Article Text

Abstract
Objectives We study the association between changing residence and risks of attempted suicide and violent assault injury in Alberta, Canada. Our primary objective is to understand whether a change in residence between urban, rural and semiurban areas is associated with increased risk of intentional injury.
Methods Study subjects are a cohort of residents linked to data on emergency department and inpatient hospital admissions between 1999 and 2010. We used generalised estimating equations to model the effects of changing residence on risk of intentional injury while controlling for the influence of age, sex, socio-economic status, Aboriginal status and history of intentional injury.
Results Changing residence is associated with an increase in the risk of both attempted suicide and violent assault injury. In the case of attempted suicide, this effect is strongest for persons between 20 and 35 years of age. For violent assault injuries, persons from rural regions that have recently moved to urban regions have higher risk of injuries, and women of rural origin are at higher risk of violent assault injury than women of urban origin.
Conclusions Our findings reveal an association between risk of intentional injuries and change of residence adjusting for geographical differences in injury risk. These findings suggest that intentional injury risk is associated with change in community at intraregional scales and that these populations may benefit from support that helps integrate them into their new communities.
Statistics from Altmetric.com
Introduction
Considerable evidence suggests that health and health behaviour changes following settlement in a new country, with years since migration often predicting a general worsening of health.1–4 Less research has described the health effects of migration at smaller geographical scales—such as between regions of a country—though some have described the relationship between small-scale changes in residence and accessibility to healthcare.5–7 Nevertheless, the relationship between intraregional migration and specific measures of health and well-being is still largely unknown, and while clearly some experiences of intranational migration fundamentally differ from the international variety, the process of changing community may be disruptive to health and well-being irrespective of the spatial and cultural distance between origin and destination of migrants.
The objective of this research is to study the relationship between intraregional migration and the risk of attempted suicide and violent assault injuries reported to hospitals. Our study region, Alberta, Canada, has experienced considerable movement of population within and into the province as a result of employment opportunities in the oil and gas sector. Migration within the province (as well as migration from other regions into the province) is generally believed to place demands on the healthcare system and other public services that can compromise the quality and timeliness of services. However, there has been little consideration of the burden of change on regionally migrating residents themselves. This research will not only determine what, if any, association intraregional (defined here as within-province) migration has with the risk of intentional injury, but also help understand how the challenges of intraregional migration may compare to the more well-understood challenges of international migration.
Methods
Data
The subjects used in this study are based on a cohort identified for earlier research on farm injuries.8 Virtually all residents of Alberta (>95%) are listed in a regularly updated public health insurance registration system, and these data are used to both identify current and historical demographic characteristics of the study population, and specifically age, gender, a measure of low socio-economic status (SES) and Aboriginal status. Study subjects comprise a random selection of rural non-farming and urban-non-farming Albertans selected from this population health insurance registry. Farming residents will be considered in a future separate study. Subjects were selected by first dividing the population into rural and urban based on place of residence at the end of the year 1999 and then excluding all residents who lived in a family in which one or more persons lived on a farm. Then subjects were selected from both groups independently at a uniform probability (without replacement). The data set includes data for the years between 1999 and 2010.
Each person in the study population is linked to two sources of health data: emergency department admissions (‘outpatient’) and hospital admissions (‘inpatient’). Linkages are deterministic based on a unique identifier used in the administration of the province's healthcare system. We link subjects to these data to identify years in which subjects visited an emergency room and/or were admitted to hospital one or more time. For outpatient and inpatient data, external cause of injury diagnostic information is available in multiple fields, but for both systems, a most responsible diagnostic code is available. This is used to classify type of injury most responsible for visiting a hospital. Over the study period, there was a shift in use of International Classification of Diseases (ICD)-9 to ICD-10 in the data system, so both codes are used for selection of intentional injuries. We also subdivided intentional injuries into attempted suicide injuries (ICD-9: E950-E959; ICD-10: X60-X84, Y87.0) and violent assault injuries (ICD-9: E960-E969; ICD-10: X85-Y09, Y87.1).
