Stroke-related physical impairments, such as muscle weakness [7, 8] of the lower extremity and spasticity at the ankle [7] may contribute to deficits in balance and mobility performance.
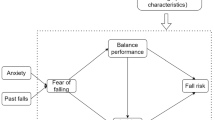
In addition to physical impairments, psychological factors may also influence balance and mobility performance following stroke. One of the psychological factors that has received increasing attention is fall-related self-efficacy [9–15]. Fall-related self-efficacy refers to the level of confidence a person has in performing daily activities without falling or losing his/her balance [12–14]. Fall-related self-efficacy can be evaluated by the Falls Efficacy Scale (FES) [10, 11] or Activities-specific Balance Confidence Scale (ABC) [12, 13], or measured as a dichotomous variable (presence of fear of falling: Yes/No) [10]. Fear of falling is a major psychological barrier that may lead to self-imposed activity avoidance [14]. Restricted activity may result in further physical deconditioning, deterioration of balance and mobility function, thereby contributing to more falls [9, 15, 16]. Indeed, strong associations of fear of falling with balance, mobility, and falls have been reported in older adults [15–17]. A previous prospective study in stroke reported a significant relationship between change in fall-related self-efficacy (measured by FES) and recovery in balance and mobility function within the first year post-stroke, but no information on falls was provided [18]. A recent study also showed that among stroke survivors in subacute and chronic stage of recovery, a positive fall history is associated with less fall-related self-efficacy (measured by FES) [10].
An accidental fall is the leading cause of bone fractures in the stroke population [19]. Fractures among stroke survivors are associated with devastating consequences, such as increased mortality [20, 21] and increased disability [21, 22]. Stroke survivors with low bone mass are particularly prone to bone fractures. Up until now, no anti-fracture effects have been shown with fall prevention strategies [23]. Nevertheless, understanding the mechanisms underlying falls in this high risk population could help to develop effective interventions to reduce falls, thereby improving the quality of life of these individuals. Successful prevention of accidental falls may also translate into substantial reduction of health care costs related to treatment of fractures, considering that the lifetime cost of hip fractures is estimated as $81,300 US in the general population [24]. To date, no study has examined the contributions of fall-related self-efficacy to performance in balance, mobility, and falls in stroke survivors with low bone mass. This is a particularly important population to study because of their high risk for fracture. We hypothesized that fall-related self-efficacy was independently associated with balance and mobility function and accidental falls in chronic stroke survivors with low hip BMD.
Methods
Subjects
The data were collected from community-dwelling individuals with chronic stroke in Vancouver, Canada. They were recruited through a local rehabilitation hospital database, local stroke clubs and newspaper advertisements. They fulfilled the following inclusion criteria: (1) had a single stroke with onset ≥ 1 year, (2) were independent in ambulation with or without an assistive device for at least 10 m, (3) were 50 years of age or older, (4) were living at home, (5) a Folstein Mini Mental Status Examination (MMSE) score ≥ 22 [25], and (6) a femoral neck BMD T-score <–1.0 as measured by dual-energy X-ray absorptiometry (DXA). Individuals were excluded from the study if they (1) had other neurological conditions in addition to stroke, (2) had unstable cardiovascular disease, or (3) had other serious diseases that precluded them from participating in the study. Relevant information of the subject (i.e., type of stroke, surgical history, co-morbid conditions) was provided by the primary care physician. Potential participants gave informed, written consent to participate in the study. The study was approved by local research ethics committees. The study was conducted according to the Helsinki Declaration for human experiments.
Measurements
Demographics
For all subjects, age and post-stroke duration were measured in years. Height (to the nearest millimeter) and weight (to the nearest 0.1 kg) was measured using the Health O Meter (Continental Scale Corp., Bridgeview, IL, USA). Habitual physical activity level was evaluated by Physical Activity Scale for Individuals with Physical Disabilities (PASIPD) [26]. It is a 13-item questionnaire that assesses participation in physical activities of different intensities for the previous 7 days based on recall. A metabolic equivalent (MET) value was assigned to each activity. The maximal score that could be obtained was 199.5MET hour/day. The femoral neck BMD on the paretic side was measured by dual-energy X-ray absorptiometry (DXA; Hologic QDR 4500, Hologic Inc., Waltham, MA, USA) and the associated T-score was derived. This skeletal site was selected as it is the most common site of fracture in the stroke population [19].
