Article Text

Abstract
Objective: To investigate the effectiveness of a paraprofessional home visitation program (HVP) to improve home safety and prevent injuries among children living in low-income settings.
Methods: The HVP was implemented in two low-income communities in South Africa. In each community, approximately 200 households were randomly selected for the trial. Eligible households were those with children aged ⩽10 years. Intervention households received four visits, one every two weeks, by trained paraprofessionals that focused on a specific injury topic and consisted of: information dissemination about specific injury prevention practices; home inspection accompanied by information about home hazards; and the supply of safety devices. The key outcomes to measure the presence of home hazards were scores for burns (safety practices, paraffin, and electrical), poisoning, and falls.
Results: Significant reductions were found for injury risks related to burn safety practices. For injury risks related to electrical burns, paraffin burns, and poisoning, a decline was also noted although this was not statistically significant. No decline was noted for fall-related risks.
Conclusions: Subject to further replication and evaluation, home visits by paraprofessionals providing safety education, home inspection, and safety devices be considered for integration into a comprehensive child injury prevention strategy in low-income communities.
Statistics from Altmetric.com
Unintentional injury, a major cause of morbidity and mortality for children worldwide, is concentrated in low- to middle-income countries (LMICs).1 Despite the growing rate of childhood unintentional injury in LMICs, effective prevention and control remain inadequate due to the lack of resources and expertise.23
In South Africa, children aged 14 and younger, who make up a third of the 44.8 million population, account for 8% of the annual non-natural deaths (estimated at 70 000) that predominantly arise from motor vehicle, pedestrian, and burn injuries.45 Motor vehicle and pedestrian injuries, burns, falls, and poison ingestion are the leading causes of non-fatal injuries among children.6–9 While traffic-related injuries are more prevalent among older children (10–14 years), burns, poisoning, and fall-related injuries are more common among young children (<10 years).9
Developmental achievements such as independent mobility and exploratory behavior increase exposure to hazards in the home among children who have not developed the ability to avoid danger.210 Environmental factors also contribute to children’s vulnerability to injuries.2 Studies worldwide reveal that children living in poorer neighborhoods are more often the victims of unintentional injuries than those living in more affluent areas.11–15 In South Africa, injuries in general are concentrated in low-income neighborhoods characterized by a lack of infrastructure, resources, overcrowding, unemployment, and poverty.1617 Similar to impoverished communities in other LMICs in Africa, Asia, and Latin America, challenging living conditions such as poor housing, the lack of demarcations for cooking or washing areas, inadequate recreation space, the use of open fires and paraffin stoves, and the lack of safe storage for paraffin and other harmful substances are among the major hazards that place children at risk for burns, poisoning, and fall-related injuries in South Africa.21116–18
Community-based interventions that include efforts to reduce household hazards could contribute to the reduction of child unintentional injuries. Home visiting programs conducted in high-income countries (HICs) have shown improved parental safety knowledge, reduced prevalence of home hazards, and reduced rates of child unintentional injury.19–22 Interventions such as education on specific injury prevention practices, home inspections accompanied by information about home hazards, and the supply of safety devices are provided through home visits by doctors, nurses, school personnel, and non-professional community workers.1922–24 A meta-analysis revealed that home safety education, especially when coupled with the provision of safety equipment, was effective in increasing a range of safety practices associated with the prevention of burns, poisoning, and fall-related injuries.25 There is however, little evidence regarding the effectiveness of home visiting programs to reduce home-centered child injury hazards in LMICs.
In response to the child injury problem in South Africa and as an attempt to generate local intervention data, the authors designed and implemented a home visiting program (HVP) in specific low-income neighborhoods. The project design, implementation plan, and ethics were reviewed and approved by an independent review panel commissioned by the agency implementing the project; the panel met in 2002 and comprised experts from three South African universities.
