Article Text

Abstract
Introduction Participation in falls prevention activities by older people following presentation to the emergency department (ED) with a fall is suboptimal. This randomised controlled trial (RCT) will test the RESPOND programme, an intervention designed to improve older persons’ participation in falls prevention activities through delivery of patient-centred education and behaviour change strategies.
Design and setting A RCT at two tertiary referral EDs in Melbourne and Perth, Australia.
Participants 528 community-dwelling people aged 60–90 years presenting to the ED with a fall and discharged home will be recruited. People who require an interpreter or hands-on assistance to walk; live in residential aged care or >50 km from the trial hospital; have terminal illness, cognitive impairment, documented aggressive behaviour or a history of psychosis; are receiving palliative care or are unable to use a telephone will be excluded.
Methods Participants will be randomly allocated to the RESPOND intervention or standard care control group. RESPOND incorporates (1) a home-based risk factor assessment; (2) education, coaching, goal setting and follow-up telephone support for management of one or more of four risk factors with evidence of effective interventions and (3) healthcare provider communication and community linkage delivered over 6 months. Primary outcomes are falls and fall injuries per person-year.
Discussion RESPOND builds on prior falls prevention learnings and aims to help individuals make guided decisions about how they will manage their falls risk. Patient-centred models have been successfully trialled in chronic and cardiovascular disease; however, evidence to support this approach in falls prevention is limited.
Trial registration number The protocol for this study is registered with the Australian New Zealand Clinical Trials Registry (ACTRN12614000336684).
Statistics from Altmetric.com
Background
Falls are one of the leading causes for emergency department (ED) presentations in older people.1 In the 6 months following an index fall ED presentation, up to 52% of cases experience subsequent falls,2 ,3 49% are re-hospitalised and many experience functional decline.2
There is conflicting evidence surrounding the effect of programmes designed to reduce secondary falls in older people presenting to the ED with a fall. Eight studies have reported programmes that had no effect on new falls, fall injuries or ED presentations,4–11 while three reported programmes reduced secondary falls.3 ,12 ,13 The characteristics that appear to differentiate successful programmes from others include delivery of the intervention within 1 month of the index fall and greater intensity of the interventions.14 An Australian randomised controlled trial (RCT) of older people attending the ED after a fall reported that for patients who accessed falls prevention services recommended by project staff after baseline assessment (an average of 28 days after ED presentation), the time lag to service access was too long—4 months for falls clinics, 2 months for physiotherapy and 3 months for occupational therapy.4 Similar delays were reported in a Dutch RCT that used an interdisciplinary intervention6 and a Danish RCT, where the time lag from fall to intervention was 7 weeks.15 In contrast, a successful UK trial delivered services within 1 month of ED discharge.12
Poor patient participation in falls prevention activities also appears to be an important factor underpinning the effectiveness of prior programmes and may be related to care not centring on what the patient perceives as being important.16 ,17 The Australian RCT cited <5% of people presenting the ED with a fall subsequently attend falls clinics, <30% attend physiotherapy and <17% attend occupational therapy.4 These findings of limited patient participation in prevention activities are consistent with an Australian qualitative study that reported that 72% of patients (with a fall-related ED presentation) were reluctant to attend exercise classes, 59% were hesitant to cease psychotropic medications and 43% were unwilling to have a home safety assessment.16 Conversely, older people see relevance in falls prevention strategies that adopt a patient-centred approach by including education and involvement in decision making.18 Guidelines to increase uptake of falls prevention strategies have also suggested older adults choose activities that have personal meaning and are compatible with their social norms.19
Patient-centred care models have been successfully trialled in chronic disease and secondary prevention of cardiovascular events.20 ,21 A RCT of 144 patients with acute coronary syndrome tested the ‘Choice of Health Options In prevention of Cardiovascular Events (CHOICE)’ programme. CHOICE showed that a brief patient-centred programme comprising a clinic visit and telephone support resulted in significant improvement in cardiac risk profiles compared with profiles of patients receiving standard care.21 Importantly, a follow-up study found CHOICE participants maintained favourable changes in coronary risk profile at 4 years compared with controls, indicating that a brief patient-centred programme with telephone support is an effective long-term intervention.22
Incorporating patient-centred care principles and telephone support into falls prevention programmes may improve participation in falls prevention strategies. This approach is supported by a recent review that reported participation in falls prevention strategies was highest in studies that offered moderate home visit support and intervention via telephone contact, where moderate support was defined as less than one home visit or telephone call per month and more than two home visits in total.23 Presenting information as positive health messages or as ‘life enhancing’ rather than ‘at risk’ may also improve participation.19
The efficacy of patient-centred falls prevention programmes that include education and coaching via positive health messages to address falls risk factors has not been previously reported. The current study will address this evidence gap by investigating the impact of a patient-centred falls prevention programme—RESPOND—on the rate of falls, fall injuries and ED re-presentations in older people presenting to the ED with a fall. The objectives of this paper are to describe the protocol for this trial.