Measures of balance and mobility
Berg Balance Scale
Balance performance was assessed by Berg Balance Scale (BBS). It is a 14-item assessment tool which evaluates the ability to balance in a variety of postures. Each item was rated based on an ordinal scale from 0 to 4, with a higher score indicating better balance performance. The BBS has been shown to be a reliable tool to assess balance in persons with stroke [27].
Timed up and go test
The timed up and go test (TUG) [28] is a common tool to evaluate functional mobility in individuals with stroke [8], participants were instructed to rise from a standard chair with arms, walk a distance of three meters, turn, walk back to the chair and sit down again. The time (in seconds) required to complete this task was measured by a stopwatch. The mean from two trials were computed and used for subsequent statistical analysis. Excellent reliability of the TUG has been demonstrated [intraclass correlation coefficient (ICC)> 0.95)] when used in the stroke population [8].
Stair climbing time
Subjects were instructed to walk up a four 18-cm steps with the option of using the railing as needed [29]. A stopwatch was used to record the time (in seconds) when both feet reached the top of the staircase. Two trials were performed and the data showed that this test has excellent intra-rater reliability (ICC = 0.95). The mean from two trials was calculated and used for statistical analysis.
Six-minute-walk test (6MWT)
Subjects were instructed to cover as much distance as they could around a 42-m rectangular path within 6 minutes [7]. The total distance walked was recorded. The 6MWT is a common outcome measure for evaluating ambulatory capacity in individuals with stroke and its reliability has been established [7].
Falls
Each subject was first asked whether they had had any falls in the past 12 months. Subjects were identified as “fallers” if any falls were reported. For fallers, the number of falls within the past 12 months and the circumstances surrounding the falls were recorded.
A fall was defined as coming to rest on the floor or another lower level but was not due to seizure, stroke or myocardial infarction, or an overwhelming displacing force [5].
Leg muscle strength
Hand-held dynamometry is a reliable method to measure leg muscle strength in stroke [30] and was used to evaluate isometric knee extension strength in this study (Nicholas MMT, Lafayette Instruments, Lafayette, IN, USA). With the subject sitting upright in a chair with back support and the knee placed in 90° flexion, a maximal isometric contraction of knee extension was performed by the subject while the thigh was stabilized by the assessor. Three trials were conducted on the paretic side. The force values obtained (Newtons) were averaged and then normalized by the subject’s body weight (kg).
Spasticity
Resistance to passive movements at the ankle on the paretic side was evaluated by the Modified Ashworth Scale (MAS) (0: no increase in muscle tone, 4: affected part rigid in flexion and extension). The MAS is a common tool used for evaluating muscle tone in individuals with stroke and its reliability has been established [31].
Fall-related self-efficacy
Fall-related self-efficacy was evaluated using the Activities-Specific Balance Confidence (ABC) scale (Appendix) [12, 13]. The scale consists of 16 functional activities, and the rating is based on a scale ranging from 0% (no confidence at all) to 100% (completely confident). Each participant was instructed to rate their level of confidence in performing each of the 16 activities without losing their balance or becoming unsteady (e.g., walking on a slope, walking in a shopping mall). The scores from all items were summed and then averaged to yield the mean ABC score. The ABC scale has been shown to have good internal consistency (Cronbach’s alpha = 0.94) and test-retest reliability (ICC = 0.85) among individuals with stroke [32]. A score above 80 indicated a high level of balance confidence characteristic of those in community exercise programs [13]. On the other hand, a score <80 indicates deficits in fall-related self-efficacy [13].
Statistical analysis
Descriptive statistics were used for relevant variables. Normality of data distribution was checked by using the Shapiro–Wilk Statistic. As BBS and TUG scores were not normally distributed, Spearman’s rho was used to determine their degree of association with other variables of interest. Mann–Whitney U tests were used to compare the differences in variables of interest between fallers and non-fallers.
The four balance and mobility measures (i.e., BBS, TUG, Stair climbing time, 6MWT) were then entered into a principal component analysis (PCA). Eigenvalues were set to be greater than 1 in the analysis. PCA is one of the statistical techniques used for data reduction and is useful in summarizing relationships among variables in a concise manner [33]. For example, if only one principal component is extracted from the analysis, it indicates that the four measures of balance and mobility represent the same theoretical construct [33].