Lay community workers, residents of the study communities, were employed on the assumption that they could provide a cost-effective strategy for child unintentional injury prevention, and add value to the program as they could deliver the interventions in a culturally sensitive and appropriate manner by virtue of their intimate understanding of the target community.326–28 This article presents the results of a cluster randomized controlled trial evaluating the effectiveness of the HVP on the reduction of household hazards for burns, poison ingestion, and fall-related injuries among children aged ⩽10 years.
METHODS
Study sites and participants
Households with children aged ⩽10 years were initially recruited from four low-income communities, Vlakfontein, Slovo Park, and Eldorado Park (near Johannesburg), and Nomzamo (near Cape Town) to participate in a pilot HVP. Children in these and similar settings are reported to be at high risk to unintentional burns, poison ingestion, and fall-related injuries, most of which occur in and around the home.2589 The pilot study indicated that successful implementation of the HVP is contingent on household receptivity and trust, and a cohesive home visitation team. Accordingly, the final trial was implemented in Slovo Park and Nomzamo where such factors were evident. Both areas are informal settlements established in the early 1990s and consist predominantly of temporary wood and corrugated iron dwellings called shacks. There are few formalized amenities like shops, clinics, schools, and recreation facilities. Recently however, there has been an effort to upgrade Nomzamo through the construction of permanent brick houses and electrification. Nonetheless, due to poverty, many residents continue to use wood and paraffin for cooking and space heating. Slovo Park, in contrast, has no electricity. Both communities are faced with high levels of overcrowding, unemployment, poverty, violence, and injury.891629
Intervention
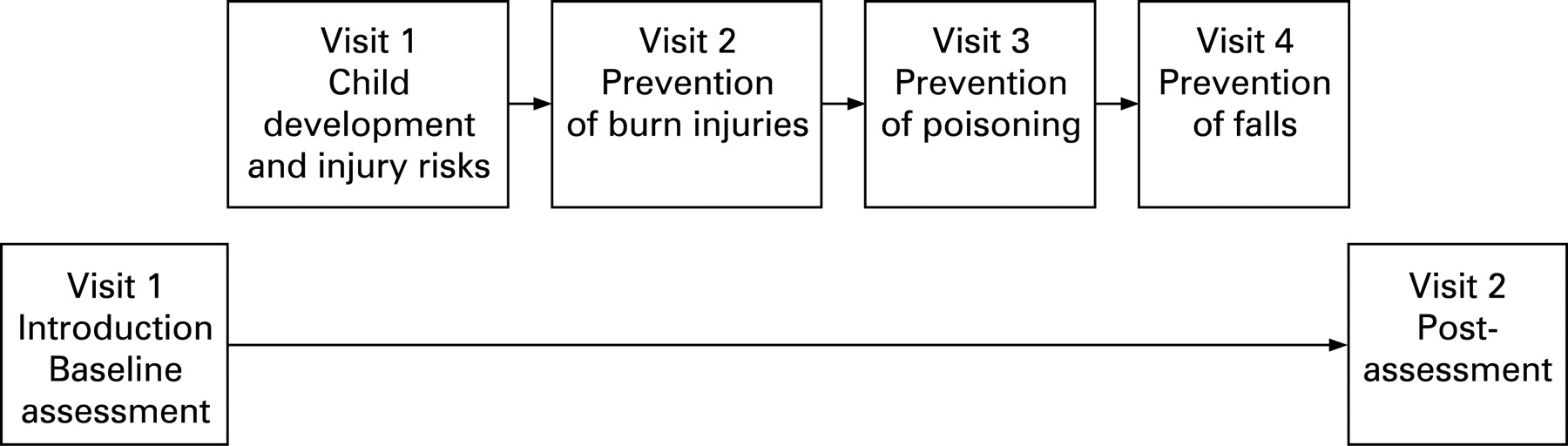
Home visitors called on the intervention households four times between October 2005 and February 2006. The control households were not visited (fig 1). The visits focused on child development and the prevention of burns, poisoning, and falls respectively. During each visit, home visitors provided caregivers (parent or primary caregiver) with information on safety practices, completed an injury hazard checklist with the caregiver, and discussed possible changes to reduce risks for child injuries. Caregivers were also given safety devices, such as child-proof locks and paraffin container safety caps, along with demonstrations on how they should be used. The cost of safety devices averaged ZAR5 (<US$1, £0.50, or €0.60) per visit. Each visit lasted approximately 40 minutes. Control households were given safety devices after the injury risk post-assessment.