All subjects are classified as living in an urban, semiurban or rural area in each year between 1999 and 2010. Urban is defined as a residence in either of the two large cities in the province (Edmonton or Calgary), two large urban centres with populations close to 1 million persons. For each city, this definition includes regions within their municipal boundaries, but excludes adjacent suburban areas that are part of different municipalities. Smaller cities (populations under 100 000) are classified as semiurban. We define rural residence based on the mailing address of the subject (specifically, a ‘0’ in the second position of the postal code). Since this method is not based on the precise location of residence, it may mischaracterise some rural persons as urban and vice versa, which may bias effects associated with location and change of residence towards the null hypothesis. All other subjects are classified as semiurban. All subjects are classified as having changed their residence in each year of study based on whether they moved between any two of these geographical classes, resulting in six possible changes of residence: urban to rural, urban to semiurban, semiurban to urban, semiurban to rural, rural to urban and rural to semiurban. Subjects are also classified as having ‘originated’ in one of these classes based on their area of residence in 1999. Together, place of origin (urban, rural or semiurban), place of current residence (urban, rural or semiurban) and change in residence are all coded as dummy variables in our analysis. For place of origin and place of current residence, urban is used as the reference category. For change of residence, no change in residence is used as the reference category. Of these covariates, only place of origin is time invariant.
We selected demographic covariates to control for the potential confounding effect of age, sex, SES and status as an Aboriginal person based on findings from previous research.9 ,10 Data on each of these measures are maintained and regularly updated in the health insurance registry. While universal healthcare coverage is guaranteed for all residents under the Canada Health Act, over the study period Alberta charged a healthcare premium (roughly $C1400 a year for families) to help offset some of the costs of healthcare delivery. Persons below a certain level of annual income can receive a partial or full subsidy assistance to offset the costs of this fee. We use data on the level of premium subsidy to classify persons as low income or non–low income; persons with partial or full subsidy are classified as low income, and persons who pay the fee in full are classified as non-low income. In addition, persons who are classified as Aboriginal are not required to pay this subsidy and can also be identified in the health insurance registry. Age and SES status are time variant, and sex is time invariant. We also include history of attempted suicide/violent assault injury in the three years prior to 1999 as a covariate in our analysis.
Analysis
We use generalised estimating equations to model attempted suicide and violent assault injuries as a function of demographic covariates (age, sex, SES and Aboriginal status) and geographical covariates.11 Our data are longitudinal, meaning that there are multiple records for individuals in the data set. So while the data set is large, there is autocorrelation in the dependent variable due to the underlying similarity of persons to themselves over time. This dependence can affect inferences associated with model terms either overestimating or underestimating coefficient SEs. Generalised estimating equations (GEEs) are a generalisation of linear regression that includes a correction for dependence between observations by specifying the structure of and estimating this dependence explicitly in the model. This is done by fitting a generalised linear model and then iteratively refitting it with model estimated covariance parameters. Using GEEs, we address imprecision in the coefficient SE estimates by correcting for the dependence of observations in the data. We use a temporally autoregressive correction in which a single parameter (ρ) is estimated, but the correlation between observations decreases with separation in time. All analyses were performed using SAS (V.9.4).
Results
A total of 286 862 subjects were available for study, 143 431 were living in a rural region, 50 916 were living in a semiurban region and 92 515 were living in an urban region in Alberta in 1999. The median follow-up is 12 years, the mean follow-up was 10.71 years and a total of 223 770 (78.01%) of the study population was still present in Alberta as of 2010. Follow-up based on starting region was similar across the geographical groups, with 78.56% of those starting in rural regions, 79.03% of those starting in semiurban regions and 76.58% of those starting in urban regions present in Alberta as of 2010. Table 1 contains information on the measures used in the study for the years 2000 and 2010 and stratified by ever-moved and never-moved subjects based on whether or not a subject changed residence any time over the study period.
Descriptive statistics (with SE) for cohort calculated for 2000 and 2010
The first two columns in table 2 present OR estimates based on models of attempted suicide and violent assault injury with only geographical covariates. All risk estimates are of similar magnitude and sign for the two types of intentional injury, though some parameters are not statistically significant. Notably, while rural origin predicts higher risk of attempted suicide compared with urban origin, semiurban origin does not appear different from urban origin. Similarly, while semiurban residence predicts lower attempted suicide risk compared with urban residence, rural residence does not appear different from urban residence. When compared with those who have not made a recent change in residence, changes of residence between urban, rural and semiurban regions are all associated with an increased risk of attempted suicide and violent assault injury.