Methods
Design
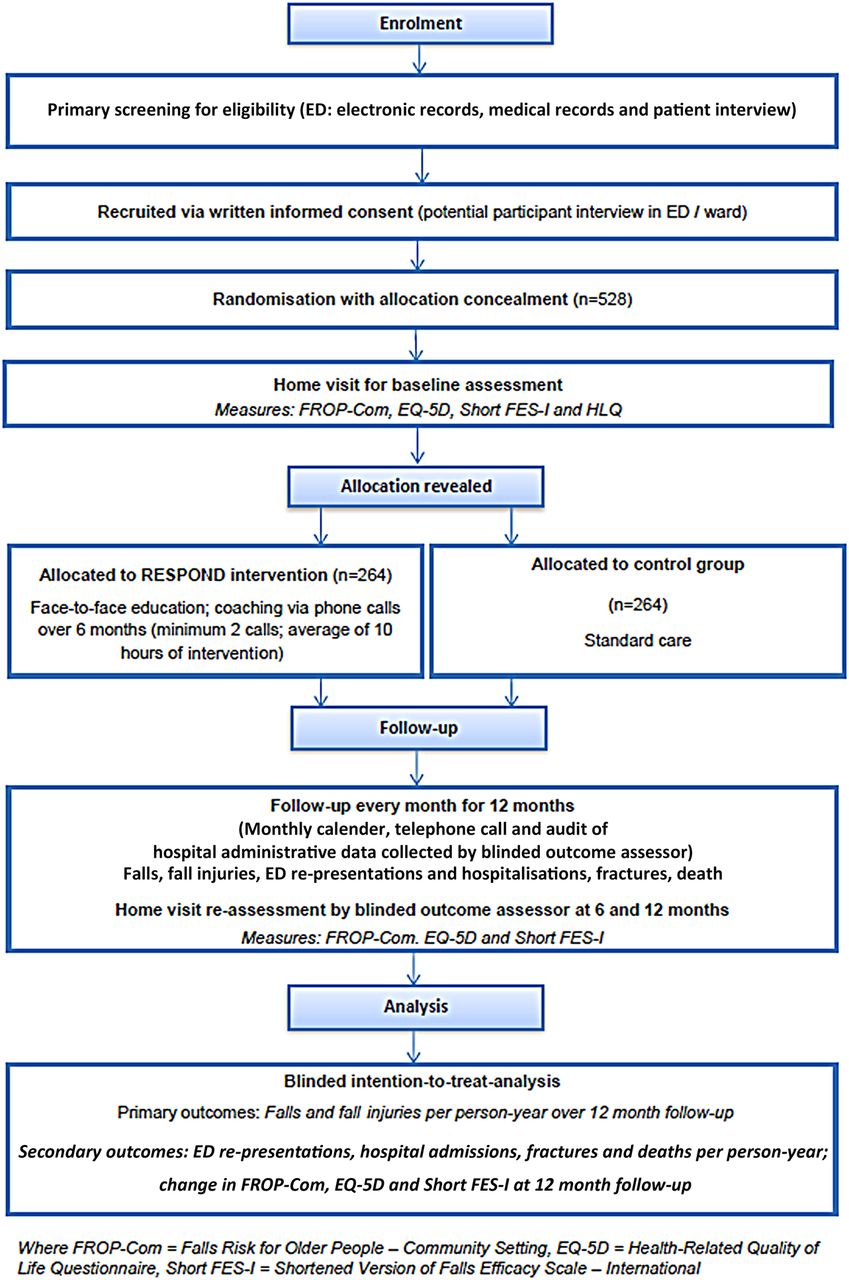
A single-blind multicentre RCT of the RESPOND programme compared with falls risk assessment and standard postdischarge care will be conducted. Figure 1 outlines each step of the study.