First, a multiple linear regression analysis was performed to determine whether the ABC score had independent contributions to balance and mobility. In this regression model, the first principal component extracted from the PCA was the dependent variable. Then ABC scores were entered into the regression model after adjusting for age, gender, habitual physical activity level and other physiological variables (e.g., leg muscle strength) that had significant bivariate correlation with balance/mobility measures.
Logistic regression analyses were performed to identify the determinants of fallers (non-fallers=0, fallers=1). In the first model, we tested whether balance/mobility performance could determine fallers. The principal component extracted from PCA was entered into the regression model, after adjusting for age, gender, and habitual physical activity. In the second model, the subjects were categorized based on the cutoff ABC score (Group 1: ABC ≤ 80, Group 2: ABC > 80) [13]. This categorical variable was then entered into the model as an independent variable to determine fallers, after adjusting for age, gender and physical activity level. All data analyses were performed using SPSS 14.0. A significance level of 0.05 was set for all statistical tests.
Results
Subject characteristics
Thirty-nine subjects were included in the analysis. Subject characteristics are listed in Table 1. The mean femoral neck BMD on the paretic side was 0.746 ± 0.149 g/cm2, with 31 and eight subjects being diagnosed with osteopenia (−2.5< T < −1.0) and osteoporosis (T < −2.5), respectively. Nine subjects (23%) obtained a BBS score < 45, indicating significant balance problems [27, 34]. Fourteen subjects (36%) had a TUG score > 13.5 seconds, indicating significant deficits in functional mobility [35]. The mean 6MWT distance was 323.2m, which was approximately 50–60% of age-matched values [36]. Twenty-two (56%) subjects obtained an ABC score < 80, indicating a deficit in balance confidence [13].
Falls
Seventeen (44%) subjects were identified as fallers. The characteristics of fallers and non-fallers are described in Table 1. No significant difference was found between fallers and non-fallers in age (P = 0.943), physical activity level (P = 0.190), paretic leg muscle strength (P = 0.315), spasticity (P = 0.824), BBS score (P = 0.102), TUG score (P = 0.527), stair climbing time (P = 0.571) and 6MWT distance (P = 0.279). There was a trend for a higher ABC score among non-fallers than fallers (P = 0.084). A total of 25 falls were reported. The minimum and maximum number of falls reported by the fallers was 1 and 4, respectively. Five subjects reported more than one fall within the past 12 months. The circumstances surrounding the fall incidents are summarized in Table 2. A large proportion of falls occurred during walking (48%).
Relationship between balance/mobility performance and other variables
Associations between each of the balance/mobility measures and other variables of interest are shown in Table 3. Better fall-related self-efficacy (ABC scores) was significantly related to better balance (BBS score) (ρ = 0.667, P < 0.001), faster TUG score (ρ = −0.679, P < 0.001), faster stair climbing score (ρ = −0.511, P = 0.001), and longer 6MWT distance (ρ = −0.679, P < 0.001). Greater paretic leg muscle strength was significantly associated with faster TUG scores (ρ = −0.416, P = 0.008), faster stair climbing time (ρ = −0.358, P=0.025), longer 6MWT distance (ρ = −0.416, P = 0.008). Lesser spasticity was significantly related to faster stair climbing time only (ρ = 0.424, P = 0.007).
Principal component analysis
Only one principal component was extracted from the PCA, indicating that all four measures of balance and mobility represent the same theoretical construct [33]. The extracted principal component explained 83.6% of the total variance. Factor loadings (unrotated) for BBS score, TUG score, stair climbing time, and 6MWT distance were 0.901, −0.939, −0.887, and 0.929, respectively.
Multiple regression analyses
Age, gender, habitual physical activity level, and paretic leg muscle strength were first entered into the regression model (Table 4, model A). These factors combined to account for 16.9% of the variance in balance/mobility performance (F4,34 = 1.733, P = 0.166). In model B, we added ABC scores to the model, after controlling for age, gender, habitual physical activity level, and paretic leg muscle strength (Table 4, model B). Adding ABC scores accounted for another 32.4% of the variance in the dependent variable, causing a significant change in F-ratio (Fchange 1,33 = 21.135 P < 0.001). A total of 49.4% of the variance in balance/mobility performance can be explained by the final model (F5,33 = 6.434, P < 0.001) (Table 4, model B). According to the standardized regression coefficients (â), ABC score had the highest association with balance/mobility performance (0.635) (Table 4, model B).