Community residents were recruited to serve as home visitors. Some recruits had been involved with injury prevention work and acted as volunteers for a local safety promotion team.30 All recruits received training in unintentional injury prevention methods. A manual for the home visitors training was developed and tested by the research team during the pilot, and was further refined for this trial.31 Two site coordinators met with the home visiting teams daily to provide debriefing and supervision. Home visitors were paid ZAR30 (approximately US$4, £2, or €2.50) per visit. The manual can be downloaded at http://www.ishs.org.za from publications, and is also available on the Injury Prevention website.
Objective
To evaluate the effectiveness of the HVP in reducing hazards for burns, poison ingestion, and fall-related injuries for low-income neighborhood households with children aged ⩽10 years.
Outcome measures
A comprehensive evaluation was conducted prior to this trial to develop and validate an injury risk assessment instrument for the communities.32 The instrument collected information from the caregiver regarding household demographics, household safety hazards, and unintentional injuries sustained by children one year previously. The key outcomes developed to measure the presence of household hazards were scores for burns (safety practices, paraffin, and electrical), poisoning, and falls (table 1). Assessments were administered in the local languages relevant to the caregiver (English, Afrikaans, Xhosa, and Zulu). The injury risk assessment questionnaire can be downloaded at http://www.ishs.org.za from publications, and is also available on the Injury Prevention website.
Sample size
Using the home as the unit of analysis, we determined that to observe a 2-point reduction in home hazards (injury risk score) based on 80% power at α = 0.05 (two-sided) a sample of 100 was required for each of the intervention and control groups. To allow for the cluster design an inflation factor of 1.2, estimated from the pilot study, was used, indicating a sample size of 120 houses per intervention group.
Randomization
To minimize potential contamination by families talking to their neighbors about the program, we decided not to randomize individual households but rather to cluster the households into blocks and to randomize the blocks.
Community volunteers drew up maps demarcating all the property stands, stand numbers, roads, and facilities at each site. Blocks of households were demarcated on the maps, grouping geographically adjacent stands together so that there was maximal separation between blocks. Main streets, shops, and other recreational buildings separating blocks were also taken into account. A total of 28 blocks were demarcated in Nomzamo, and 26 blocks in Slovo Park. There were 48–99 houses per block in Nomzamo and 26–56 houses per block in Slovo Park. Two of the demarcated blocks in Slovo Park were excluded from the sampling because they were near a footbridge that presented a potential security risk for the home visitation team.
Data collectors were allocated at random to the blocks, but not to a block where they resided. They were given computer generated lists of all house numbers in each block, sorted in random order, and instructed to select houses from the top down until the required total of eligible households (those with children aged ⩽10) were recruited from each site. Before a home was considered non-participating it was visited at least three times. After obtaining informed written consent from participating homes, data collectors implemented the baseline injury risk assessment.
Thereafter, eligible blocks were randomly allocated to the intervention and control groups (14 each for Nomzamo and 12 each for Slovo Park). Two weeks after the final home visit, data collectors visited the intervention and control households to readminister the injury risk assessment. While data collectors were masked to group assignment at baseline, they might have been alerted to the intervention houses at post-intervention.
Statistical methods
The intervention effect was calculated using the post-intervention mean scores for the intervention households minus those obtained for the control households. A mixed-model analysis of variance, with random effects to reflect the correlation of observations among households in the same block, was conducted to assess whether the intervention effect was significantly different from zero, with 95% CIs. The mixed-model with unstructured correlational matrix was used and allowance was made for unequal variances for the two strata, Nomzamo and Slovo Park. An interaction was included in the mixed model to test if the uptake of the two sites was similar.