Participant flow.
Participants and setting
Community-dwelling persons aged 60–90 years who present over a 12-month period to two large, metropolitan, tertiary referral major trauma centre EDs with a fall and who are planned to be discharged directly home from the hospital within 72 h will be recruited during their hospital stay. This study targets patients who are planned to have a short inpatient stay as these people are least likely to receive comprehensive geriatric assessment and management and would therefore be at greater risk of secondary falls than patients hospitalised for longer periods or discharged to rehabilitation services.
Exclusion criteria relate to an inability to participate in the intervention and include discharge to residential aged care, current palliative care or terminal illness, requiring hands-on assistance to walk, being unable to use a telephone, needing an interpreter and presence of cognitive impairment, social aggression or a history of psychoses. As a reflection of study constraints around home visits, people living further than 50 km from the trial hospital will also be ineligible to participate.
Sample size
The study is powered to detect a significant difference in the primary outcome of the rate of falls and fall injuries between the intervention and control groups in the 12-month follow-up. Assuming a control group fall injury rate of 1.01 injuries per person-year,4 we require 293 participants to have 80% power to detect a rate ratio of 0.70 between intervention and control groups at the 5% (z=2.8) significance level. To allow for a 20% loss to follow-up4 and over-dispersion (φ=1.5) 528 participants (n=264 per group) are required. The study will be adequately powered to detect differences in ED re-presentations in the 12-month follow-up based on an expected control rate of 0.71 per person-year,4 and 80% power to detect a rate ratio of 0.70 between intervention and control groups at the 5% significance level (N required=502).
Recruitment
A three-stage process will be used by research staff to identify eligible participants. Stage 1 involves screening electronic records on a daily basis in the ED to identify potential participants based on age, living status (home as opposed to residential aged care), presenting diagnosis and distance of home from the hospital. Stage 2 involves review of medical records of persons meeting stage 1 screening requirements to determine those who meet the inclusion criteria of planned discharge home within 72 h and to exclude people who have a documented life expectancy of 12 months or less, are receiving palliative care or have a history of social aggression or psychoses. Stage 3 involves approaching people meeting stage 2 screening requirements to obtain verbal consent to conduct a screening interview. During the interaction, the research staff will determine whether the individual requires an interpreter, is able to use the telephone, has a hearing impairment or requires physical assistance from another person to walk. Cognitive ability will be determined by the Mini Mental State Examination (MMSE)24 applying a cut-off score of <23. Potential participants who have a physical impairment or injury that limits upper limb function will have the MMSE score adjusted as per the tool's handbook.25
Eligible participants at this stage will be provided with an overview of the study including written information about the study and asked to provide written consent to participate.
Randomisation
After receipt of informed written consent, participants will be randomly assigned into one of the two trial groups. A web-based randomisation sequence will be used, with permuted block randomisation stratified by recruitment site to ensure equal control and intervention participant numbers across sites. Research staff will be unaware of the next group allocation at the time that they request a participant's group assignment. The participants and research staff will be blinded to group allocation until after the baseline assessment has been completed.