Logistic regression analyses
Our results showed that balance/mobility performance did not significantly explain falls (adjusted odds ratio: 0.52, 95%CI: 0.24, 1.15, P = 0.11) (Table 5, model A). In contrast, fall-related self-efficacy was a significant determinant of fallers. Those with an ABC score > 80 were significantly less likely to fall when compared with those with an ABC score ≤ 80 (adjusted odds ratio: 0.18; 95%CI: 0.04–0.97, P = 0.04), after accounting for age, gender, and physical activity level (Table 5, model B).
Discussion
To our knowledge, this is the first study to demonstrate that fall-related self-efficacy, but not balance/mobility performance, is independently associated with falls in chronic stroke survivors with low hip BMD.
Contributions of fall-related self-efficacy to balance, mobility and falls
The results showed that fall-related self-efficacy, as measured by the ABC scale, is independently associated with balance and mobility performance in the studied population, accounting for more than 30% of the variance in balance and mobility performance. Our results also indicate that those with higher ABC scores (>80) are significantly less likely to fall than those with low ABC scores (≤80). The results are in agreement with previous studies in older adults which found that fear of falling is strongly associated with balance and mobility [13, 16, 17], and accidental falls [37]. Although some previous studies showed a significant bivariate correlation between ABC score and various measures of balance and mobility (BBS, gait velocity, TUG, six-minute-walk test) [10, 11, 38], and falls [10] in individuals with stroke, this study is unique in that all of our subjects were diagnosed with osteopenia or osteoporosis at the hip (T-score <−1.0). These individuals are especially prone to hip fractures (the most common type of bone fractures after stroke) due to their compromised bone health status [19]. Our findings may have particularly important clinical implications in terms of preventing fragility fractures within the chronic stroke population (will discuss below in the section on clinical implications).
It is intriguing that balance and mobility performance is not a significant determinant of falls in this study (Table 5, model 1). This finding concurs with the study by Harris et al. [39], which found that the BBS score or gait speed alone was unable to explain falls in community-dwelling people with chronic stroke. Specifically, they [39] found that those who had poor BBS scores and low gait velocity but used a wheelchair or walker for longer distances had a low risk for falls, whereas those with better BBS scores and higher gait velocity but used a cane for ambulation had a higher risk for falls. In another recent study using receiver operating characteristics (ROC) curve analysis, it is shown that fall-related self-efficacy, as measured by the FES, has superior ability to discriminate fallers and non-fallers in community-dwelling individuals with chronic stroke when compared with mobility and balance measures (BBS, TUG) [10]. Indeed, factors causing falls in the stroke population must be complex. The type of assistive device, exposure to risky situations, environmental conditions may all have an effect on falling. The complex relationship between falls and balance/mobility measures is also reflected in studies on post-stroke fractures. Melton III et al. [40] found that fracture risk in stroke is increased with moderate but not severe disability. The authors concluded that moderate physical impairment allows the patients to be independently mobile and therefore increase the exposure to risky situations and falls whereas those who are more severely impaired may have limited exposure to such fall-inducing situations [40]. However, the lack of a significant association between falls and balance/mobility measures (P = 0.11, Table 5) in this study may be related to inadequate statistical power due to the small sample size. We cannot rule out the possibility that a significant association between falls and balance/mobility performance would be found if a larger sample size was used.
Nevertheless, fall-related self-efficacy, a psychological factor, is more important than other physiological factors (e.g., paretic leg muscle strength, spasticity) in determining balance/mobility performance and falls. Our findings thus concur with Bandura’s theory of self-efficacy, which states that the perceived ability is more predictive of behavior than is actual physical ability [41]. Results from a previous study in stroke also have substantiated this theory. Salbach et al. found that ABC score is a more important determinant of physical function (as measured by SF-36 physical function scale) than other demographic or physiological measures in individuals with stroke [37].