RESULTS
Participant flow
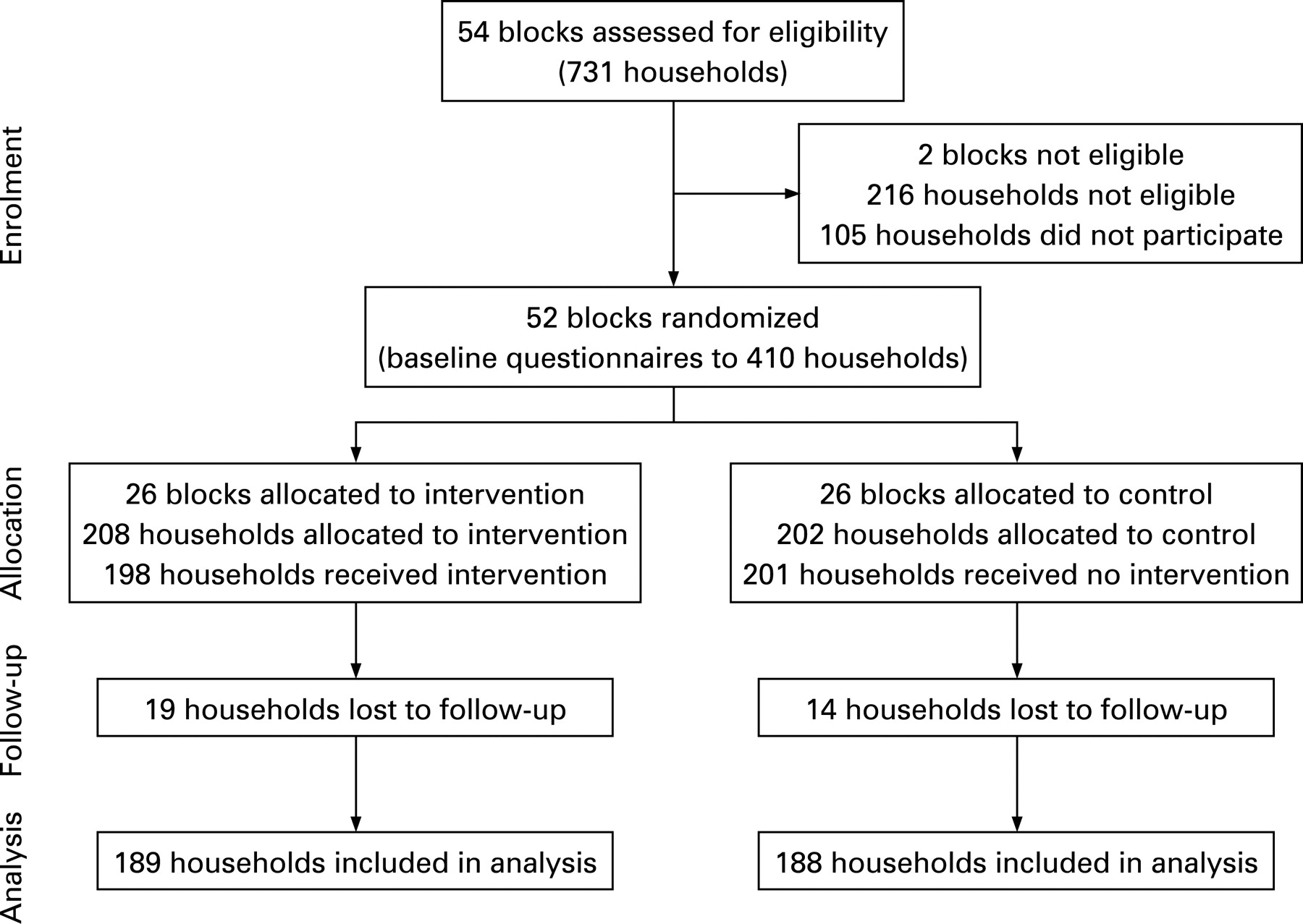
A total of 731 households were visited, of which 515 (70%) were eligible for study participation (fig 2). Of the eligible households, 410 (80%) participated. Reasons for non-participation included the unavailability of caregivers after three visits (13%) and refusal to participate in the study (10%). In Nomzamo, an average of 7 households participated per block, ranging from 3 to 11 households. In Slovo Park, an average of 8 households participated per block, ranging from 5 to 11 households. Follow-up data were available for 92% of the households.