Baseline assessment
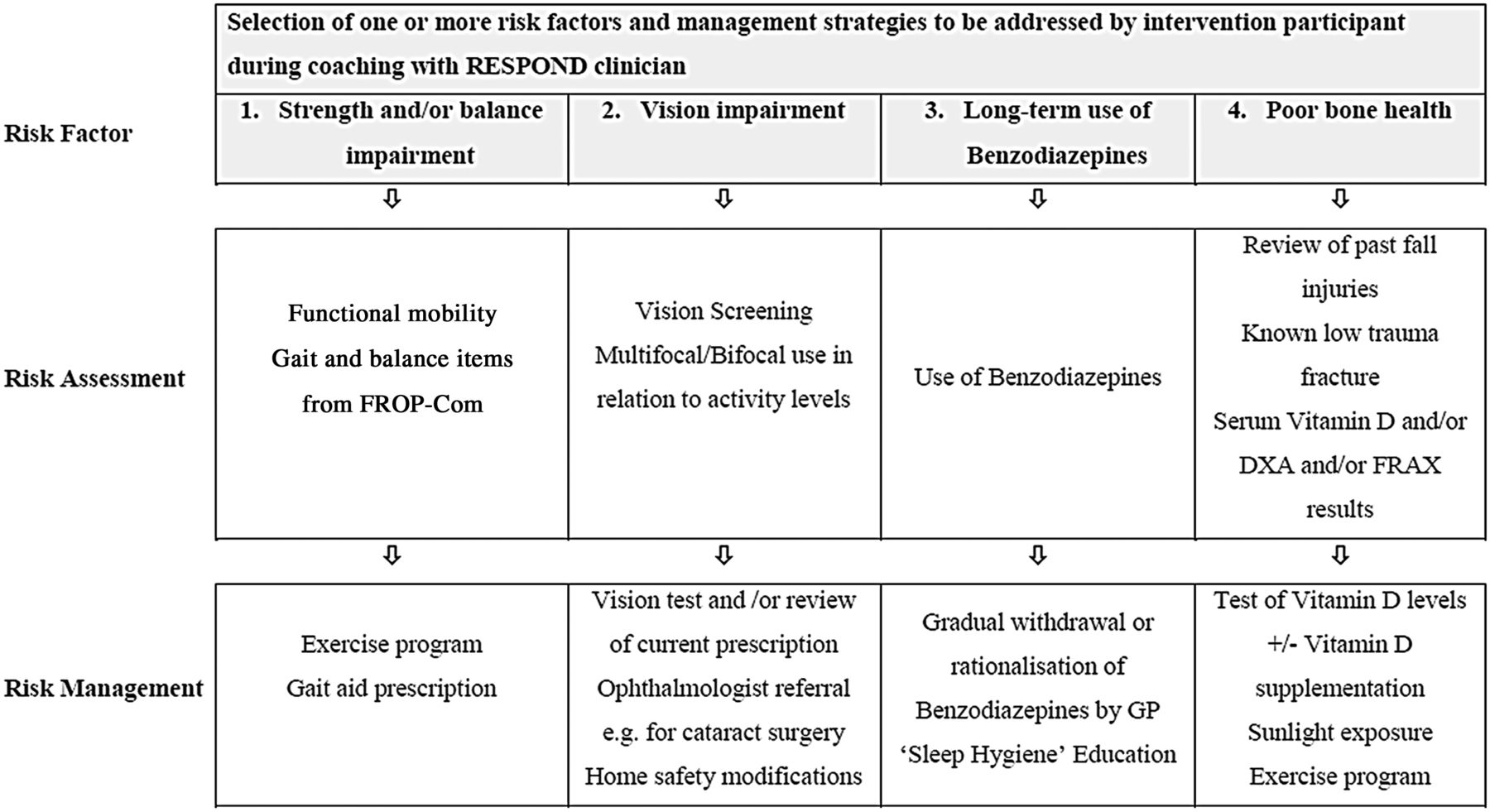
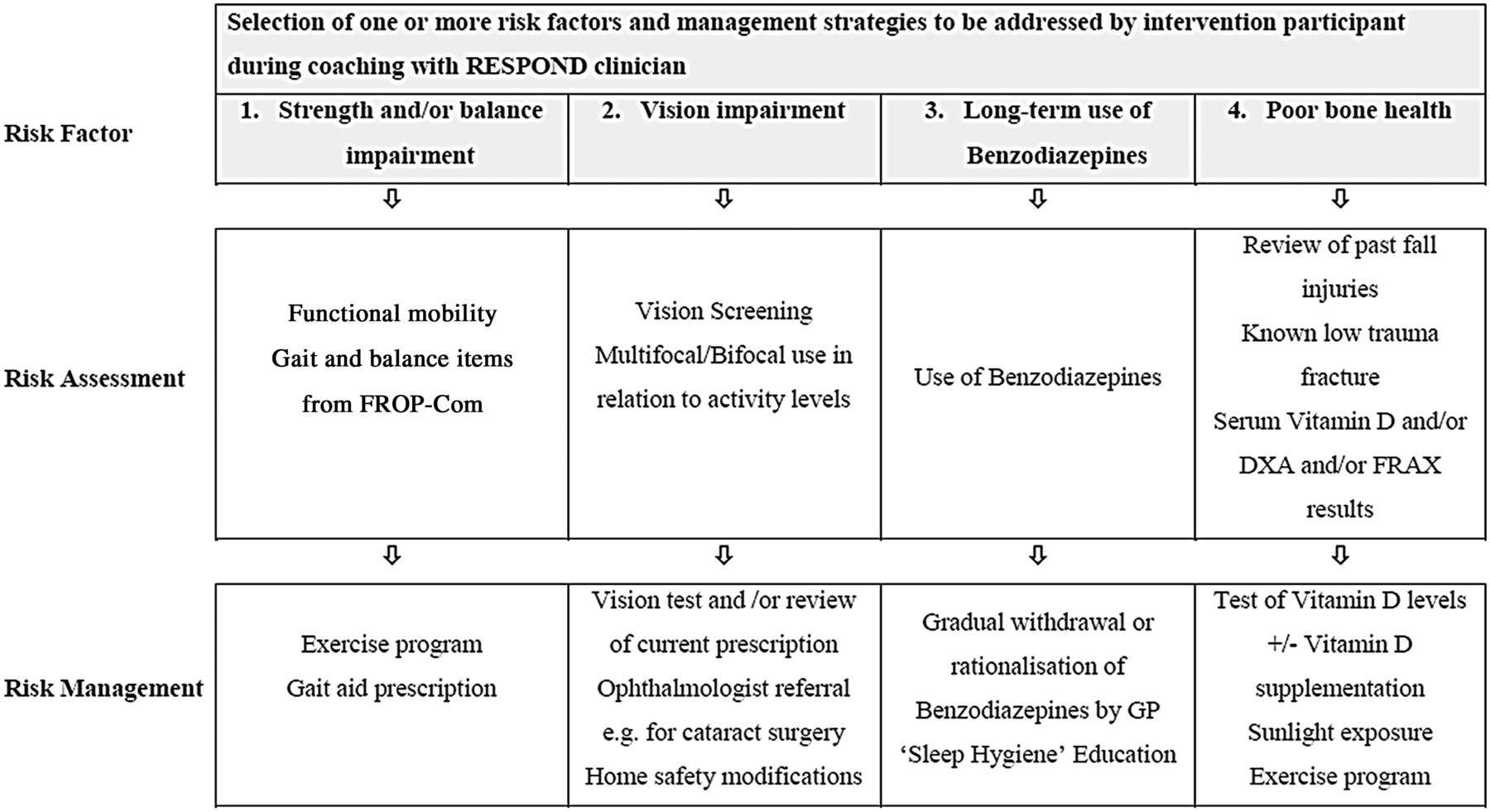
The next phase of the study is conducted by the RESPOND clinician—a registered healthcare professional, who will visit the participant at their home within 2 weeks of discharge from hospital. At this visit, data will be collected relating to demographic details, social history, index and past fall history, existing referrals and any clinical recommendations made by hospital staff. A falls risk factor assessment will be completed and falls self-efficacy, functional health literacy and health-related quality of life will also be evaluated (figure 2).