Given the association between falls and fall-related self-efficacy, one may be tempted to ask which condition (i.e., frequent falls or low fall-related self-efficacy) comes first. This is a cross-sectional correlational study and therefore could not determine causality. Some possible scenarios may explain the association between fall-related self-efficacy and falls. First, an experience of a fall may cause fear of further falls (i.e., fall–fear scenario). In this case, prevention of falls should be a primary goal of intervention. In contrast, fear of falling may cause falls (i.e., fear-fall scenario). Fear of falling may lead to avoidance of physical activities, resulting in further deconditioning. The impaired mobility and balance ability that ensues may in turn increase the risk of falling [42, 43]. Prevention of the development or progression of fear of falling thus becomes very important in this scenario. Alternatively, the association between falls and fear of falling may be explained by the shared risk factors, such as cognitive deficits [9]. A large prospective study in older adults has found that falls at baseline (falls within the past 12 months based on recall) is an independent predictor of fear of falling 20 months later (odds ratio: 1.75). On the other hand, fear of falling at baseline (yes or no) is an independent predictor of falling at 20-month follow-up (odds ratio: 1.79) [37]. Therefore, it is likely that each scenario or combination of scenarios results in a vicious cycle of fear of falling, falls, and functional decline [37]. We postulate that the first scenario is more likely in our subjects, as fall-related self-efficacy, but not balance and mobility performance, is a determinant of falls. However, we could not rule out other possibilities due to the cross-sectional design.
Clinical implications
The results point to several important clinical implications. First, as fall-related self-efficacy can distinguish between fallers and non-fallers, one possible clinical implication is that the ABC scale can be used as part of the initial assessment to identify those with increased fall risk. Second, over half of the subjects have significant deficits in fall-related self-efficacy (i.e., ABC score <80). Falls-related efficacy is also strongly related to balance, mobility, and falls. Therefore, fear of falling should be taken into consideration in assessment and treatment of stroke survivors with compromised bone status. Various intervention approaches have been used to reduce fear of falling or promoting fall-related self-efficacy. Cognitive-behavioral intervention program, which contains group discussion, mutual problem solving, exercise training, assertiveness training, has been shown to be effective in improving fall-related self-efficacy and the perceived ability to manage risk of falls and actual falls among older adults [12]. There is also some evidence to suggest that certain forms of group exercise programs also improve fall-related self-efficacy in the stroke population [44]. In summary, one should not overlook the psychological factors such as fall-related self-efficacy in an effort to reduce incidence of falls and fractures in this specific population.
Limitations
We noted several limitations of the study. First, the subjects are all ambulatory and are mildly or moderately affected by stroke only. The results are, thus, not generalizable to those who are severely affected by stroke (e.g., those who are wheelchair-bound). However, a large proportion (>60%) of stroke survivors are able to regain ambulatory function [45]. Second, this is a cross-sectional analysis which cannot prove causation. We are not certain whether fear of falling causes more falls, or previous experience of falling causes more fear of falling. Third, the data on falls were collected retrospectively. Recall bias (e.g., under-reporting) could be high in stroke patients due to the possible effects of the neurological insult on memory function. Such recall bias may have negatively influenced the results. However, all of our subjects had a MMSE score >22 and should not have any severe impairment in cognition. Nevertheless, based on the significant findings from this study, it would be valuable to conduct a prospective study to track the incidence of falls and changes in fear of falling, balance, mobility, and other relevant outcomes as stroke recovery progresses.
Conclusion
This is the first study to show that fall-related self-efficacy is independently associated with balance, mobility and falls in chronic stroke survivors with low hip BMD. Fall-related self-efficacy could be a useful measure for screening individuals with high risk for fragility fractures. It could also serve as an important clinical outcome in the treatment of chronic stroke survivors with bone loss.