ORs estimated in models of injury as a function of geographical, change of residence and demographic covariates
The last two columns in table 2 present OR estimates that also include demographic covariates that may confound some of the observed geographical effects. Following the inclusion of these covariates, neither region of residence nor region of origin are statistically significant predictors of attempted suicide, and ORs are near 1. The magnitude and statistical significance of geographical covariates do not noticeably change after the inclusion of demographic covariates. Changing residence between the three geographical classes continues to predict higher risk of attempted suicide and violent assault injury, and although the model coefficients are smaller than in the previous model, all remain statistically significant. The magnitude of this effect does appear to vary somewhat depending on the origin and destination of move, with a move from urban to rural areas corresponding with the greatest increase in risk for both types of injury, and a move from rural to semiurban areas corresponding with the smallest increase in risk for both types of injury.
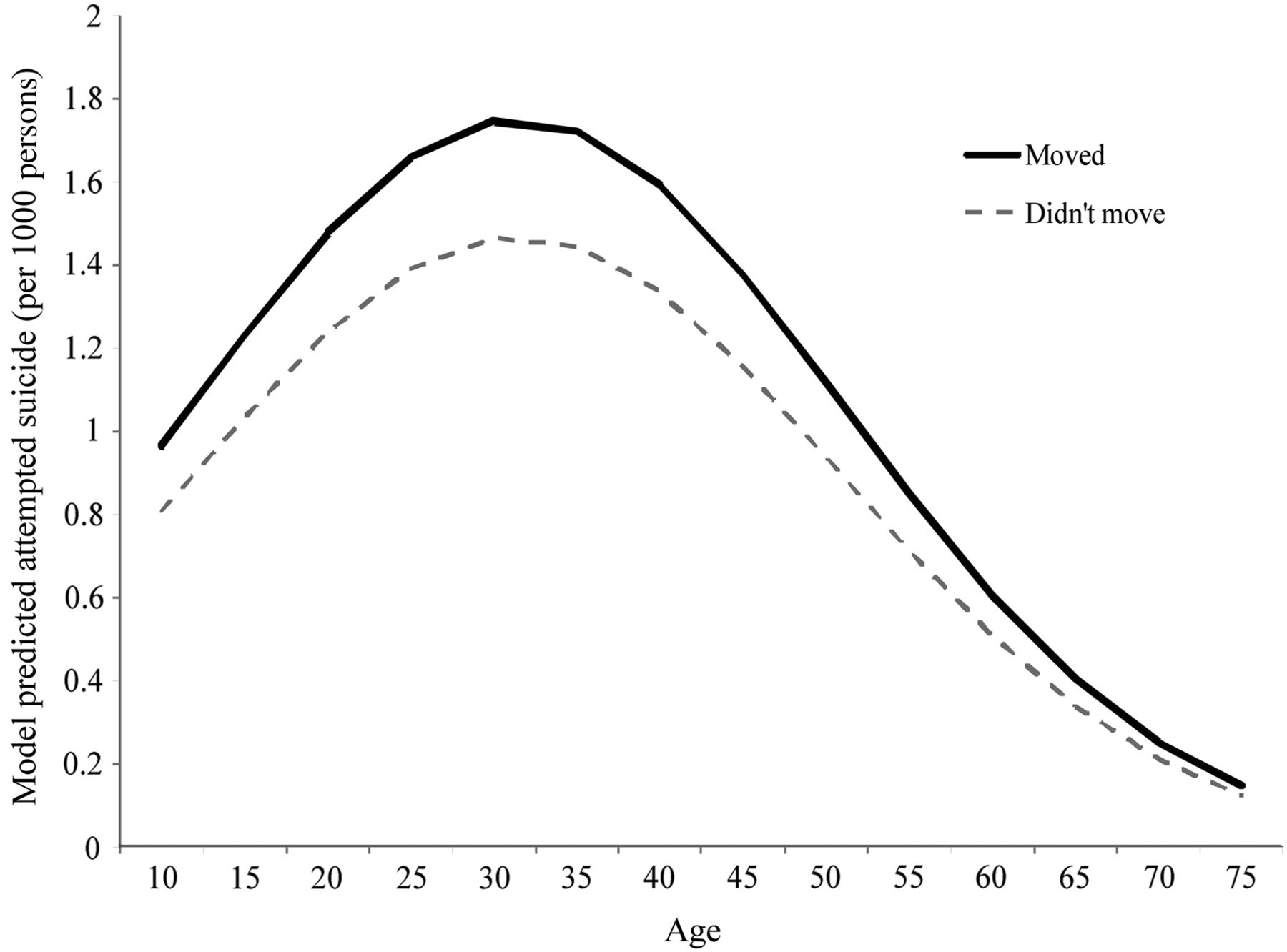
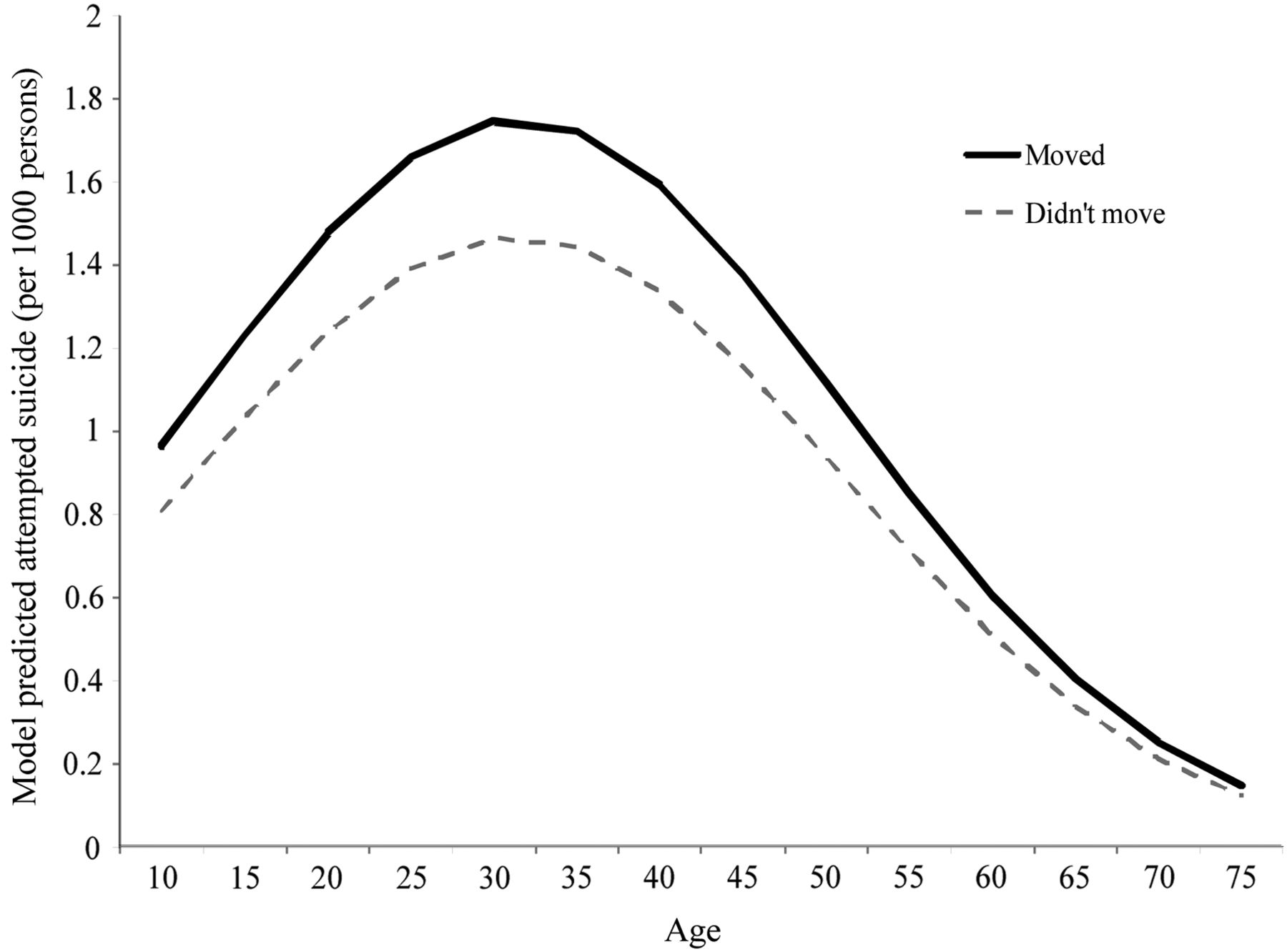
Table 3 includes the same main effects presented in table 2 but with two differences. First, the six changes of residence covariates are reduced to a single ‘moved’ covariate that represents any migration between regions. Second, the model includes interaction terms. All possible interaction effects between the demographic and geographical variables were tested and only those reaching 0.01 level of significance were retained in the model. The rural origin by female interaction in predicting violent assault injury is relatively straightforward to interpret; rural origin is associated with higher risk of violent assault injury and female sex is associated with a lower risk of violent assault injury, but being female with origins in rural areas is associated with a further increase in risk independent of the additive effect of these two terms. The moved by age interaction