{kind=link}
{kind=link}
RESPOND risk factor assessment and management foci.
The Falls Risk for Older People in the Community (FROP-Com) assessment will be used to assess falls risk factors and risk status (low, medium, or high falls risk). This tool includes 28 questions on 13 risk factors that have either dichotomous or ordinal scoring from 0 to 3. A total score out of 60 is obtained with higher scores indicative of greater risk.5 ,26 High inter-rater and intra-rater reliability has been reported as has a moderate accuracy to predict those at risk of future falls.5 ,26
Functional health literacy will be assessed using the Health Literacy Questionnaire (HLQ), a tool that includes nine conceptually distinct areas of health literacy and has been demonstrated to possess robust psychometric properties.27 Health-related quality of life will be assessed using the EQ-5D, a utility-based quality-of-life instrument that estimates quality-adjusted life years and provides a single value for health-related quality of life.28 ,29 Falls self-efficacy will be assessed using the Falls Efficacy Scale—International (short version) (Short FES-I).30 This seven-item tool measures the level of concern about falling during social and physical activities inside and outside the home and has been shown to be a reliable and valid measure of fear of falling in older people.31
The baseline assessment will be conducted in a standard way to minimise the likelihood that it could influence behaviour change in control participants. A simple written report including the participants falls risk status (low, medium or high falls risk) based on the FROP-Com score will be sent to each participant's general practitioner (GP) following baseline assessment. If the participant scored ‘moderate or severe anxiety or depression’ on the EQ-5D, this information will also be included on the letter. All letters to the GP will be countersigned by a study geriatrician.
Intervention
The RESPOND programme will be implemented by the RESPOND clinicians over a 6-month period. Table 1 describes the intervention according to the CONSORT extension Template for Intervention Description and Replication guidelines (TIDieR).32
Intervention description as per TIDieR32
The RESPOND clinician will explore participant's falls knowledge, beliefs and self-efficacy to assist in the selection of options for management. The focus will be on participant choice and engagement. Risk factor goals will be based on each participant's individual risk factor profile, social factors, work and/or family commitments and summarised into an individualised action plan. Motivational interviewing will be used to support the participant to understand assessment findings and to facilitate them in making guided decisions about how they will action recommendations and referrals. Clinicians will also assist in identifying solutions to barriers identified by participants.
The RESPOND clinician will not duplicate care provided by other healthcare professionals involved in the participants care during the 6-month intervention period. The RESPOND clinician assessment will capture existing care recommendations and healthcare professionals involved in the participants care. RESPOND clinicians will refer intervention participants to relevant services and facilitate community linkages.
The participant's ongoing consultation with GPs and specialist physicians over the course of the study will be encouraged. As part of the study intervention, the RESPOND clinician will communicate the individualised action plan to the participant's healthcare providers and any community services the participant is linked into.
The comparator
Participants in the control group will receive the same baseline assessment as outlined above. A letter detailing the participants risk status will be provided by the assessing clinician to the control participant's GP following the baseline assessment. Where the participant indicates moderate or severe anxiety or depression on the EQ-5D, this will be communicated in the GP letter. Control participants will receive standard care from all health professionals who are involved in their management within the ED and in the primary care setting during the 12-month follow-up. No treatments will be withheld from the control group. Care in the ED may consist of investigations and multidisciplinary assessment within the ED, referral to other health professionals and services, and postdischarge telephone contact by a nurse. Control participants will not receive any coaching phone calls or other contact from the RESPOND clinician after the baseline assessment.