{kind=link}
{kind=link}
Baseline data: sociodemographic profile and injury risks
The sociodemographic characteristics of the intervention and control households were similar except that more respondents from the intervention than control group were the children’s primary caretaker (table 2). The average age of the respondents was 34 years. Only a third of the respondents were employed.
At baseline, the risk profiles were similar for both groups (table 3). The average number of total risk items was 16 out of a possible 90 items for both groups.
Outcomes: impact of home visits on the risk profile
Table 3 shows the post-intervention comparisons between intervention and control groups for injury risk scores. All changes, as measured by the six risk scores, except for falls, were in a favorable direction as reflected by the total risk score in which the intervention households obtained a lower total injury risk mean score (13.9) than the control households (14.2). However, the intervention effect (IE) of −0.31 was not statistically significant (95% CI −1.18 to 1.2).
For burn-related electrical hazards, no statistically significant difference was noted at post-intervention between the intervention and control households (IE = −0.19, 95% CI −0.54 to 0.16). Differences between the intervention (3.2) and control (3.2) household scores for paraffin-related burn risks were also not significant (IE = −0.03, 95% CI −0.64 to −0.57). Statistically significant changes were observed for burn-related safety practices (IE = −0.41, 95% CI −0.76 to −0.07). Compared to control households (2.9), intervention households obtained a lower mean score (2.5), demonstrating their greater application of burn safety practices.
Although the intervention households obtained a lower mean score (1.9) for poisoning-related risks compared to the control households (2.4) at post-assessment, the effect was not statistically significant (IE = −0.45, 95% CI −1.01 to 0.11).
No significant difference was seen at post-intervention between the intervention (3.7) and control households (0 = 3.6) for fall-related risks (IE = 0.09, 95% CI −0.60 to 0.78).
The interactions to test for the differential uptake of the intervention in the two sites were not significant in any of the models, and were therefore excluded from the final model.
DISCUSSION
On a community level, our study revealed that HVP could effectively reduce home-based child injury risks for burns related to unsafe practices. Insignificant declines were however noted for the injury risks related to electrical burns, paraffin burns, and poison ingestion. No decline was observed for fall-related risks. The modest improvements over time between intervention and control groups may be contextualized within a range of constraining influences, such as recipient suspicion, home visitor selection and preparation, and home visitor attributes, all of which require further study.33
Strengths and weaknesses
Our study is one of the first randomized controlled trials assessing child unintentional injury risk reduction through home visitation in an LMIC. The study also points to the possibilities of deploying trained community residents to engage in home visits for the purposes of reducing child unintentional injury risks in underserved communities. Although it was slightly underpowered (by about 5%) as we were unable to recruit the number of houses required by the sampling scheme, our study demonstrated a small range of statistically significant differences between the intervention and control households. It is possible that, despite efforts to prevent treatment contamination through cluster randomization, the control group may have been alerted to some of the injury hazards during the pre-assessment and so may have corrected these by post-assessment, as is evident from all their lower post-mean compared to baseline scores.