is harder to interpret with coefficients alone. Figure 1 displays the nature of this interaction visually by graphing the risk per 1000 persons as a function of age holding other parameters constant. Having moved recently between an urban, semiurban or rural area is associated with a higher risk of attempted suicide for persons under 75 years of age, but the contrast in risk is highest for those persons between 20 and 35 years of age.
ORs estimated in final models of injury as a function of geographical, change of residence, demographic covariates and interactions
{kind=link}
Interaction between changing residence and age in predicting attempted suicide.
Discussion
Considerable research has shown regional variability in fatal and non-fatal intentional injury.12–17 Suicide is typically more common in rural than urban regions, particularly among males and independent of access to mental health services.12 ,15 ,18 ,19 An urban–rural contrast in attempted suicide risk has also been reported, with some evidence of higher risk in urban regions and some evidence of the opposite.12 ,20 In contrast, our results suggest that after controlling for measures like age, income, sex and status as an Aboriginal person, there is little variation in attempted suicide risk between urban, rural and semiurban regions of Alberta.
However, our results suggest an independent association between changing residence and the risk of attempted suicide; in any given year, a change in residence between urban, semiurban or rural areas is associated with an increase in the risk of attempted suicide. Notably, the interaction effects suggest that much of this association corresponds to persons of younger ages, with the peak difference between those who change residence and those who do not in the 20–35 years of age range. Many life stressors are common at these ages, such as attending postsecondary education institutions and finding work.21 ,22 The result may also reveal the importance of social support as a protection against attempted suicide. Social support has an important protective role in reducing suicide ideation and suicide.23–26 