References
Jorgensen L, Engstad T, Jacobsen BK (2002) Higher incidence of falls in long-term stroke survivors than in population controls. Depressive symptoms predict falls after stroke. Stroke 33:542–547
Tutuarima JA, van der Meulen JHP, de Haan RJ et al (1997) Risk factors for falls of hospitalized stroke patients. Stroke 28:297–301
Nyberg L, Gustafson Y (1995) Patient falls in stroke rehabilitation: a challenge to rehabilitation strategies. Stroke 26:838–842
Lamb SE, Ferrucci L, Volapto S et al (2003) Risk factors for falling in home-dwelling older women with stroke. The women’s health and aging study. Stroke 34:494–501
Hyndman D, Ashburn A, Stack E et al (2002) Fall events among people with stroke living in the community: circumstances of falls and characteristics of fallers. Arch Phys Med Rehabil 83:165–170
Hyndman D, Ashburn A (2003) People with stroke living in the community: attention deficits, balance, ADL ability, and falls. Disabil Rehabil 25:817–822
Eng JJ, Chu KS, Dawson AS et al (2002) Functional walk tests in individuals with stroke. Relation to perceived exertion and myocardial exertion. Stroke 33:756–761
Ng SS, Hui Chan CW (2005) The Timed Up & Go test: its reliability and association with lower-limb impairments and locomotor capacities in people with chronic stroke. Arch Phys Med Rehabil 86:1641–1647
Tinetti ME, Speechley M, Gineter SF et al (1988) Risk factors for falls among elderly persons living in the community. N Engl J Med 319:1701–1707
Belgen B, Beninato M, Sullivan PE et al (2006) The association of balance capacity and falls self-efficacy with history of falling in community-dwelling people with chronic stroke. Arch Phys Med Rehabil 87:554–561
Rosen E, Sunnerhagen KS, Kreuter M et al (2005) Fear of falling, balance, and gait velocity in patients with stroke. Physiother Theory Pract 21:113–120
Powell LE, Myers AM (1995) The Activities-Specific Balance Confidence (ABC) Scale. J Gerontol A Biol Sci Med Sci 50A:M28–M34
Myers AM, Fletcher PC, Myers AH et al (1998) Discriminative and evaluative properties of the Activities-specific Balance Confidence (ABC) Scale. J Gerontol A Biol Sci Med Sci 53:M287–294
Fletcher PC, Hirdes JP (2004) Restriction in activity associated with fear of falling among community-based seniors using home care services. Age Ageing 33:273–279
Tinetti ME, Mendes de Leon CF, Doucette JT et al (1994) Fear of falling and fall-related efficacy in relationship to functioning among community-living elders. J Gerontol 49:M140–M147
Maki BE, Holliday PJ, Topper AK et al (1991) Fear of falling and postural performance in the elderly. J Gerontol Med Sci 46:M123–M131
Liu-Ambrose T, Khan KM, Donaldson MG et al (2006) Fall-related self-efficacy is independently associated with balance and mobility in older women with low bone mass. J Gerontol Med Sci A 8:832–838
Hellstrom K, Lindmark B, Wahlberg B et al (2003) Self-efficacy in relation to impairments and activities of daily living disability in elderly patients with stroke: a prospective investigation. J Rehabil Med 35:2002–2007
Ramnemark A, Nyberg L, Borssen B et al (1998) Fractures after stroke. Osteoporos Int 8:92–95
Farahmand BY, Michaelsson K, Ahlbom A et al (2005) Swedish Hip Fracture Study Group. Survival after hip fracture. Osteoporos Int 16:1583–1590
Ramnemark A, Nilsson M, Borssen B et al (2000) Stroke, a major and increasing risk factor for femoral neck fracture. Stroke 31:1572–1577
Di Monaco M, Vallero F, Di Monaco R et al (2003) Functional recovery and length of stay after hip fracture in patients with neurologic impairment. Am J Phys Med Rehabil. 82:143–148
Eng JJ, Pang MYC, Ashe MA. Role of exercise in reducing the risk of fracture after stroke. J Rehabil Res Dev. In press.
Braithwaite RS, Col NF, Wong JB et al (2003) Estimating hip fracture morbidity, mortality and costs. J Am Geriatr Soc 51:364–370
Folstein MF, Folstein, SE, McHugh PR et al (1975) Mini-Mental State: A practical method for grading the state of patients for the clinician. J Psychiatr Res 12:189–198
Washburn RA, Zhu W, McAuley E et al (2002) The physical activity scale for individuals with physical disabilities: development and evaluation. Arch Phys Med Rehabil 83:193–200
Berg KO, Wood-Dauphinee SL, Williams JI et al (1992) Measuring balance in the elderly: Validation of an instrument. Physiother Can 41:304–311
Podsiadlo D, Richardson S (1991) The timed “Up & Go”: a test of basic functional mobility for frail elderly. J Am Geriatr Soc 39:142–148