Outcome measures
Table 2 outlines the primary and secondary outcomes for this trial, and the timing of their collection. The primary outcomes are falls and fall injuries per person-year in the 12 months after recruitment. A fall will be defined as per the World Health Organisation (WHO), “an event resulting in a person coming to rest inadvertently on the ground, floor or other lower level”.33 A fall injury is any physical harm resulting from a fall reported by study participants on the monthly calendars or during monthly telephone calls. Where participants suffer multiple injuries from one fall, all injuries will be included in the outcome analysis irrespective of their severity.
RESPOND outcome measures and key covariates collected at study time points
Secondary outcomes are ED re-presentations, hospitalisations, fractures (confirmed by radiological investigation) and deaths per-person year in the 12 months post randomisation. Change in falls risk status, falls self-efficacy and health-related quality of life in the 12 months post randomisation will also be evaluated.
Data collection
Hospital admitted episode and ED administrative data will be audited to obtain the number of potentially eligible study participants, participant demographics and diagnoses, and ED re-presentations and hospitalisations that occur during the follow-up.
Participants in both groups of the trial will complete monthly calendars over the 12-month follow-up documenting details of any falls, fall injuries, ED presentations and hospital admissions on a daily basis. Calendars will be returned monthly by participants using prepaid envelopes. All participants will receive a monthly telephone call to verify information recorded on calendars. This will be conducted by RESPOND outcome assessors who will be blinded to participants’ group allocation. Calendar and telephone-verified data on falls, fall injuries, fractures, ED presentations and hospital admissions will be triangulated with data recorded in hospital administrative data sets.
Adverse events spontaneously reported by participants to research staff will be reported to the study steering committee for evaluation.
Statistical analysis
Outcome analyses will be undertaken on an intention-to-treat basis by a statistician blinded to group allocation. Differences in falls, fall injuries, fractures, ED re-presentation rates and deaths will be compared between groups using negative binomial regression including a variable for adjustment by site. Secondary analysis that adjusts for age and cognitive ability (using FROP-Com cognitive status score obtained at baseline assessment) will be undertaken if significant imbalance in these factors is identified across groups. Differences in continuous outcomes including falls risk, quality of life and falls efficacy scores will be evaluated using General Linear Models (ANCOVA) or the non-parametric Mann–Whitney U statistic where data are not normally distributed. A significance level of p<0.05 will be used for all analyses. The multifactorial design (participants will choose different risk factors and strategies) means it is not possible to discern the effects of any single intervention on the primary outcomes.
Elements introduced to mitigate bias in the study include use of a computer randomisation service and outcome assessment and intention-to-treat analysis performed by staff blinded to participant's group allocation.
Ethics approval
Ethics approval was obtained from each of the participating hospitals, Alfred Health (HREC 439/13) and Royal Perth Hospital (REG 13-128) and Monash University Human Research Ethics Committee (MUHREC CF13/3869-201300).
Discussion
This RCT will develop and test a patient-centred programme—RESPOND—that aims to support older people in making decisions about how they will manage their falls risk. The intervention will assist participants to participate in falls prevention activities by providing education, coaching, referral to services they need and ongoing telephone support to provide positive reinforcement and to troubleshoot barriers that are identified.
Patient-centred models have been successfully trialled in chronic disease20 and secondary prevention of cardiovascular events. The RESPOND programme draws its conceptual framework from the experience with CHOICE and builds on our previous work addressing patient participation in falls prevention activities.34–39 RESPOND will include additional tailoring to the frailer client group who are likely to be the majority of the study sample.
This study design is supported by extensive standard operating procedures (SOPs) developed for the recruiters, clinicians and outcome assessors at each stage of the study. In order to prevent contamination, strategies have been included in the SOPs to ensure that study staff and standard care practitioners do not influence the behaviour of participants in the control group. The main contamination threat to the control group lies in ED staff incorporating some of the intervention strategies into standard care practices. Recruiters have been specifically trained not to flag participants to ED staff and to minimise discussion about potential participants. Randomisation will be concealed from all study staff until after the baseline assessment has been completed and from the outcome assessors and study statistician for the study duration.