Changes of residence may correspond to a period of adjustment in which a new resident has yet to identify support systems to help manage the challenges of their lives. For young adults in particular, moving to a new area may involve leaving family and could lead to feelings of isolation and loneliness; this observation has been made for international students, who seem to use social support to manage external pressures related to school, finances and cultural adaptation.27 ,28 Our findings build on these observations, suggesting that similar to international migration, absence of social support among regional migrants may also have an adverse effect on the well-being of young people.
Violent assault injuries are more common than attempted suicide in these data and have equivalent, if not stronger, associations with the geographical covariates. Indeed, the geographical differences in rates of violent assault injuries remain even after inclusion of the demographic covariates, though in an interesting way. Starting out in a rural or semiurban region is associated with higher risk of violent assault injury than starting out in an urban region, but current residence in an urban region is associated with a higher risk of violent assault injury than living in a rural or semiurban region. Together, this suggests that persons originally from rural regions that move to urban regions have the highest risk of violent assault injuries and that persons from urban regions that move to rural or semiurban regions have the lowest risk, all else being equal. The magnitude of this difference in risk is not trivial; there is a >50% increase in model predicted risk of violent assault injury for urban residents originally from a rural area compared with rural residents originally from an urban area. Our results also suggest that women with rural origins may experience higher risk of violent assault injury than women with urban origins irrespective of current place of residence. This demographic–geographical interaction effect is not present in men and partly offsets the overall lower risk of violent assault injury in women.