Another limitation of our study, due to the small sample size and short study period, was that it assessed the reduction of injury hazards rather than injury occurrence. Moreover, the injury risks comprising the outcome measures were based on risks reported in the literature to have an association with injury outcomes or risks considered significant in low-income South African settings.33 Therefore, how the injury risk scores in our study explain or predict the actual occurrence of injury requires further investigation. The injury risk assessment tool also relied on observation which may have contributed to observer bias being introduced at follow-up.
Finally, our findings are limited by the characteristics of the two informal settlements and so may not be applicable to disadvantaged areas in other LMICs.
Comparisons with previous studies
Although the type of burn safety practices (table 1) in our study differed to that of HIC studies, as a consequence of the different housing circumstances, our findings are consistent with HIC studies that demonstrated the effectiveness of home visiting in improving burn safety practices.222425 Other studies evaluating the effectiveness of home safety education to reduce child burn risks due to the unsafe use of paraffin and appliances are scarce; hence further research in this area is important as paraffin remains a popular fuel for cooking in poor communities.34 Nevertheless, while education may contribute to the safe use and maintenance of paraffin appliances, engineering in the form of safe affordable design and enforcement of standards for paraffin-fuelled appliances is also crucial for the effective reduction of paraffin-related burn risks in the home.34
Unlike previous home visiting studies we did not find a significant reduction in electrical-related hazards, probably because of the minimal use of electrical appliances in the study communities, as indicated by the relatively low risk for electrical burns at baseline.192425
Although our study did not reveal a significant reduction for poisoning-related injury hazards, several households were shown to have benefitted from the intervention. Previous HIC home visiting programs have demonstrated a reduction in poisoning-related injury hazards, such as the safe storage of medicines and other harmful products, that may be attributable to the supply of safety devices.19222425 Our safety devices specifically included a child safety lock for cupboard doors and a child resistant container for the safe storage of paraffin. Research in low-income communities has demonstrated the effectiveness of child resistant containers in reducing the rate of paraffin ingestion by children.335 However, while the provision of safety devices might be necessary for the success of the program in low-income communities, education is also essential for the appropriate use of such devices.2434
In contrast to previous home visiting studies we did not find a reduction in fall-related hazards.2224 For example, Schwarz et al reported a reduction in tripping hazards (for example, loose rugs/floor coverings in particular rooms).24 Differences in dwelling features may account for the variance in results. The households in our study consisted primarily of one room shacks, wherein inadequate floor space arising from the clutter of furniture and the presence of several inhabitants contributed to fall risks. Therefore, the reduction of these fall-related hazards for children would require the provision of larger, formal housing.
Implications for prevention and research
Our findings suggest that home visits by trained lay workers who provide education, home inspection, and safety devices may contribute to child injury risk reduction in LMICs. However, the improvements in burn- and poisoning-related injury risk reduction over time between intervention and control groups were modest. Furthermore, no reduction in injury risks due to falls was noted. Therefore, prior to considering the program for integration into a comprehensive child injury prevention strategy, further replication and evaluation is required to assess the full utility of the HVP for low-income communities in other LMICs similar to South Africa. Furthermore, the influence of contextual factors on the implementation of home visitation, such as recipient suspicion, home visitor selection and preparation, and home visitor attributes also require further study. Ultimately, research in both HICs and LMICs must assess the impact of the program in terms of reduced injury rates, and should therefore include an analysis of the cost effectiveness of the program.
Key points
In low-income communities where professional expertise is scarce, residents can be trained to deliver child injury prevention interventions during home visits.
Home visits by paraprofessionals providing education, home inspection, and safety devices may contribute to child injury risk reduction, particularly burn-related injury.
Further replication and evaluation is required to assess the full utility of the home visitation program (HVP) for other low-income communities.
Apart from the reduction of home hazards, the HVP’s impact must also be assessed in terms of reduced injury rates.
REFERENCES
Supplementary materials
web only appendices 14/3/164
Files in this Data Supplement:
Footnotes
Competing interests: None.
▸ The manual and injury risk assessment questionnaire is published online only at http://injuryprevention.bmj.com/content/vol14/issue3