A potential source of contamination is provision of information about falls risk to the control participant's GP. While we can argue that this will not change their behaviour, it is not ‘usual care’ and a failure to show a difference between study groups may be due to individual GPs acting on the information provided about control participants by RESPOND staff.
The study internal validity is strengthened by the inclusion of competency checks for staff adherence to operating procedures. Staff across both study sites will be trained by the same instructor using reference to the SOPs and tools to ensure identical data collection practices. Performance indicators have been developed for each of the study roles (ie, recruiter, clinician, outcome assessor) and compliance with SOPs will be verified by quality audits at each stage of the study.
Since recall bias has the potential to limit accuracy of data, this study has applied current best practice recommendations for identifying fall events, which involves the use of multiple methods for the capture of falls data.40 Participants will record fall events prospectively in a study calendar, rather than relying on recollection at follow-up time points, and this information will be verified by outcome assessors during the monthly phone calls. Fall injuries that result in an ED hospital presentation will be triangulated with hospital administrative data. Participants with cognitive impairment have been excluded to minimise bias associated with memory impairment.
Our findings will generate new knowledge on strategies to enhance care of older people who present to the ED after a fall and who are likely to fall again. However, findings may not be generalisable to all community-dwelling older people who fall, or to frail older people who are in residential aged care.
The project will also investigate the cost-effectiveness, acceptability and sustainability of the RESPOND programme, as well as participant knowledge, attitudes and beliefs surrounding participation in falls prevention activities. These investigations have detailed methodology in addition to that reported here and will be described in subsequent protocols.
The research outcomes have the potential to change current falls prevention practice and policies for older people presenting to an ED with a fall. The findings from this project could impact on the planning, design, implementation and management of secondary falls prevention programmes in Australia and internationally.
Acknowledgments
We thank Dr Gayle Savige for assistance in preparing this manuscript for publication and the representatives from our funding partner organisations who have contributed to development and implementation of this study. The partner organisations include
1. Health Strategy and Networks Branch, Strategic System Policy and Planning, Department of Health, WA
2. Aged and Continuing Care Directorate, Department of Health, WA
3. Royal Perth Hospital
4. Curtin University of Technology
5. The University of Western Australia
6. The Royal Perth Hospital Medical Research Foundation
7. Sir Charles Gairdner Hospital (SCGH) Area Rehabilitation and Aged Care Falls Specialist Program
8. Injury Control Council of Western Australia (ICCWA)
9. The George Institute for Global Health
10. The Alfred Hospital
11. Monash University
12. Integrated Care, Victorian Department of Health
References
Footnotes
-
Contributors All authors provided substantial contribution to conception and design of the project, drafting the article and revising it critically for important intellectual content; and final approval of the version to be published. AB led the drafting of all sections of the article in consultation with all of the co-authors. KH, JR and SN provided substantial contributions to the background, critical appraisal of prior studies and rationale for the project. PC, GA, JL, PH, DS and AF provided substantial contribution to the design of the recruitment processes. CB, NW, SN, LF, JR, A-MH and CEB provided substantial contribution to the intervention design. KH, CB, TH, AF, JR and JL provided substantial contribution to the overall design aspects including selection of outcome measures and refinement of study processes. AB and AF provided substantial contribution to the sample size and statistical analysis section.
-
Funding This project is funded under the Australian National Health and Medical Research Council (NHMRC) Partnership Projects funding scheme (project number APP1056802) with financial and in-kind contributions from the partner organisations listed above. AB is funded by a Career Development Fellowship funded by the NHMRC (1067236), JR is funded by a Postdoctoral Fellowship co-funded by the NHMRC and National Heart Foundation (632933) and JAL is funded by an Early Career Fellowship funded by the NHMRC (1052442).
-
Competing interests None.
-
Ethics approval The Alfred Hospital Ethics Committee; Royal Perth Hospital Human Research Ethics Committee; Monash University Human Research Ethics Committee.
-
Provenance and peer review Not commissioned; externally peer reviewed.