As with attempted suicide, the mechanism underlying the association between changing residence and violent assault injury risk may be related to an absence of social support for newcomers. There is some evidence linking the perception of neighbourhood social capital to fear of violent assault, and considerable evidence that violence is strongly associated with income inequality.29–33 However, much of this research is based on an assessment of the social capital within a place or region rather than the interaction between a person's need for social support and sense of community engagement and the level of social capital in a community. Our findings suggest that much like international migrants, intraregional migrants may also require time to benefit from the protective social effects community.
For both attempted suicide and violent assault injuries, moving to a rural area is associated with larger increases in risk than any other change in residence observed. We note that these are the least frequent movers in our study (most migration is rural to urban not the other way around), and as a result, the total public health impact of these risks is comparatively small. Nevertheless, our observations are consistent with research that suggests moving to rural environments may increase geographical and interpersonal isolation.34 ,35 Our findings also suggest that the change from urban to rural may exacerbate the already higher risks of intentional injuries in rural areas.
Finally, while not the focus of this study specifically, we note the strong relationship between Aboriginal status and intentional injury, effects also observed in other research.36 ,37 The magnitude of these effects reinforces other observations that structural challenges that Aboriginal persons face merit meaningful engagement and action from the community, academia and government.
Limitations
A noteworthy limitation of this study is that some of the observed relationship may be due to reverse causation—injury influences the likelihood of intraregional migration rather than the other way around. It may be that some or much of the association implies that people who are at higher risk of intentional injury are more inclined to change residence. However, while our findings should be interpreted with caution, we would suggest that our favoured interpretation—migration is associated with reduced social support and increased injury risk—is most consistent with the literature linking length of residence to social support and the relationship between social support and risk of intentional injury.23 ,24 ,29 ,38
We very likely underestimate the association between migration and injury risk since we do not account for the effect of change within urban, rural and semiurban environments themselves. It is possible that a move from one side of the city to another may present similar challenges to social support as a move between a semiurban and urban area, for example. Part of the challenge of this effect is that it is likely mediated by factors like access to a motor vehicle and public transit, and even lifestyle factors that are difficult to measure. In this study, we lacked the detailed geographical information to analyse data at the scale required for this analysis, but our results suggest that such research may be worth conducting in the future.
Finally, it is possible that subjects that did not remain in the cohort through the entire study period may have exited the cohort because of factors associated with the study—specifically death due to homicide or suicide, or moving out of the province. Removal from the cohort as a result of death could attenuate results since our analysis would very likely exclude persons who died as a result of intentional injury. Similarly, if the relationship between moving out of province and intentional injury is the same as the relationship between moving with the province and intentional injury, this could also attenuate observed effects. Given that nearly 80% of the cohort remained in the data set for the study period, we suspect the magnitude of these effects is probably small.
Conclusion
Our results suggest that intraregional migration is associated with the risk of intentional injuries independent of demographic factors and geographical differences between urban, rural and semiurban areas. Future research may benefit from investigating a broadening of community integration programmes to include both international and intranational migrants. Our findings also highlight the importance of drawing a distinction between how a geographical process—like changing place of residence—is important for understanding health independent of social and physical environments themselves. Such processes are difficult to study in the absence of longitudinal data, but when possible can help advance a deeper understanding of the interactions between places and people.
What is already known on the subject
International migration is associated with changes in health.
Changing community of residence can cause anxiety and stress.
What this study adds
Regional migration is associated with increased risk of intentional injury.
Urban–rural differences in intentional injury risk are small after controlling for demographic risk factors.
Acknowledgments
The data used in this study were provided by Alberta Health.
References
Footnotes
Disclaimer The interpretation and conclusions contained herein are those of the researchers and do not necessarily represents the views of the Government of Alberta or Alberta Health.
Competing interests None declared.
Ethics approval The Research Ethics Office at the University of Alberta (protocol Pro00015547).
Provenance and peer review Not commissioned; externally peer reviewed.