Kim CM, Eng JJ (2003) The relationship of lower-extremity muscle torque to locomotor performance in people with stroke. Phys Ther 83:49–57
Bohannon RW (1997) Measurement and nature of muscle strength in patients with stroke. J Neuro Rehabil 11:115–125
Bohannon RW, Smith MB (1987) Interrater reliability of a Modified Ashworth Scale of muscle spasticity. Phys Ther 67:206–207
Botner EM, Miller WC, Eng JJ (2005) Measurement properties of the Activities-specific Balance Confidence Scale among individuals with stroke. Disabil Rehabil 27:156–163
Tabachnick B, Fidell L (eds) (2001) Using multivariate statistics. 4th edition. Allyn and Bacon, Boston
Bogle Thorbahn LD, Newton RA (1996) Use of the Berg Balance Test to predict falls in elderly persons. Phys Ther 76:576–582
Shumway-Cook A, Baldwin M, Polissar NL et al (1997) Predicting the probability of falls in community-dwelling older adults. Phys Ther 77:812–819
Steffen TM, Hacker TA, Mollinger L (2002) Age- and gender-related test performance in community-dwelling elderly people: six-minute walk test, Berg balance sale, timed up & go test, and gait speeds. Phys Ther 82:128–137
Friedman SM, Munox B, West SK et al (2002) Falls and fear of falling: which comes first? A longitudinal prediction model suggests strategies for primary and secondary prevention. J Am Geriatr Soc 50:1329–1335
Salbach NM, Mayo NE, Robichaud-Ekstrand S et al (2006) Balance self-efficacy and its relevance to physical function and perceived health status after stroke. Arch Phys Med Rehabil 87:364–370
Harris JE, Eng JJ, Marigold DS et al (2005) Relationship of balance and mobility to fall incidence in people with chronic stroke. Phys Ther 85:150–158
Melton III LJ, Brown Sr RD, Achenbach SJ et al (2001) Long-term fracture risk following ischemic stroke: a population study. Osteoporos Int 12:980–986
Bandura A (1977) Self-efficacy: toward a unifying theory of behavioral change. Psychol Rev 84:240–245
Howland J, Tennstedt S, Lachman M et al (1998) A randomized, controlled trial of a group intervention to reduce fear of falling and associated activity restriction in older adults. J Gerontol Psychol Sci 53B:P384–392
Nevitt MC, Cummings SR, Kidd S et al (1989) Risk factors for recurrent nonsyncopal falls. JAMA 261:2663–2668
Salbach NM, Mayo NE, Robichaud-Ekstrand S et al (2005) The effect of a task-oriented walking intervention on improving balance self-efficacy poststroke: a randomized, controlled trial. J Am Geriatr Soc 53:576–582
Jorgensen HS, Nakayama H, Raaschou HO et al (1999) Stroke: Neurologic and functional recovery. The Copenhagen Study. Phys Med Rehabil Clin N Am 10:887–906
Funding
M.Y.C.P. was supported by a post-doctoral fellowship from Natural Sciences and Engineering Research Council of Canada. This study was supported by a grant-in-aid from the Heart Stroke Foundation of British Columbia and Yukon (J.J.E.) and from career scientist awards from Canadian Institute of Health Research (J.J.E) and the Michael Smith Foundation for Health Research (J.J.E.).
Conflicts of interest
None.
Author information
Authors and Affiliations
Corresponding author
Appendix
Appendix
Activities-specific balance confidence scale
Each subject indicates the level of self-confidence of losing balance or becoming unsteady when doing the following activities (0–100%):
-
1.
Walk around the house.
-
2.
Walk up and down stairs.
-
3.
Pick up a slipper from the floor.
-
4.
Reach at eye level.
-
5.
Reach while standing on your tiptoes.
-
6.
Stand on a chair to reach.
-
7.
Sweep the floor.
-
8.
Walk outside to nearby car.
-
9.
Get in and out of a car.
-
10.
Walk across a parking lot.
-
11.
Walk up and down a ramp.
-
12.
Walk in a crowded mall.
-
13.
Walk in a crowd or get bumped.
-
14.
Ride an escalator holding the rail.
-
15.
Ride an escalator not holding the rail.
-
16.
Walk on icy sidewalks.
aReprinted with permission of the publisher from: Powell LE, Myers AM. The Activities-Specific Balance Confidence (ABC) Scale. J Gerontol A Biol Sci Med Sci 1995;50A:M28–M34. Copyright 1995, The Gerontological Society of America.
Rights and permissions
About this article
Cite this article
Pang, M.Y.C., Eng, J.J. Fall-related self-efficacy, not balance and mobility performance, is related to accidental falls in chronic stroke survivors with low bone mineral density. Osteoporos Int 19, 919–927 (2008). https://doi.org/10.1007/s00198-007-0519-5
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00198-007-0519-5